Learning Outcome
- Recall the presentation of Hodgkin lymphoma
- Summarize the treatment of Hodgkin lymphoma
- Discuss the complications of treatment of Hodgkin lymphoma
- List the nurse's role in managing patients with Hodgkin lymphoma

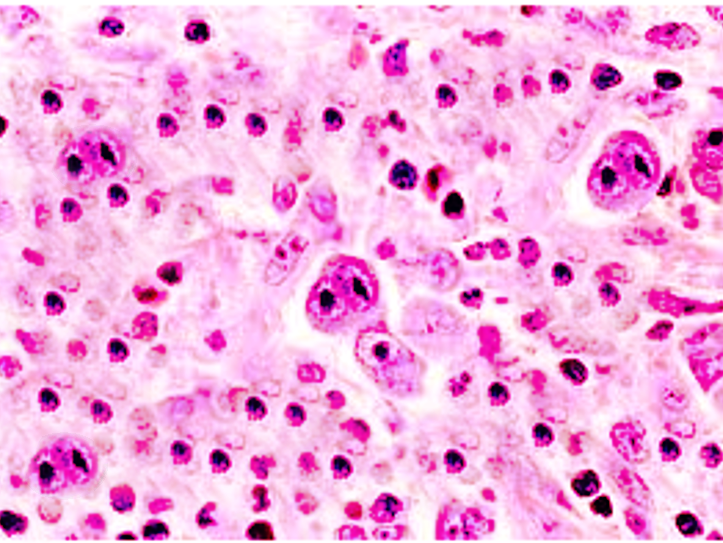
Hodgkin lymphoma (HL), formerly called Hodgkin's disease, is a rare monoclonal lymphoid neoplasm with high cure rates. Biological and clinical studies have divided this disease entity into two distinct categories: classical Hodgkin lymphoma and nodular lymphocyte-predominant Hodgkin lymphoma (NLP-HL). These two disease entities show differences in the clinical picture and pathology. Classical Hodgkin lymphoma accounts for approximately 95% of all HL, and it is further subdivided into four subgroups: nodular sclerosis (NSHL), lymphocyte-rich (LRHL), mixed cellularity (MCHL), and lymphocyte-depleted (LDHL). Four features characterize Hodgkin lymphomas. They commonly arise in the cervical lymph nodes; the disease is more common in young adults; there are scattered large mononuclear Hodgkin and multinucleated cells (Reed-Sternberg) intermixed in a background of a mixture of non-neoplastic inflammatory cells; finally, T lymphocytes are often observed surrounding the characteristic neoplastic cells. Hodgkin lymphoma has an excellent overall prognosis with approximately an 80% cure rate.[1][2][3]
The exact etiology of Hodgkin lymphoma is unknown. However, there is an increased risk of Hodgkin lymphoma in Epstein-Barr (EBV) infection, autoimmune diseases, and immunosuppression. There is also evidence of familial predisposition in Hodgkin lymphoma. EBV has been found to be more common in the mixed cellularity and lymphocyte depleted subtypes of Hodgkin lymphoma. Loss of immune surveillance has been proposed as the possible disease etiology in EBV-positive disease. No other virus has been found to play a major contributing role in disease pathogenesis. Immunosuppression secondary to a solid organ or hematopoietic cell transplantation, therapy with immunosuppressive drugs, and human immunodeficiency (HIV) infection have all a higher risk of developing Hodgkin lymphoma. HIV patients commonly present with a more advanced stage, unusual lymph nodes sites, and a poor prognosis. Studies found that there is a ten-fold increase of developing HL in same-sex siblings of patients with Hodgkin lymphoma, suggesting a gene-environment interaction role in Hodgkin lymphoma predisposition.[4][5][6]
The exact etiology of Hodgkin lymphoma is unknown. However, there is an increased risk of Hodgkin lymphoma in Epstein-Barr (EBV) infection, autoimmune diseases, and immunosuppression. There is also evidence of familial predisposition in Hodgkin lymphoma. EBV has been found to be more common in the mixed cellularity and lymphocyte depleted subtypes of Hodgkin lymphoma. Loss of immune surveillance has been proposed as the possible disease etiology in EBV-positive disease. No other virus has been found to play a major contributing role in disease pathogenesis. Immunosuppression secondary to a solid organ or hematopoietic cell transplantation, therapy with immunosuppressive drugs, and human immunodeficiency (HIV) infection have all a higher risk of developing Hodgkin lymphoma. HIV patients commonly present with a more advanced stage, unusual lymph nodes sites, and a poor prognosis. Studies found that there is a ten-fold increase of developing HL in same-sex siblings of patients with Hodgkin lymphoma, suggesting a gene-environment interaction role in Hodgkin lymphoma predisposition.[4][5][6]
Patients with Hodgkin lymphoma frequently present with painless supra-diaphragmatic lymphadenopathy (one to two lymph node areas), B symptoms including unexplained profound weight loss, high fevers, and drenching night sweats. B symptoms are evident in up to 30% of patients and are generally more common in stage 3 to 4 of the disease, mixed cellularity, and lymphocyte depleted HL subtypes. Pain in lymph nodes may occur with alcohol consumption (paraneoplastic symptom). Chronic pruritus is another disease symptom that may be encountered. If mediastinal nodes enlargement is significant, the mass effect can produce chest pain and shortness of breath. If the patient has an extra-nodal disease, which is less common, related clinical manifestations may occur.
Each subtype of Hodgkin lymphoma has distinct clinical features. Nodular sclerosis subtype affects young adults and presents with early disease stage, while mixed cellularity HL is prevalent in both children and elderly patients and commonly presents with advanced disease stage. Lymphocyte depletion HL presents with extensive extranodal disease, affects elderly patients, and is associated with AIDS infection. Lymphocyte-rich classical HL presents with localized painless peripheral lymphadenopathy similar to NLP-HL. NLP-HL is a distinct, unique clinicopathological entity that is distinct from classical HL. It presents in males with localized painless peripheral lymphadenopathy in the neck that often spares the mediastinum. NLP-HL shows a more indolent course with a tendency for late relapses.[7][8][9]
Definitive diagnosis for Hodgkin lymphoma is through biopsy from a lymph node or suspected organ. It is important to note that fine-needle aspiration or core-needle biopsy frequently show non-specific findings because of the low ratio of malignant cells and loss of architectural information. So excisional biopsy should be pursued if suspicion of Hodgkin lymphoma is high. An RS cell or LP cell need to be identified within the biopsy specimen to establish a definitive diagnosis. Further workup is essential to determine the stage, which guides treatment and provide prognostic information.
Laboratory tests include complete blood count (CBC), complete metabolic panel (CMP), erythrocyte sedimentation rate, Hepatitis B virus, hepatitis C virus, and HIV.
LDH levels correlate with the bulk of disease. Elevated levels of alkaline phosphatase may suggest liver or bone involvement. Testing for HIV is recommended as the treatment of the infection can improve outcomes in HIV positive individuals.
Chest x-ray, CT chest/abdomen/pelvis, and PET/CT scans can help with staging. PET-CT scanning has now become a standard test for assessment of treatment response in HL and most lymphomas. Overall, a comprehensive workup is essential for both diagnosis and staging of Hodgkin lymphoma.
Treatment of Hodgkin lymphoma largely depends on the histologic characteristics, the stage of the disease, and the presence or absence of prognostic factors. The goal of treatment for patients with Hodgkin lymphoma is to cure the disease with control of short and long-term complications. There are several different staging systems for Hodgkin lymphoma, and the Cotswolds modified Ann Arbor classification is commonly used. The International Prognostic Factors Project on Advanced Hodgkin's lymphoma identified 7 variables for patients with advanced disease:
Risk stratification categorizes patients as low risk or high risk for recurrence. The response to therapy is determined by PET scan and is used to optimize therapy. The initial treatment of Hodgkin lymphoma depends on subgroup treatment. There are three treatment subgroups: patients with the early-stage disease with favorable prognostic factors, patients with the limited-stage disease who have unfavorable prognostic factors, and those with advanced-stage disease. Patients who are in early-stage (stage I to IIA) with favorable prognostic features are treated with short duration of chemotherapy, typically two cycles of ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) followed by restricted involved-field radiation therapy (IFRT).
Patients who are in limited-stage disease but with unfavorable features such as bulky mediastinal disease, elevated ESR, and extra-nodal extension are treated with a longer course of chemotherapy (4 to 6 cycles) followed by a higher dose of IFRT. Patients with advanced-stage (stage IIB to IV) are risk-stratified by a different scoring system, the International Prognostic Score (IPS). Depending on IPS, different chemotherapy regimens (for example, escalated BEACOPP and Stanford V) can be used, but the standard of care is ABVD for most patients.
Radiation, in general, is not beneficial in these patients. Despite the high cure rate with initial therapy, approximately 10% of patients with Hodgkin lymphoma are refractory to initial treatment, and up to 30% of patients will relapse after achieving an initial complete remission. High-dose chemotherapy, followed by an autologous stem cell transplant is the standard of care for the majority of patients who are refractory or relapse post-initial therapy. For patients who fail autologous transplantation treatment options include: brentuximab vedotin, PD-1 blockade, non-myeloablative allogeneic transplantation, or clinical trials. Future directions in the management of Hodgkin lymphoma will include the incorporation of frontline therapeutics that have shown efficacy in refractory/relapses disease setting as well as other possible novel therapeutics.[10][11][12][13]
Hematopoietic stem cell transplantation is done in refractory or relapsed patients.
Hodgkin lymphoma is a systemic disorder that is best managed by an interprofessional team for best outcomes.
The management of Hodgkin lymphoma is primarily by the oncologists. However, the patient may first present to the primary care provider or nurse practitioner with symptoms suggestive of the lymphoma. The key is prompt referral so that therapy can be initiated.
Treatment of Hodgkin lymphoma largely depends on the histologic characteristics, the stage of the disease, and the presence or absence of prognostic factors. The goal of treatment for patients with Hodgkin lymphoma is to cure the disease with control of short and long-term complications.
The pharmacist has to educate the patient on the drugs, their benefits, and side effect profile. In addition, the pharmacist has to ensure that the patient has had the recommended preoperative workup before dispensing the drugs. The oncology nurse should monitor the patient for acute side effects of the chemotherapeutic drugs and educate the patient on minimizing complications.
Because many patients develop anxiety and depression, a mental health provider should provide appropriate counseling.
The dietitian should be involved in educating the patient on foods to eat and what to avoid.
The interprofessional team has to meet on a weekly basis to discuss patient care and future therapy. The communication between the members should be clear and open to ensure that the patient's treatment has not been jeopardized. Finally, if the patient is terminal, a hospice care team should be involved.
Outcomes
Prognosis depends on several prognostic factors, including disease stage. Disease stage is currently only one factor in the prognostic indices used for pretreatment risk stratification and assessment. The 5-year overall survival (OS) in stage 1 or 2a is approximately 90%; on the other hand, stage 4 disease has a 5-year OS of approximately 60%.[14][15](Level 5)
Hodgkin lymphoma is a systemic disorder that is best managed by an interprofessional team for best outcomes.
The management of Hodgkin lymphoma is primarily by the oncologists. However, the patient may first present to the primary care provider or nurse practitioner with symptoms suggestive of the lymphoma. The key is prompt referral so that therapy can be initiated.
Treatment of Hodgkin lymphoma largely depends on the histologic characteristics, the stage of the disease, and the presence or absence of prognostic factors. The goal of treatment for patients with Hodgkin lymphoma is to cure the disease with control of short and long-term complications.
The pharmacist has to educate the patient on the drugs, their benefits and side effect profile. In addition, the pharmacist has to ensure that the patient has had the recommended preoperative workup before dispensing the drugs. The oncology nurse should monitor the patient for acute side effects of the chemotherapeutic drugs and educate the patient on minimizing complications.
Because many patients develop anxiety and depression, a mental health nurse should provide appropriate counseling.
The dietitian should be involved in educating the patient on foods to eat and what to avoid.
The interprofessional team has to meet on a weekly basis to discuss patient care and future therapy. The communication between the members should be clear and open to ensure that the patient's treatment has not been jeopardized. Finally, if the patient is terminal a hospice care team should be involved.
Lees C, Keane C, Gandhi MK, Gunawardana J. Biology and therapy of primary mediastinal B-cell lymphoma: current status and future directions. British journal of haematology. 2019 Apr:185(1):25-41. doi: 10.1111/bjh.15778. Epub 2019 Feb 10 [PubMed PMID: 30740662]
Amraee A, Evazi MR, Shakeri M, Roozbeh N, Ghazanfarpour M, Ghorbani M, Ansari J, Darvish L. Efficacy of nivolumab as checkpoint inhibitor drug on survival rate of patients with relapsed/refractory classical Hodgkin lymphoma: a meta-analysis of prospective clinical study. Clinical & translational oncology : official publication of the Federation of Spanish Oncology Societies and of the National Cancer Institute of Mexico. 2019 Aug:21(8):1093-1103. doi: 10.1007/s12094-018-02032-4. Epub 2019 Feb 9 [PubMed PMID: 30739242]
Metzger ML, Mauz-Körholz C. Epidemiology, outcome, targeted agents and immunotherapy in adolescent and young adult non-Hodgkin and Hodgkin lymphoma. British journal of haematology. 2019 Jun:185(6):1142-1157. doi: 10.1111/bjh.15789. Epub 2019 Feb 6 [PubMed PMID: 30729493]
PDQ Pediatric Treatment Editorial Board. Childhood Hodgkin Lymphoma Treatment (PDQ®): Health Professional Version. PDQ Cancer Information Summaries. 2002:(): [PubMed PMID: 26389170]
Milgrom SA, Elhalawani H, Lee J, Wang Q, Mohamed ASR, Dabaja BS, Pinnix CC, Gunther JR, Court L, Rao A, Fuller CD, Akhtari M, Aristophanous M, Mawlawi O, Chuang HH, Sulman EP, Lee HJ, Hagemeister FB, Oki Y, Fanale M, Smith GL. A PET Radiomics Model to Predict Refractory Mediastinal Hodgkin Lymphoma. Scientific reports. 2019 Feb 4:9(1):1322. doi: 10.1038/s41598-018-37197-z. Epub 2019 Feb 4 [PubMed PMID: 30718585]
Lyapichev KA, You MJ. Unusual presentation of classic Hodgkin lymphoma. Blood. 2019 Jan 31:133(5):502. doi: 10.1182/blood-2018-10-878058. Epub [PubMed PMID: 30705049]
Justiz Vaillant AA, Stang CM. Lymphoproliferative Disorders. StatPearls. 2024 Jan:(): [PubMed PMID: 30725847]
Gaut D, Schiller GJ. Hematopoietic stem cell transplantation in primary central nervous system lymphoma: a review of the literature. International journal of hematology. 2019 Mar:109(3):260-277. doi: 10.1007/s12185-019-02594-1. Epub 2019 Jan 22 [PubMed PMID: 30671909]
Cai Q, Fang Y, Young KH. Primary Central Nervous System Lymphoma: Molecular Pathogenesis and Advances in Treatment. Translational oncology. 2019 Mar:12(3):523-538. doi: 10.1016/j.tranon.2018.11.011. Epub 2019 Jan 4 [PubMed PMID: 30616219]
Hoppe RT, Advani RH, Ai WZ, Ambinder RF, Aoun P, Armand P, Bello CM, Benitez CM, Bierman PJ, Chen R, Dabaja B, Dean R, Forero A, Gordon LI, Hernandez-Ilizaliturri FJ, Hochberg EP, Huang J, Johnston PB, Kaminski MS, Kenkre VP, Khan N, Maddocks K, Maloney DG, Metzger M, Moore JO, Morgan D, Moskowitz CH, Mulroney C, Rabinovitch R, Seropian S, Tao R, Winter JN, Yahalom J, Burns JL, Ogba N. NCCN Guidelines Insights: Hodgkin Lymphoma, Version 1.2018. Journal of the National Comprehensive Cancer Network : JNCCN. 2018 Mar:16(3):245-254. doi: 10.6004/jnccn.2018.0013. Epub [PubMed PMID: 29523663]
Gordon LI. Strategies for Management of Relapsed or Refractory Hodgkin Lymphoma. Journal of the National Comprehensive Cancer Network : JNCCN. 2017 May:15(5S):716-718 [PubMed PMID: 28515253]
Klimm B, Goergen H, Fuchs M, von Tresckow B, Böll B, Meissner J, Glunz A, Diehl V, Eich HT, Engert A, Borchmann P. Impact of risk factors on outcomes in early-stage Hodgkin's lymphoma: an analysis of international staging definitions. Annals of oncology : official journal of the European Society for Medical Oncology. 2013 Dec:24(12):3070-6. doi: 10.1093/annonc/mdt413. Epub 2013 Oct 22 [PubMed PMID: 24148816]
Hoppe RT, Advani RH, Ai WZ, Ambinder RF, Aoun P, Bello CM, Bierman PJ, Blum KA, Chen R, Dabaja B, Duron Y, Forero A, Gordon LI, Hernandez-Ilizaliturri FJ, Hochberg EP, Maloney DG, Mansur D, Mauch PM, Metzger M, Moore JO, Morgan D, Moskowitz CH, Poppe M, Pro B, Winter JN, Yahalom J, Sundar H, National Comprehensive Cancer Network. Hodgkin lymphoma, version 2.2012 featured updates to the NCCN guidelines. Journal of the National Comprehensive Cancer Network : JNCCN. 2012 May:10(5):589-97 [PubMed PMID: 22570290]
Chihara D, Oki Y, Fanale MA, Westin JR, Nastoupil LJ, Neelapu S, Fayad L, Fowler NH, Cheah CY. Stage I non-Hodgkin lymphoma: no plateau in disease-specific survival ? Annals of hematology. 2019 May:98(5):1169-1176. doi: 10.1007/s00277-018-3571-7. Epub 2019 Jan 8 [PubMed PMID: 30617643]
Ramchandren R, Advani RH, Ansell SM, Bartlett NL, Chen R, Connors JM, Feldman T, Forero-Torres A, Friedberg JW, Gopal AK, Gordon LI, Kuruvilla J, Savage KJ, Younes A, Engley G, Manley TJ, Fenton K, Straus DJ. Brentuximab Vedotin plus Chemotherapy in North American Subjects with Newly Diagnosed Stage III or IV Hodgkin Lymphoma. Clinical cancer research : an official journal of the American Association for Cancer Research. 2019 Mar 15:25(6):1718-1726. doi: 10.1158/1078-0432.CCR-18-2435. Epub 2019 Jan 7 [PubMed PMID: 30617130]