
Introduction
Carpal tunnel syndrome (CTS) is a common ailment affecting the general patient population. It is the most common cause of peripheral nerve compression, with an incidence of 99 in 100,000 people. CTS is most commonly seen in patients over 40 years of age and has a greater prevalence in women, as they comprise approximately 65% to 75% of all reported cases [1]. CTS results from compression of the median nerve within the carpal tunnel in the wrist.[2] Typically, the pressure within the carpal tunnel in these patients can be 32 to 110 mm Hg compared to 2 to 31 mm Hg in normal patients.[3] The compression of the median nerve causes the classic pain distribution and/or paresthesias seen in CTS on the palmar aspect of the hand. The classic distribution involves the area innervated by the median nerve, including the volar aspect of the thumb, index finger, long finger, and the radial volar half of the ring finger. Risk factors for the development of CTS include obesity, pregnancy (especially later in pregnancy), age, trauma to the wrist, and inflammatory rheumatic disorders.[4] Controversy exists whether or not overuse is a contributing factor (such as daily typing). Conservative treatment options include keeping the wrist immobile using wrist splints, physiotherapy, and pain medications, both topically and systemically.[5] More invasive options include local steroid injections to the carpal tunnel and surgical decompression of the space. This article will focus on injection techniques for CTS.
The exact etiology of CTS is not completely known, but the condition is largely assumed to be idiopathic or multifactorial. Some of the suspected risk factors for CTS include diabetes mellitus type 1 or 2, hypothyroidism, menopause, obesity, arthritis, and age.[6] Diabetes seems to have the greatest association with CTS, with a prevalence rate of 30% in patients with diabetic neuropathy and 14% in patients without neuropathic symptoms.[7] Hormonal changes may be a contributing factor since pregnancy, menopause, and hypothyroidism are associated with CTS. Mechanical risk factors, including inflammation, thickening, arthritic deformity, and bony irregularities, contribute to median nerve compression.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The carpal tunnel is located in the volar aspect of the wrist between the carpal bones and flexor retinaculum.[8] The boundaries of the carpal tunnel include the floor of carpal bones and the roof formed by the flexor retinaculum. The carpal tunnel contains the median nerve as well as 9 tendons (flexor pollicis longus, 4 flexor digitorum superficialis, and 4 flexor digitorum profundus). Increased pressure within the tunnel causes pain in the distribution of the median nerve within the hand. The median nerve is formed by a confluence of the medial and lateral cords of the brachial plexus. The nerve supplies motor innervation to the thenar muscles and sensory innervation to the radial 3.5 fingers. The median nerve supplies sensation to the radial half of the fourth finger. The ulnar nerve supplies sensation to the ulnar (or medial) half of the fourth finger.
Indications
Most patients are indicated for a carpal tunnel injection after failing conservative therapies, including wrist immobilization, physical therapy, and oral analgesic medications. When electromyography/nerve conduction velocity results are equivocal, carpal tunnel injections may also be considered preoperatively to confirm the diagnosis of carpal tunnel syndrome.
Contraindications
Some of the contraindications to carpal tunnel injections include patient refusal, infection over the injection site, and edema at the injection site. Patients on anticoagulation may undergo carpal tunnel injections, but with careful evaluation for bleeding.
Technique or Treatment
Many patients turn to injections for their CTS when conservative therapies fail. Corticosteroid solutions are the predominant injectate used. Controversy exists over the safest injection site. A comparative study of several locations found that injecting within the flexor carpi radialis tendon proximal to the carpal tunnel might be the safest.[9] The in-plane ulnar approach has been shown to be superior to the proximal approach for improving symptom severity.[10]
The patient may be seated or supine during the injection. The affected wrist is supinated in slight dorsiflexion using a rolled-up towel and taping the fingers down. An ultrasound linear array probe can be used to scan the wrist for any anatomical variants, such as volar ganglion cysts, flexor tendon tenosynovitis, and tumors.[11] The probe is then placed transversely at the proximal wrist crease by the entrance to the carpal tunnel. The goal is to have the pisiform, ulnar nerve, and ulnar artery in view as well as the median nerve. Doppler imaging can aid in determining vascular structures. The median nerve is identified and most often edematous. The injectate is targeted around the nerve in a target sign. The subsynovial tissue may also be injected, which has recently been implicated as the etiology of idiopathic CTS.[12]
Using a sterile technique, the needle is introduced most commonly on the ulnar aspect of the carpal tunnel. The initial trajectory is shallow and superficial to the ulnar artery and nerve penetrating the flexor retinaculum.[13] The anterior aspect of the medial side of the nerve is injected first. The nerve should separate from the flexor retinaculum located anteriorly. This hydrodissection should reduce any adhesions which may have caused entrapment. The needle is then redirected deeper on the ulnar side to inject the posterior aspect. The nerve should be completely surrounded by the injectate and “floating” in the solution.
Study results have shown that 75% of corticosteroid injections were accurately placed solely using landmarks, while 8.7% penetrated and damaged the median nerve.[14] Ultrasound guidance has been proven to reduce adverse events significantly. Meta-analysis also showed significant improvement in CTS severity using ultrasound guidance in 12 weeks compared to landmark-guided injections.[15]
Platelet-rich plasma (PRP) injections have recently risen as a new modality for long-lasting pain relief. PRP contains concentrated platelets and growth factors that have been shown to alleviate CTS symptomatology. PRP promotes axonal regeneration, thereby restoring the function of the median nerve. A systemic review of 5 studies, including 3 randomized controlled trials, one case-control, and one case report, showed the efficacy of PRP for patients with mild CTS.[16] More extensive studies need to be performed to show the benefit of PRP injections for CTS.
Complications
The following complications may arise during qa carpal tunnel injection:
- Bleeding
- Elevated blood glucose levels
- Infection
- Median nerve injury
- Pain
- Paresthesias
Clinical Significance
The symptomatology of patients with CTS often develops insidiously over the course of months, years, or even decades. One of the most common symptoms is a “pins and needles” sensation in the first three fingers (thumb, index, and middle fingers) and nocturnal pain in the hand.[17] As the condition progresses, patients often experience intermittent pain and numbness in the affected area during daytime activities like driving, lifting, or using the computer.[17] Over time, patients complain primarily of constant pain and even swelling of the affected hand and thenar atrophy. On physical exam, practitioners may be able to see thenar wasting, indicating extensive CTS.
Tinel’s and Phalen’s tests are in-office maneuvers doctors may ask patients to perform to apply stress to the median nerve at the wrist.[17] A positive Tinel’s sign is elicited when percussing the carpal tunnel evokes the patient’s symptomatology. Phalen sign (or prayer sign) can be seen with forced wrist flexion or hyperextension for one minute. See Image. Carpal Tunnel Physical Exam. The diagnosis is most often made clinically, but many agree that nerve conduction studies are the gold standard for diagnosing.[18] The one drawback of nerve conduction testing is putting the patient through undue pain and stress.
Enhancing Healthcare Team Outcomes
Carpal tunnel syndrome poses a unique challenge to doctors in many specialties. As the most common peripheral nerve entrapment syndrome, it is extremely prevalent throughout the population. Wrist and hand pain, in general, can have a myriad of etiologies, including DeQuervain tenosynovitis, trigger finger, gout, and carpal tunnel syndrome. Wrist and hand pain can even be referred from the neck in cervical radiculopathy or even from a cardiac condition like myocardial infarction.
Usually, a primary care practitioner is the first person a patient sees with carpal tunnel syndrome. This provider may start conservative therapies, but for more advanced treatment options, proper coordination with a pain management doctor, rheumatologist, or orthopedist is needed. Radiologists play a vital role as well to rule out potential fractures or dislocations at the wrist after trauma. In the office setting, many pain physicians will need a team of nurse practitioners to help during the procedure to maintain sterility and help with ultrasound guidance throughout the injection. Proper coordination of care through different medical professionals gives patients with carpal tunnel syndrome the best chance at resolving their symptomatology.
Media
(Click Image to Enlarge)
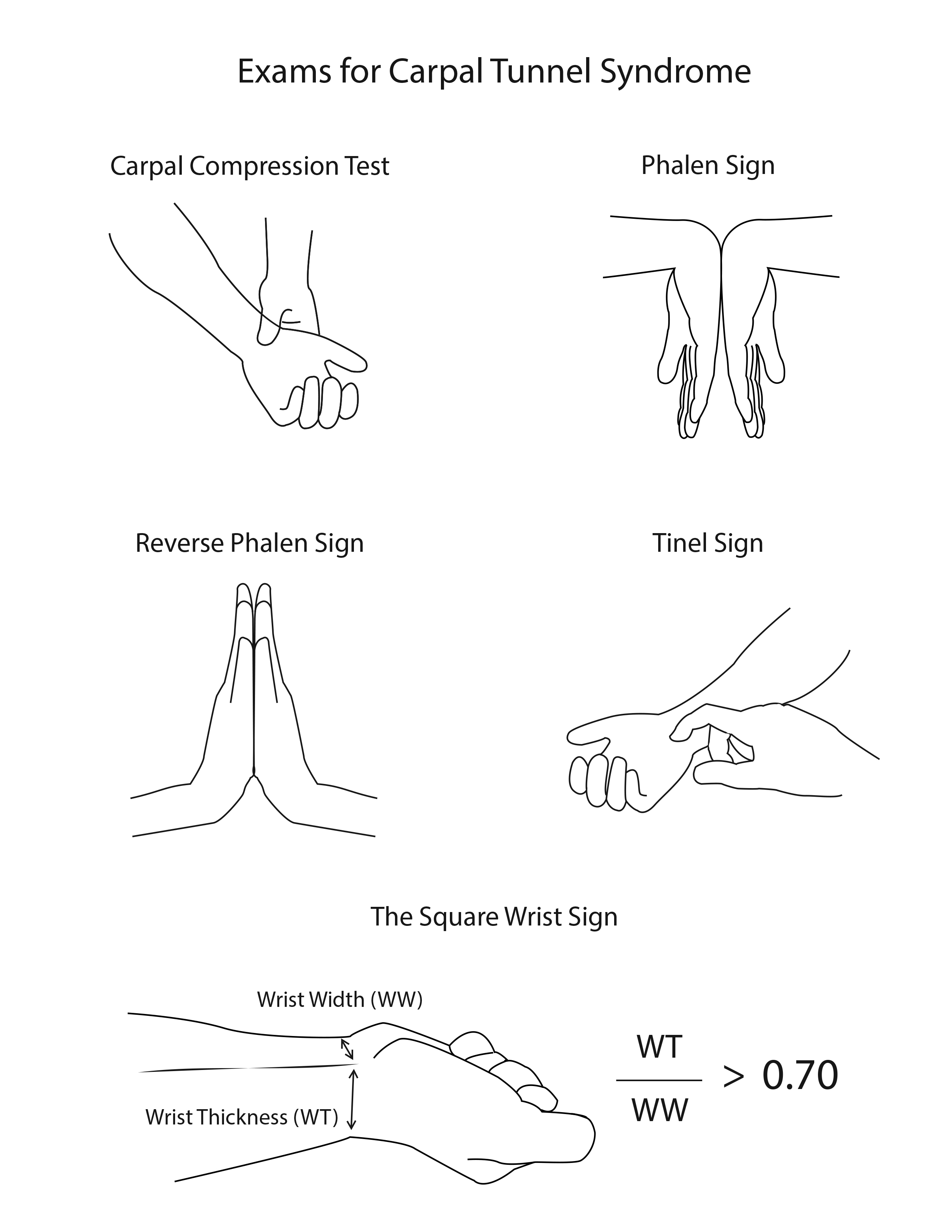
Carpal Tunnel Physical Exam. The illustration depicts some maneuvers that test for carpal tunnel syndrome.
Contributed by R Kabir, MD
References
Gillig JD, White SD, Rachel JN. Acute Carpal Tunnel Syndrome: A Review of Current Literature. The Orthopedic clinics of North America. 2016 Jul:47(3):599-607. doi: 10.1016/j.ocl.2016.03.005. Epub [PubMed PMID: 27241382]
Bland JD. Carpal tunnel syndrome. BMJ (Clinical research ed.). 2007 Aug 18:335(7615):343-6 [PubMed PMID: 17703044]
Gelberman RH, Hergenroeder PT, Hargens AR, Lundborg GN, Akeson WH. The carpal tunnel syndrome. A study of carpal canal pressures. The Journal of bone and joint surgery. American volume. 1981 Mar:63(3):380-3 [PubMed PMID: 7204435]
Solomon DH,Katz JN,Bohn R,Mogun H,Avorn J, Nonoccupational risk factors for carpal tunnel syndrome. Journal of general internal medicine. 1999 May; [PubMed PMID: 10337041]
Level 2 (mid-level) evidenceBickel KD. Carpal tunnel syndrome. The Journal of hand surgery. 2010 Jan:35(1):147-52. doi: 10.1016/j.jhsa.2009.11.003. Epub [PubMed PMID: 20117319]
Padua L, Coraci D, Erra C, Pazzaglia C, Paolasso I, Loreti C, Caliandro P, Hobson-Webb LD. Carpal tunnel syndrome: clinical features, diagnosis, and management. The Lancet. Neurology. 2016 Nov:15(12):1273-1284. doi: 10.1016/S1474-4422(16)30231-9. Epub 2016 Oct 11 [PubMed PMID: 27751557]
Sharma D, Jaggi AS, Bali A. Clinical evidence and mechanisms of growth factors in idiopathic and diabetes-induced carpal tunnel syndrome. European journal of pharmacology. 2018 Oct 15:837():156-163. doi: 10.1016/j.ejphar.2018.08.017. Epub 2018 Aug 17 [PubMed PMID: 30125568]
Presazzi A,Bortolotto C,Zacchino M,Madonia L,Draghi F, Carpal tunnel: Normal anatomy, anatomical variants and ultrasound technique. Journal of ultrasound. 2011 Mar; [PubMed PMID: 23396809]
Racasan O, Dubert T. The safest location for steroid injection in the treatment of carpal tunnel syndrome. Journal of hand surgery (Edinburgh, Scotland). 2005 Aug:30(4):412-4 [PubMed PMID: 15950338]
Chen PC, Chuang CH, Tu YK, Bai CH, Chen CF, Liaw M. A Bayesian network meta-analysis: Comparing the clinical effectiveness of local corticosteroid injections using different treatment strategies for carpal tunnel syndrome. BMC musculoskeletal disorders. 2015 Nov 19:16():363. doi: 10.1186/s12891-015-0815-8. Epub 2015 Nov 19 [PubMed PMID: 26585378]
Level 1 (high-level) evidenceWong SM, Griffith JF, Hui AC, Lo SK, Fu M, Wong KS. Carpal tunnel syndrome: diagnostic usefulness of sonography. Radiology. 2004 Jul:232(1):93-9 [PubMed PMID: 15155897]
Oh S, Belohlavek M, Zhao C, Osamura N, Zobitz ME, An KN, Amadio PC. Detection of differential gliding characteristics of the flexor digitorum superficialis tendon and subsynovial connective tissue using color Doppler sonographic imaging. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2007 Feb:26(2):149-55 [PubMed PMID: 17255175]
Green DP, MacKay BJ, Seiler SJ, Fry MT. Accuracy of Carpal Tunnel Injection: A Prospective Evaluation of 756 Patients. Hand (New York, N.Y.). 2020 Jan:15(1):54-58. doi: 10.1177/1558944718787330. Epub 2018 Jul 13 [PubMed PMID: 30003816]
Smith J, Wisniewski SJ, Finnoff JT, Payne JM. Sonographically guided carpal tunnel injections: the ulnar approach. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2008 Oct:27(10):1485-90 [PubMed PMID: 18809959]
Level 1 (high-level) evidenceBabaei-Ghazani A, Roomizadeh P, Forogh B, Moeini-Taba SM, Abedini A, Kadkhodaie M, Jahanjoo F, Eftekharsadat B. Ultrasound-Guided Versus Landmark-Guided Local Corticosteroid Injection for Carpal Tunnel Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Archives of physical medicine and rehabilitation. 2018 Apr:99(4):766-775. doi: 10.1016/j.apmr.2017.08.484. Epub 2017 Sep 21 [PubMed PMID: 28943161]
Level 1 (high-level) evidenceMalahias MA, Chytas D, Mavrogenis AF, Nikolaou VS, Johnson EO, Babis GC. Platelet-rich plasma injections for carpal tunnel syndrome: a systematic and comprehensive review. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie. 2019 Jan:29(1):1-8. doi: 10.1007/s00590-018-2278-8. Epub 2018 Jul 18 [PubMed PMID: 30022241]
Level 1 (high-level) evidenceArnold WD, Elsheikh BH. Entrapment neuropathies. Neurologic clinics. 2013 May:31(2):405-24. doi: 10.1016/j.ncl.2013.01.002. Epub 2013 Feb 8 [PubMed PMID: 23642716]
Level 3 (low-level) evidenceKeith MW, Masear V, Chung K, Maupin K, Andary M, Amadio PC, Barth RW, Watters WC 3rd, Goldberg MJ, Haralson RH 3rd, Turkelson CM, Wies JL. Diagnosis of carpal tunnel syndrome. The Journal of the American Academy of Orthopaedic Surgeons. 2009 Jun:17(6):389-96 [PubMed PMID: 19474448]