Introduction
The thalamus is a mostly gray matter structure of the diencephalon that has many essential roles in human physiology. The thalamus is composed of different nuclei that each serve a unique role, ranging from relaying sensory and motor signals, as well as regulation of consciousness and alertness. Clinically, there are only a few conditions related to thalamic damage and dysfunction. Most of these conditions are rare, but some of the more common conditions have significant anatomical changes that are visible with neuroimaging. Surgical interventions of the thalamus in the past have had limitations, but currently, this field is evolving due to increased accessibility through the advancement of microsurgical techniques and improved neuroimaging.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The thalamus is a paired gray matter structure of the diencephalon located near the center of the brain. It is above the midbrain or mesencephalon, allowing for nerve fiber connections to the cerebral cortex in all directions — each thalamus connects to the other via the interthalamic adhesion. The thalamus forms the upper and lateral walls of the third ventricle while the dorsal surface is part of the floor of the body of the lateral ventricle. Laterally, the thalamus limits with the posterior arm of the internal capsule. Anterolaterally, it limits with the head of the caudate and ventral nucleus with the subthalamus and hypothalamus.
While the thalamus is mostly gray matter (cell bodies of neurons), there are some areas of white matter (axons). The external and internal medullary laminae are white matter structures of the thalamus. The external medullary laminae cover the lateral surface of the thalamus, and the internal medullary laminae divide the thalamic nuclei into anterior, medial, and lateral groups.[1]
The thalamus is made up of a series of nuclei which are responsible for the relay of the different sensory signals. These nuclei are formed mainly by neurons of excitatory and inhibitory nature. The thalamocortical neurons receive sensory or motor information from the rest of the body and present selected information via nerve fibers (thalamocortical radiations) to the cerebral cortex. The thalamus also has connections with the hippocampus, mammillary bodies, and fornix via the mammillothalamic tract.[2] The connection of limbic system structures to the anterior nuclei of the thalamus allows the thalamus to be involved in learning and episodic memory.[3] The thalamus is also involved in the regulation of sleep and wakefulness.[4]
Generally, the thalamus acts as a relay station filtering information between the brain and body. Except for olfaction, every sensory system has a thalamic nucleus that receives, processes, and sends information to an associated cortical area. The lateral geniculate nucleus of the thalamus receives visual sensory information from the retina to route to the visual cortex of the occipital lobe. The medial geniculate nucleus receives auditory sensory information from inferior colliculus and projects it to the primary auditory cortex in the temporal lobe. The ventral posterior nucleus of the thalamus is subdivided further by three. The spinothalamic tract is the sensory pathway for pain, temperature and crude touch that originates in the spinal cord and feeds into the ventral posterolateral nucleus of the thalamus for further processing, while the ventral posteromedial nucleus receives sensory information from the trigeminal nerve about the face. Lastly, the ventral intermediate nucleus has correlations with pathological tremors.[5]
The reticular nucleus is in the ventral portion of the thalamus and forms a capsule around the thalamus laterally. Interestingly, this nucleus does not project to the cerebral cortex; rather, its function is to process and modulate information it receives from other thalamic nuclei. The reticular nucleus also receives disinhibitory input from the globus pallidus allowing for the initiation of voluntary movement.
Functionally, the thalamus divides into five major functional components as[6]:
- Reticular and intralaminar nuclei dealing with arousal and pain regulation
- Sensory nuclei regulating all sensory domains except olfaction
- Effector nuclei governing motor language function
- Associative nuclei connoting cognitive functions
- Limbic nuclei encompassing mood and motivation
Embryology
During the third week of embryogenesis, the neural tube forms from the ectoderm. The neural tube forms the prosencephalon, the mesencephalon, and rhombencephalon. The prosencephalon is the most rostral of these structures and further divides into the telencephalon and diencephalon. The thalamus develops from the embryonic diencephalon.[7]
Blood Supply and Lymphatics
The basilar communicating artery, posterior cerebral artery, and posterior communicating artery are the major blood supply for the thalamus. The major vascular pedicles supplying the thalamus divide into[6][8][6]:
- Tuberothalamic artery (polar artery)
- Paramedian artery
- Thalamogeniculate artery and
- Medial and lateral posterior choroidal artery
Surgical Considerations
Due to the deep location of the thalamus, thalamic tumors have historically been challenging to manage. Recently contemporary microsurgical techniques and advances in neuroimaging have resulted in some improvement in outcomes of resections involving the thalamus.[9]
Clinical Significance
Though a central sensory relay station, thalamic lesions can paradoxically present with various non-sensory clinical patterns, thereby complicating diagnostic issues.
Thalamic aphasia can present as lexical-semantic deficits with verbal paraphasia but with intact repetition and naming.[10] Characteristically this pattern of aphasia following thalamic strokes shows speedy recovery.[11]
After a thalamic stroke, a rare condition called Dejerine-Roussy syndrome or thalamic pain syndrome may occur; this usually presents initially with the absence of sensation and tingling of the body contralateral to the affected thalamus. Months later, numbness occurs, eventually developing to severe chronic pain.[12] It is due to the involvement of the thalamogeniculate branch, thereby leading to excruciating pain owing to the absence of central cortical inhibition.[13]
The reticular thalamic nucleus, a pacemaker zone for rhythmic cortical activity, might be the ictus for generalized spike-wave, as seen in idiopathic generalized epilepsy.[14]
Patients with alcoholic Korsakoff syndrome have damage to their mamillary bodies, which can extend into the thalamus via the mammillothalamic fasciculus.[15][16]
A hereditary prion disease called fatal familial insomnia exists in which the gene PRNP located on chromosome 20 at p13 deposits in the thalamus, causing degeneration over time. Patients develop worsening insomnia that can have associated psychiatric symptoms such as panic attacks, paranoia, and phobias. They then develop hallucinations and the complete inability to sleep. Rapid weight loss follows with dementia and mutism until death occurs.[17][18]
The “pulvinar sign” is an MRI identification technique originally developed as a non-invasive method to identify patients with Creutzfeldt-Jakob disease.[19] Essentially, this technique looks for posterior thalamus changes on magnetic resonance imaging that appear as density changes in the shape of hockey sticks. Fabry disease is an X-linked lysosomal storage disease in which a deficiency of the enzyme alpha-galactosidase A causes an acclamation of globotriaosylceramide in the blood, which deposits into tissues and organs. The pulvinar sign has been found to be a highly specific sign of Fabry disease of patients with cardiac and kidney involvement.[20]
Concerning anatomical changes, the interthalamic adhesions appear enlarged in patients with Arnold-Chiari malformation type II.[21] Additionally, the ventral intermediate nucleus of the thalamus has been the target for deep brain stimulation for the treatment of medically refractory essential tremors and tremor-dominant Parkinson disease with some success.[5]
Other Issues
'Eye peering at the tip of the nose' has been taken as a consistent clinical sign in cases of thalamic hemorrhages.[22]
Media
(Click Image to Enlarge)
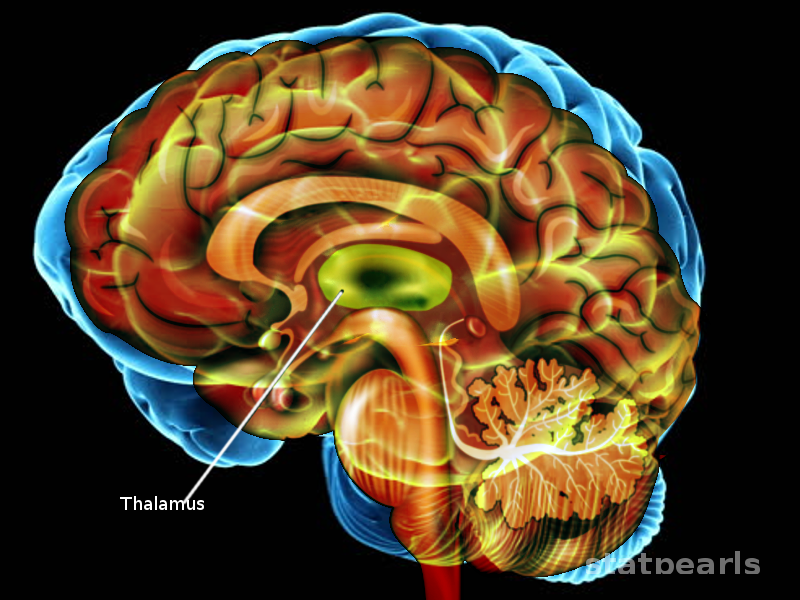
CNS Thalamus Image courtesy S Bhimji MD
(Click Image to Enlarge)
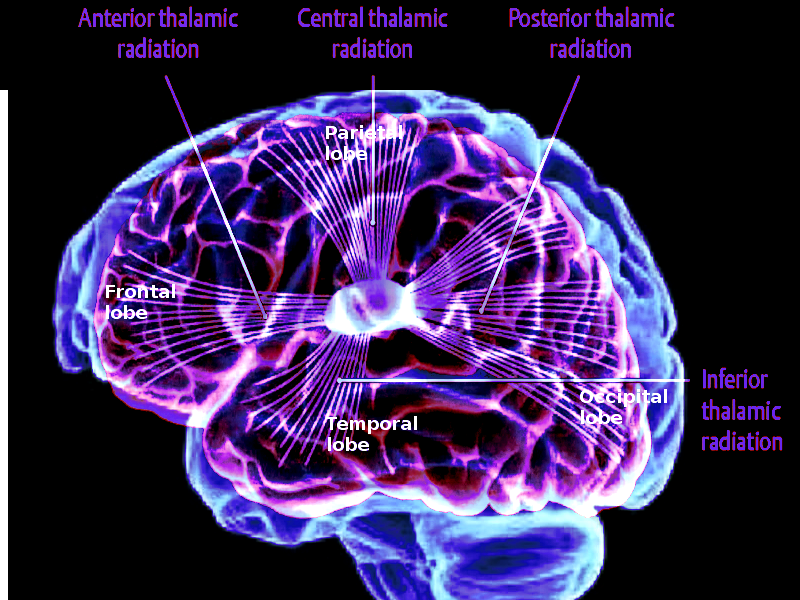
Thalamocortical projections Image courtesy O.Chaigasame
(Click Image to Enlarge)
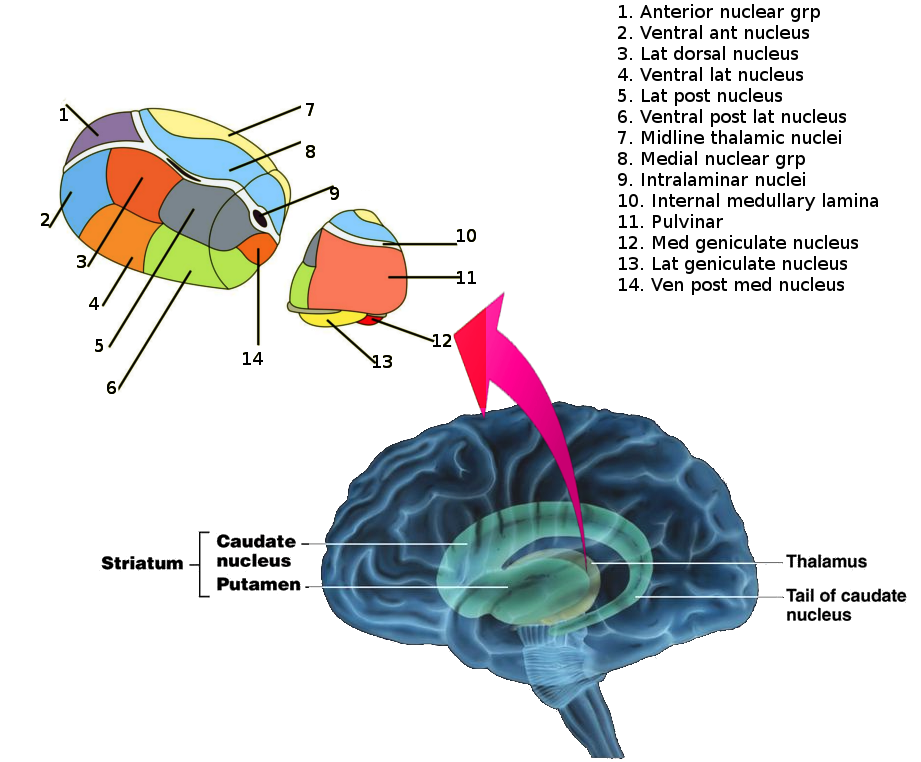
Thalamic nuclei Image courtesy S Bhimji MD
References
Savage LM, Sweet AJ, Castillo R, Langlais PJ. The effects of lesions to thalamic lateral internal medullary lamina and posterior nuclei on learning, memory and habituation in the rat. Behavioural brain research. 1997 Jan:82(2):133-47 [PubMed PMID: 9030395]
Level 3 (low-level) evidenceStein T, Moritz C, Quigley M, Cordes D, Haughton V, Meyerand E. Functional connectivity in the thalamus and hippocampus studied with functional MR imaging. AJNR. American journal of neuroradiology. 2000 Sep:21(8):1397-401 [PubMed PMID: 11003270]
Child ND, Benarroch EE. Anterior nucleus of the thalamus: functional organization and clinical implications. Neurology. 2013 Nov 19:81(21):1869-76. doi: 10.1212/01.wnl.0000436078.95856.56. Epub 2013 Oct 18 [PubMed PMID: 24142476]
Level 3 (low-level) evidenceSteriade M, Llinás RR. The functional states of the thalamus and the associated neuronal interplay. Physiological reviews. 1988 Jul:68(3):649-742 [PubMed PMID: 2839857]
Level 3 (low-level) evidenceBanerjee S, Shinde R, Sevick-Muraca EM. Probing Static Structure of Colloid-Polymer Suspensions with Multiply Scattered Light. Journal of colloid and interface science. 1999 Jan 1:209(1):142-153 [PubMed PMID: 9878147]
Schmahmann JD. Vascular syndromes of the thalamus. Stroke. 2003 Sep:34(9):2264-78 [PubMed PMID: 12933968]
Level 3 (low-level) evidenceScholpp S, Lumsden A. Building a bridal chamber: development of the thalamus. Trends in neurosciences. 2010 Aug:33(8):373-80. doi: 10.1016/j.tins.2010.05.003. Epub 2010 Jun 11 [PubMed PMID: 20541814]
Level 3 (low-level) evidenceJaved K, Reddy V, Das JM. Neuroanatomy, Posterior Cerebral Arteries. StatPearls. 2025 Jan:(): [PubMed PMID: 30860709]
Cinalli G, Aguirre DT, Mirone G, Ruggiero C, Cascone D, Quaglietta L, Aliberti F, Santi SD, Buonocore MC, Nastro A, Spennato P. Surgical treatment of thalamic tumors in children. Journal of neurosurgery. Pediatrics. 2018 Mar:21(3):247-257. doi: 10.3171/2017.7.PEDS16463. Epub 2017 Dec 22 [PubMed PMID: 29271729]
Afzal U, Farooq MU. Teaching neuroimages: thalamic aphasia syndrome. Neurology. 2013 Dec 3:81(23):e177. doi: 10.1212/01.wnl.0000436950.75473.af. Epub [PubMed PMID: 24297806]
Level 3 (low-level) evidenceOzeren A, Sarica Y, Efe R. Thalamic aphasia syndrome. Acta neurologica Belgica. 1994:94(3):205-8 [PubMed PMID: 7526590]
Ramachandran VS, McGeoch PD, Williams L. Can vestibular caloric stimulation be used to treat Dejerine-Roussy Syndrome? Medical hypotheses. 2007:69(3):486-8 [PubMed PMID: 17321064]
Wilkins RH, Brody IA. The thalamic syndrome. Archives of neurology. 1969 May:20(5):559-62 [PubMed PMID: 5767614]
Kelemen A, Barsi P, Gyorsok Z, Sarac J, Szucs A, Halász P. Thalamic lesion and epilepsy with generalized seizures, ESES and spike-wave paroxysms--report of three cases. Seizure. 2006 Sep:15(6):454-8 [PubMed PMID: 16828318]
Level 3 (low-level) evidenceKopelman MD, Thomson AD, Guerrini I, Marshall EJ. The Korsakoff syndrome: clinical aspects, psychology and treatment. Alcohol and alcoholism (Oxford, Oxfordshire). 2009 Mar-Apr:44(2):148-54. doi: 10.1093/alcalc/agn118. Epub 2009 Jan 16 [PubMed PMID: 19151162]
Level 1 (high-level) evidenceRahme R, Moussa R, Awada A, Ibrahim I, Ali Y, Maarrawi J, Rizk T, Nohra G, Okais N, Samaha E. Acute Korsakoff-like amnestic syndrome resulting from left thalamic infarction following a right hippocampal hemorrhage. AJNR. American journal of neuroradiology. 2007 Apr:28(4):759-60 [PubMed PMID: 17416834]
Level 3 (low-level) evidenceSchenkein J, Montagna P. Self-management of fatal familial insomnia. Part 2: case report. MedGenMed : Medscape general medicine. 2006 Sep 14:8(3):66 [PubMed PMID: 17406189]
Level 3 (low-level) evidenceJansen C, Parchi P, Jelles B, Gouw AA, Beunders G, van Spaendonk RM, van de Kamp JM, Lemstra AW, Capellari S, Rozemuller AJ. The first case of fatal familial insomnia (FFI) in the Netherlands: a patient from Egyptian descent with concurrent four repeat tau deposits. Neuropathology and applied neurobiology. 2011 Aug:37(5):549-53. doi: 10.1111/j.1365-2990.2010.01126.x. Epub [PubMed PMID: 20874730]
Level 3 (low-level) evidenceZeidler M, Sellar RJ, Collie DA, Knight R, Stewart G, Macleod MA, Ironside JW, Cousens S, Colchester AC, Hadley DM, Will RG. The pulvinar sign on magnetic resonance imaging in variant Creutzfeldt-Jakob disease. Lancet (London, England). 2000 Apr 22:355(9213):1412-8 [PubMed PMID: 10791525]
Level 2 (mid-level) evidenceBurlina AP, Manara R, Caillaud C, Laissy JP, Severino M, Klein I, Burlina A, Lidove O. The pulvinar sign: frequency and clinical correlations in Fabry disease. Journal of neurology. 2008 May:255(5):738-44. doi: 10.1007/s00415-008-0786-x. Epub 2008 Feb 26 [PubMed PMID: 18297328]
Level 2 (mid-level) evidenceWolpert SM, Anderson M, Scott RM, Kwan ES, Runge VM. Chiari II malformation: MR imaging evaluation. AJR. American journal of roentgenology. 1987 Nov:149(5):1033-42 [PubMed PMID: 3499774]
Choi KD, Jung DS, Kim JS. Specificity of "peering at the tip of the nose" for a diagnosis of thalamic hemorrhage. Archives of neurology. 2004 Mar:61(3):417-22 [PubMed PMID: 15023820]
Level 3 (low-level) evidence