Introduction
Total knee arthroplasty offers an alternative to individuals suffering from osteoarthritis of the knee. The improvements in surgical techniques, pain management, preoperative medical optimization, patient selection, and implant design have allowed primary total knee arthroplasty to be offered to qualifying individuals of varying ages, even to be performed as an outpatient procedure. The need for primary total knee arthroplasty is estimated to increase to nearly three and a half million procedures performed in 2030, a 673% rise compared to 2005.[1] With the advancements in the medical management and applied sciences, individuals are surpassing previously established life expectancies. The increased appeal for total knee arthroplasty has led to a concurrent increase in periprosthetic fractures.[2] Surgical fixation of periprosthetic fractures is one of the most demanding procedures an orthopedic surgeon faces. Careful preoperative preparation and referral to a well-trained surgeon are of utmost importance for a successful outcome.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Periprosthetic fractures have an increased prevalence in:
- Female sex (hormonal imbalance)
- Osteoporosis/Osteopenia
- Neuromuscular disease (Parkinson's, epilepsy, ataxia)
- Cognitive disorder (e.g. dementia)
- Medication-related (chronic steroid use)
- Inflammatory arthritides (rheumatoid arthritis, osteoarthritis, etc.)
- Infection
- Primary total knee arthroplasty (notching of the anterior femoral cortex, stress shielding)
- Implant specific (level of constraint, polyethylene wear)[3][4]
Epidemiology
The incidence of periprosthetic fractures is 300,000 per year and makes up 0.3% to 2.5% of the total fractures for the year. Revision total knee arthroplasty often requires extensive soft tissue and bony dissection and raises the incidence of periprosthetic fracture to 38%.[5] An orthopedic surgeon trained in trauma or arthroplasty is best suited to take on the complexity of these surgeries with careful dissection and an arsenal of surgical options.
Pathophysiology
Minor trauma accounts for the majority of presentations of periprosthetic fractures in the emergency department. Abu Rajab studied 40 patients, twenty cemented and twenty uncemented total knee arthroplasties, and revealed a loss of 27% loss of bone mineral density seen behind the anterior flange of the distal femur. They noted the majority of density loss occurs over the first 24 months and stabilizes after. During this period, patients were at an increased risk of traumatic events secondary to stress shielding.[6] The elastic modulus, an object's innate ability to counteract an elastic force, plays a critical role in periprosthetic distal femur fractures. Modern total knee implants are composed of mixed metals. Cuppone et al. reported that cortical bone elastic modulus to be 1/13th that of the femoral implant.[7] The difference in the elastic modulus between cortical bone and the femoral implant accounts for the potential of a stress riser.
History and Physical
The majority of patients who present with periprosthetic distal femur fractures will not recall a significant traumatic event; instead, they will claim a minor misstep or twisting injury that has led to their presentation to the hospital. Patients may reveal a recent history of fractures and falls and clue the physician into their bone health quality and quantity. Patients will complain of pain in the involved extremity and an inability to ambulate. On physical exam, patients often do not have a gross deformity of the limb but will be exquisitely tender to range of motion to the knee and palpation of the distal femur.
Evaluation
The workup of a patient with suspected periprosthetic distal femur fracture should begin with a complete x-ray evaluation of the extremity from hip to ankle. Adequate visualization of the ipsilateral hip and knee is critical for determining what implants would be available to the performing surgeon. Of utmost importance is whether the implant has subsided from its position on primary arthroplasty.[8] A retrograde intramedullary nail is a reasonable method of fixation for certain periprosthetic fractures. However, poor component positioning or non-compatible box on the femoral component can eliminate intramedullary fixation as a viable option. Also, the presence of intramedullary hardware in the involved extremity limits fixation options. Orthogonal imaging of the knee may not always provide adequate imaging for preoperative planning. If warranted, a computed tomography (CT) scan may be ordered and has the benefit of fine detail with three-dimension reconstitution possible. A periprosthetic infection has damaging effects to the surrounding bone and should always be considered if the patient presents with findings indicative of infection. Appropriate infectious workup and joint fluid analysis obtained before consideration for definitive fixation. Previous operative report or familiarity with the radiographic appearance of standard arthroplasty implants dramatically increases the ability to preoperative plan. Thompson et al. published a total knee specific implant compatibility paper of specific retrograde nail sizes and should be reviewed before surgery if this is the intended treatment modality.[8] The performing surgeon should be comfortable with a variety of surgical options ranging from in-situ fixation, distal femoral replacement, and in the worst situation, above knee amputation.
Classification systems play a significant role in orthopedics, and most fractures in the body have a classification system designed to dictate treatment. Neer developed the first classification for periprosthetic fractures in 1967. Neer classified 100 supracondylar distal femur fractures into three subtypes based on displacement and comminution.[9] Lewis and Rorabeck further classified periprosthetic distal femur fractures into three subtypes in 1997. Lewis and Rorabeck classification remains the most commonly spoken classification and separates fractures based on the displacement and stability of the component.[10] In 2006, Su developed an additional classification of supracondylar femur fractures above total knee arthroplasties. Su classifies fractures into three groups based on the location relative to the femoral component.[11]
- Neer classification of supracondylar fractures
- Type I: Nondisplaced (<5 mm or 5 degrees angulation)
- Type II: Displaced fracture > 1 cm
- IIa: Condylyes displaced medially
- IIb: Condyles displaced laterally
- Type III: Conjoined supracondylar and shaft fracture
- Su classification
- Type I: Fracture originates proximal to the femoral component
- Type II: Fracture arising at the proximal aspect of the femoral component and extends proximally
- Type III: Fracture in which any part of the fracture line can be seen distal to the upper edge of the anterior flange of the femoral component
- Lewis and Rorabeck classification of supracondylar periprosthetic distal femur fractures proximal to knee arthroplasty
- Type I: Nondisplaced; component intact
- Type II: Displaced: Component intact
- Type III: Displaced; component loose of failing
Treatment / Management
Every fracture is treated on an individual basis. Skeletal immobilization is the first priority for patients presenting with a periprosthetic distal femur fracture. Immobilization is dictated by displacement, discomfort, and body habitus. A hinged knee brace, knee immobilizer, or long leg splint should be considered for the majority of patients. Emergent provisional stabilization, with an external fixator or skeletal traction, is required in fractures with concern for soft tissue or neurovascular compromise.
Nonoperative management is rarely the recommended treatment option and is reserved for specific patient indications. Patients unfit for surgery account for the majority of periprosthetic distal femur fractures treated nonoperatively. Patients unfit for surgery are often bed-bound and require additional surveillance of their soft tissue surrounding the fracture. Frequent skin checks and extra padding of bony prominences are necessary to avoid dreaded complications. Nonoperative management options include a cast, hinged knee brace, knee immobilizer, or an external fixator. It is critical to inform the patient and the patient's family of the risk of nonunion. Culp et al. found a high nonunion rate displaced periprosthetic fractures treated non-operatively with a high conversion rate to surgery.[12]
The treatment of choice for displaced periprosthetic fractures is operative fixation. Modern technology has revolutionized the treatment options for surgical intervention with the goal of limited dissection and immediate weight-bearing.
Load sharing devices, such as conventional plates and locked plates, are reserved for Su type I-III fracture with a stable prosthesis and implants not amenable to intramedullary nail. Femoral components may not be amenable to intramedullary fixation if a stemmed prosthesis is present, has a closed box system, or implanted in an unfavorable position. Conventional plates were the first plates available for fixation. The addition of locking technology has improved fixation in the osteoporotic bone while allowing a customizable screw trajectory to avoid femoral components and has decreased the risk of nonunion.[4]
Advancements in the load sharing devices with an intramedullary nail have provided an alternative treatment modality that can be performed with less soft tissue dissection and allow for earlier weight-bearing.[13] The antegrade intramedullary nail can be considered in the absence of a stemmed femoral prosthesis. Depending on the manufacturer, the location of distal screw fixation may limit the indications for this modality. It should be reserved for fractures proximal to the anterior flange of the femoral prosthesis. The retrograde intramedullary nail is indicated for Su type I-II fractures that do not progress distally to the anterior flange, and fixation is achieved with distal interlocking screws. The success of a retrograde nail rest on the orientation and design of the femoral prosthesis. If the femoral box is placed too posterior, the passage of a nail will result in an extension deformity. Component placed into flexion or extension can lead to iatrogenic fracture or malreduction of fracture. Acquiring previous operative reports or familiarity of radiographic signs allows a surgeon to decide which implants are amenable to retrograde nail passage. Retrograde intramedullary nails have the potential to damage the polyethylene when gaining access to the distal femur and is avoided at all costs with spare polyethylene ready if needed. The presence of ipsilateral total hip arthroplasty is not a contraindication to treatment but may predispose the patient to a stress riser from the stem tip to the end of the nail. In the absence of a proximal femur prosthesis, the distal end of a retrograde intramedullary nail should end at the level of the lesser trochanter.
Revision total knee arthroplasty is indicated in Su type III or a Lewis and Rorabeck type III with sufficient bone stock. Unstable femoral components should not be stabilized with a load sharing or load-bearing device alone. Revision arthroplasty is key to a successful surgery. Revision of the femoral component with a stemmed prosthesis allows for intramedullary support and reinforced with cable fixation or plate fixation.[13]
Salvage procedures may be necessary for the worst of scenarios. A distal femoral replacement is indicated in those with a Su type III or a Lewis and Rorabeck type III fracture with inadequate bone stock and an unstable prosthesis.[4] Distal femur replacements are a complicated and expensive procedure. However, it is a salvage procedure that has a decreased operative time compared to conventional plating, allows immediate weight-bearing, and reduces the risk of immobilization. An infected Su type III or a Lewis and Rorabeck type III fracture with an unstable prosthesis in a critically ill patient may require urgent or emergent above-knee amputation.
Differential Diagnosis
Before radiographic evaluation, the differential diagnosis should include:
- Periprosthetic fracture
- Aseptic loosening
- Prosthetic joint infection
- Ligamentous injury
- Fracture of the metal or polyethylene implant
- Contusion
- Knee dislocation
- Venous thromboembolism
- Occult fracture
Prognosis
Distal femur fractures and hip fractures have a well-established mortality rate of 30%. Streubel et al. analyzed 92 patients from 1992 to 2009, with an average age of 77.9 years. 78% of the patients were female. The majority of fractures were closed (95%) and extraarticular (76%). 52% of fractures occurred around a total knee arthroplasty. The overall mortality rate was 38% with a ten year follow up. Mortality rate increased over their time frames of 30 days, six months, and one year. Their rates were 6%, 18%, and 25%, respectively. Streubel et al. outlined several factors that correlate with successful patient outcomes. Patients with poor preoperative medical status, advanced age, and restricted ambulatory status tend to have a complicated postoperative course plagued with numerous medical complications. Complex fracture morphology and fractures with significant bone loss are best suited for surgeons with considerable experience in overcoming these obstacles.[14]
Complications
Common complications associated with surgical fixation include delayed union, nonunion, failure of hardware, and infection. Nonunion is a complication of operative and nonoperative management. Culp et al. advised against the use of closed treatment for periprosthetic distal femur fractures. Twenty (20%) of patients were found to have a nonunion, and twenty-three percent (23%) presented with symptomatic malunion. Merkell's study found that thirty-five (35%) of patients that elected nonoperative management required revision arthroplasty because of nonunion.[15] The addition of locking technology to plates technology provides an extramedullary option in osteoporotic bone. Lower rates of malunion (20%) and similar rates of nonunion (4.2%) have been reported when compared with intramedullary fixation.[12][16]The intramedullary nail group had a lower rate of nonunion than the locked plate group at 5.1% and 11.3%, respectively. Henderson et al. quoted the rate of infection for in-situ fixation with plating up to 9%. Compared to retrograde intramedullary fixation, in-situ plate fixation involved a more substantial operative dissection and trauma to the bone and soft tissue. Plate fixation of periprosthetic femur fractures has a risk of screw pullout with resultant malalignment.[17] Arthrofibrosis of the knee, neurovascular injury, and wound complications also complicate surgery in some patients.
Postoperative and Rehabilitation Care
The ability to immediately weight-bear is the ideal situation. With the advent of load sharing devices, such as an intramedullary nail, an overall decrease in patients requiring weight-bearing restrictions, is achievable. Improved technology of intramedullary implants is expanding the indications for distal fractures. Intramedullary nail fixation is a load sharing device and allows for immediate weight-bearing. Early ambulation and focused physical therapy limit the complications associated with immobilization and restricted weight-bearing. Periprosthetic distal femur fractures exclusively treated with plate fixation require weight-bearing restrictions for weeks to months. Postoperative patient immobilization drastically increases the complication risk associated with surgery, and avoidance of this limitation is one of the main indications for surgery.
Deterrence and Patient Education
Fall prevention is crucial to avoiding fractures in general. The combined efforts of a primary care physician and a surgeon should aim to optimize bone health and limit factors that contribute to falls. Keeping up with the U.S. Preventive Services Task Force (USPSTF) recommendations regarding Dual-energy x-ray absorptiometry (DEXA) scanning should be followed. The addition of supplements and/or prescription medication should be implemented as seen fit by the treatment team. Assistive devices should be used by individuals who do not feel stable ambulating alone.
Enhancing Healthcare Team Outcomes
The increasing demand for total knee arthroplasty and subsequent increased incidence of periprosthetic femur fractures requires effective communication among multiple departments. The aging patient who suffers a periprosthetic femur fracture often requires a primary medical service, pharmacist, therapist, and surgeon. The goal of care includes preoperative medical optimization, effective fracture management, and focused therapy to decrease hospital length of stay and facilitate early weight-bearing. Nurses, case managers, and pharmacists familiar with orthopedic preoperative and postoperative management play a crucial role in the overall success of treatment. [Level 5]
Media
(Click Image to Enlarge)

Anteroposterior View of a Periprosthetic Distal Femur Fracture. This anteroposterior view image illustrates a periprosthetic distal femur fracture observed in the context of a cemented cruciate-retaining total knee arthroplasty.
Contributed by D Mesko, DO
(Click Image to Enlarge)

Lateral View of a Periprosthetic Distal Femur Fracture. This lateral view image depicts a periprosthetic distal femur fracture around a cemented cruciate-retaining total knee arthroplasty.
Contributed by D Mesko, DO
(Click Image to Enlarge)
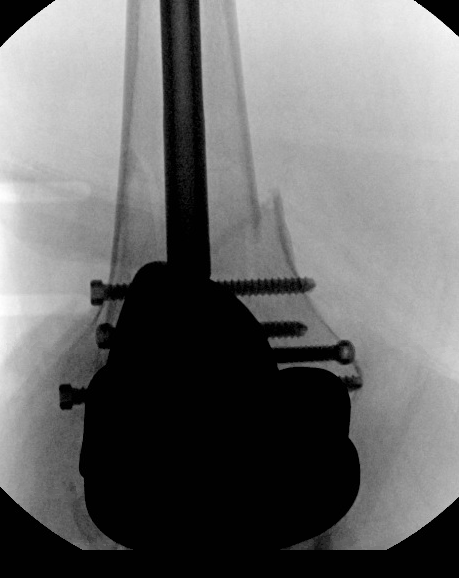
Anteroposterior view of a retrograde intramedullary nail for a periprosthetic distal femure fracture Contributed by Daniel Mesko, DO
(Click Image to Enlarge)

Lateral view of a retrograde intramedullary nail for a periprosthetic distal femure fracture Contributed by Daniel Mesko, DO
(Click Image to Enlarge)

Retrograde femoral nail of periprosthetic distal femur fracture Contributed by Daniel R Mesko DO
References
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. The Journal of bone and joint surgery. American volume. 2007 Apr:89(4):780-5 [PubMed PMID: 17403800]
Lunenfeld B, Stratton P. The clinical consequences of an ageing world and preventive strategies. Best practice & research. Clinical obstetrics & gynaecology. 2013 Oct:27(5):643-59. doi: 10.1016/j.bpobgyn.2013.02.005. Epub 2013 Mar 28 [PubMed PMID: 23541823]
Nauth A, Ristevski B, Bégué T, Schemitsch EH. Periprosthetic distal femur fractures: current concepts. Journal of orthopaedic trauma. 2011 Jun:25 Suppl 2():S82-5. doi: 10.1097/BOT.0b013e31821b8a09. Epub [PubMed PMID: 21566481]
Lombardo DJ, Siljander MP, Sobh A, Moore DD, Karadsheh MS. Periprosthetic fractures about total knee arthroplasty. Musculoskeletal surgery. 2020 Aug:104(2):135-143. doi: 10.1007/s12306-019-00628-9. Epub 2019 Oct 23 [PubMed PMID: 31643045]
Canton G, Ratti C, Fattori R, Hoxhaj B, Murena L. Periprosthetic knee fractures. A review of epidemiology, risk factors, diagnosis, management and outcome. Acta bio-medica : Atenei Parmensis. 2017 Jun 7:88(2S):118-128 [PubMed PMID: 28657573]
Abu-Rajab RB, Watson WS, Walker B, Roberts J, Gallacher SJ, Meek RM. Peri-prosthetic bone mineral density after total knee arthroplasty. Cemented versus cementless fixation. The Journal of bone and joint surgery. British volume. 2006 May:88(5):606-13 [PubMed PMID: 16645105]
Cuppone M, Seedhom BB, Berry E, Ostell AE. The longitudinal Young's modulus of cortical bone in the midshaft of human femur and its correlation with CT scanning data. Calcified tissue international. 2004 Mar:74(3):302-9 [PubMed PMID: 14517712]
Thompson SM, Lindisfarne EA, Bradley N, Solan M. Periprosthetic supracondylar femoral fractures above a total knee replacement: compatibility guide for fixation with a retrograde intramedullary nail. The Journal of arthroplasty. 2014 Aug:29(8):1639-41. doi: 10.1016/j.arth.2013.07.027. Epub 2014 Jun 11 [PubMed PMID: 24929282]
Neer CS 2nd, Grantham SA, Shelton ML. Supracondylar fracture of the adult femur. A study of one hundred and ten cases. The Journal of bone and joint surgery. American volume. 1967 Jun:49(4):591-613 [PubMed PMID: 6025996]
Level 3 (low-level) evidenceRorabeck CH, Taylor JW. Classification of periprosthetic fractures complicating total knee arthroplasty. The Orthopedic clinics of North America. 1999 Apr:30(2):209-14 [PubMed PMID: 10196422]
Su ET, Kubiak EN, Dewal H, Hiebert R, Di Cesare PE. A proposed classification of supracondylar femur fractures above total knee arthroplasties. The Journal of arthroplasty. 2006 Apr:21(3):405-8 [PubMed PMID: 16627150]
Sarmah SS, Patel S, Reading G, El-Husseiny M, Douglas S, Haddad FS. Periprosthetic fractures around total knee arthroplasty. Annals of the Royal College of Surgeons of England. 2012 Jul:94(5):302-7. doi: 10.1308/003588412X13171221592537. Epub [PubMed PMID: 22943223]
McGraw P, Kumar A. Periprosthetic fractures of the femur after total knee arthroplasty. Journal of orthopaedics and traumatology : official journal of the Italian Society of Orthopaedics and Traumatology. 2010 Sep:11(3):135-41. doi: 10.1007/s10195-010-0099-6. Epub 2010 Jul 27 [PubMed PMID: 20661762]
Streubel PN, Ricci WM, Wong A, Gardner MJ. Mortality after distal femur fractures in elderly patients. Clinical orthopaedics and related research. 2011 Apr:469(4):1188-96. doi: 10.1007/s11999-010-1530-2. Epub 2010 Sep 10 [PubMed PMID: 20830542]
Merkel KD, Johnson EW Jr. Supracondylar fracture of the femur after total knee arthroplasty. The Journal of bone and joint surgery. American volume. 1986 Jan:68(1):29-43 [PubMed PMID: 3941120]
Henderson CE, Kuhl LL, Fitzpatrick DC, Marsh JL. Locking plates for distal femur fractures: is there a problem with fracture healing? Journal of orthopaedic trauma. 2011 Feb:25 Suppl 1():S8-14. doi: 10.1097/BOT.0b013e3182070127. Epub [PubMed PMID: 21248560]
Wallace SS, Bechtold D, Sassoon A. Periprosthetic fractures of the distal femur after total knee arthroplasty : Plate versus nail fixation. Orthopaedics & traumatology, surgery & research : OTSR. 2017 Apr:103(2):257-262. doi: 10.1016/j.otsr.2016.11.018. Epub 2017 Jan 13 [PubMed PMID: 28089667]