Introduction
Over the last decade, endoscopic vein harvesting (EVH) has been the method of choice to harvest the greater saphenous vein (GSV), which is the most widely used conduit in coronary artery bypass graft (CABG) surgery. The saphenous veins are often used for their ease of harvesting and length. The global demand for CABG surgery and the increasing need for patients to require multiple coronary artery bypasses in the same procedure have increased the demand for more and better conduits.[1]
In the past, the conventional open technique of GSV harvesting involved a long skin incision, which often carries a higher incidence of wound complications and pain. This is often coupled with increased length of hospital stay and decreased patient satisfaction. The EVH technique has evolved and developed to improve the above-mentioned drawbacks of the open procedure.[2]
Results from a recent review of approximately 28,000 patients from 22 studies found that the mid- and long-term patency of vein conduits harvested using the endoscopic technique was lower than that of the open technique. However, this study was limited to 1 year. The researchers concluded that growing surgical experience in the EVH might be associated with better outcomes.[3] Although the long-term patency of harvested conduits by EVH has been questioned, many studies show that the patency of vein grafts harvested by the EVH technique is similar to that reported using the conventional method.[4]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The GSV is the longest vein in the human body, originating from the medial marginal vein of the foot and terminating at the femoral vein via the saphenous opening, just below the inguinal ligament. The GSV follows a distinct course: ascending anterior to the medial malleolus, traversing the distal third of the medial tibial surface, crossing it obliquely, and continuing posteriorly along the medial knee border. From there, it ascends along the medial aspect of the thigh, ultimately draining into the femoral vein (see Image. Saphenous Neurovasculature). Along its course, it receives tributaries such as the anterior and posterior accessory saphenous veins and communicates with the small saphenous vein via the Giacomini vein. The GSV connects with the deep venous system through perforator veins, including Crockett (lower leg), Boyd (below the knee), and Dodd (above the knee) perforators.
Physiologically, the GSV plays a crucial role in venous return, directing blood from the superficial to the deep venous system, aided by 1-way valves that prevent retrograde flow. Valve dysfunction can lead to chronic venous insufficiency, varicose veins, venous stasis ulcers, and edema. Due to its length, diameter, and adaptability to arterial circulation, the GSV is frequently used as a conduit in CABG and peripheral vascular procedures. Anatomical variations, including duplication of the GSV below the knee, are common, making it susceptible to postoperative pain and paresthesias following surgical interventions.[5]
Indications
The main indication for EVH is CABG, where the GSV serves as a conduit for revascularization. Other potential bypass conduits include the internal mammary artery and radial artery, but the saphenous vein remains a primary choice due to its availability, length, and adaptability. Beyond CABG, the GSV is also utilized in various other vascular procedures, including dialysis fistulas, peripheral vascular bypass interventions, and cerebral bypass surgeries.[6]
Contraindications
From a technical point of view, there are no absolute contraindications for EVH. However, there are some reservations about harvesting the saphenous vein in general, especially in patients with extensive varicosities, deep venous thrombosis, and those where the vessel is of poor quality and would not function as an adequate conduit.[7]
Equipment
Successful EVH requires specialized equipment that ensures adequate visualization, illumination, and safe dissection of the GSV while minimizing trauma. The essential components include:
- Endoscopic visualization system
- A 0° endoscopic lens connected through a cable to a high-definition monitor video display provides real-time visualization of the surgical field.
- A light source unit is wired to the lens to ensure proper illumination within the tunnel for vein harvesting.
- Insufflation system
- A carbon dioxide insufflation system is necessary to inflate and maintain the tunnel around the saphenous vein, improving visibility and space for maneuvering.
- Vein harvesting kit
- A single-use, prepackaged EVH kit is commonly used, which includes:
- A tissue retractor/cannula that serves as the housing for the endoscope.
- An electrocautery probe for precise dissection and hemostasis.
- Blunt dissector tools to separate the vein from surrounding tissues safely.
- A single-use, prepackaged EVH kit is commonly used, which includes:
- Suction and irrigation system
- Suction devices help remove blood, fluids, or smoke generated from cautery use.
- Irrigation may be used to flush the surgical field to maintain clarity.
Different manufacturers produce EVH systems with similar core mechanisms, but minor design variations exist across brands.[8] These variations may include differences in handle ergonomics, cannula shape, or electrocautery settings, which require proper training and familiarity before use. Ensuring that all EVH equipment is functional, properly calibrated, and ready for use before the procedure is essential to optimize efficiency, patient safety, and surgical outcomes.
Personnel
The personnel required for EVH include:
- Surgeon
- Surgical assistant
- Anesthesiologist or nurse anesthetist
- Surgical nurse
- Scrub tech
Preparation
While no specific patient preparation is required for EVH, preoperative bedside venous Doppler mapping is highly recommended and, in many centers, considered mandatory before harvesting. This noninvasive test provides critical information about the GSV's location, size, and quality, ensuring its suitability as a conduit. Doppler ultrasound offers high-accuracy measurements, typically within a 95% confidence margin of the predicted conduit diameter.[9] This test helps determine the optimal harvest site or whether to abandon the procedure altogether in cases of small-caliber veins (diameter <1.5–2 mm), severe dilation, or extensive varicosities. The quick test takes less than 10 minutes and is vital in optimizing surgical outcomes.
Technique or Treatment
Under general anesthesia, with the patient in a supine position, the surgical team determines the laterality and harvest site, referencing preoperative venous Doppler mapping for guidance. The knee is flexed to 90 to 120 degrees for optimal access with mild external hip rotation on the ipsilateral side. Towels support the leg posteriorly at the popliteal region to maintain stability.[10]
Based on surgeon preference and vein mapping results, a 2 cm skin incision is made on the medial aspect of the lower limb, either above or below the medial tibial tuberosity. After identifying the GSV, standard surgical dissection frees the proximal vein, confirming its suitability as a conduit before proceeding. A balloon port is then advanced through the incision to seal the tunnel and prevent carbon dioxide escape. The endoscope is introduced into the subcutaneous tissue tunnel under direct vision to minimize trauma. Some centers administer low-dose heparin at this stage to prevent thrombus formation inside the conduit.[11]
Carbon dioxide insufflation (10–13 mm Hg) maintains tunnel patency and facilitates gentle dissection, minimizing the risk of venous wall injury or branch avulsion. Once dissection is completed, endoscopic electrocautery is used to cut and cauterize tributary branches while freeing the vein from its surrounding adventitia. Small incisions at the groin and medial malleolus allow for the division and extraction of the conduit at the original incision site. The proximal and distal vein ends are transfixed with 3-0 silk sutures and secured with medium titanium clips.[1]
The tunnel is carefully inspected for hemostasis and then packed with an antibiotic-soaked swab for 5 minutes before closure. Some institutions routinely place a surgical drain, while others use it selectively in patients at higher risk of postoperative bleeding. All wounds are sutured appropriately using absorbable sutures and staples, and the limb is tightly bandaged to ensure hemostasis. Once extracted, the vein is cannulated and meticulously inspected for tears, thrombus, or avulsed branches. All branches are clipped with small clips, while tears are repaired using 7-0 nonabsorbable sutures. The conduit is stored in heparinized saline until ready for anastomosis.[12]
Complications
EVH is a minimally invasive technique that significantly reduces complications compared to traditional open harvesting methods. EVH is associated with a markedly lower incidence of leg wound infections, hematomas, seromas, and wound dehiscence, leading to faster recovery and improved patient outcomes. Wound infection remains the most common complication, although its occurrence is significantly lower than in conventional open techniques.[13] Most cases of hematoma, dehiscence, and infection can be managed conservatively, though surgical intervention may be required in severe cases.[14][15]
Saphenous nerve injury is another important consideration in EVH. This can result in postoperative pain, paresthesias, or hyperalgesia along the medial aspect of the lower limb, particularly above the harvest site. While these symptoms are often temporary, they can lead to more postoperative leg pain than sternal discomfort in some patients. Careful surgical technique is necessary to avoid mechanical trauma or heat-related nerve damage, especially in the lower leg, where the saphenous nerve is near the GSV.[16]
Another potential complication arises from using carbon dioxide insufflation to maintain tunnel patency. This technique can lead to pneumoperitoneum, subcutaneous extravasation, or air embolism. In such cases, the primary treatment involves halting insufflation and providing hemodynamic support until the carbon dioxide is absorbed.[17]
While EVH has largely addressed many complications of open vein harvesting, initial concerns about its impact on vein graft integrity and long-term patency were raised. Early observational studies, including a posthoc analysis of the Project of Ex-vivo Vein Graft Engineering via Transfection IV (PREVENT IV) trial, provided results suggesting higher rates of midterm graft failure, myocardial infarction, repeat revascularization, and mortality with EVH.[18] Similarly, results from a meta-analysis of 22 observational and randomized studies indicated that EVH may have lower midterm and long-term graft patency than open harvesting.[19]
However, more recent randomized controlled trials have shown no significant differences in long-term clinical outcomes between EVH and traditional techniques, aside from the clear benefits of reduced leg wound complications and postoperative pain. With a 4.7-year follow-up, the REGROUP trial confirmed that EVH provides comparable long-term clinical outcomes to the open approach.[20][21] Additionally, results from a retrospective analysis of the REGROUP trial found no significant difference in the overall costs of CABG surgeries and follow-up care between EVH and open vein harvesting.[22][23] Consequently, EVH has become the standard approach for saphenous vein harvesting in the United States.[2]
Clinical Significance
EVH has become the preferred technique for harvesting the GSV for various surgical procedures, particularly CABG surgery. Results from a recent meta-analysis of 43 randomized controlled trials and observational studies involving 27,789 patients compared the 2 techniques. Of these, 46% underwent EVH, while 56% received the conventional open procedure. The results confirmed the superiority of the EVH technique for multiple endpoints, including conduit failure, myocardial infarction, mortality, and wound infection.
Harvesting the GSV is a critical step in various vascular and cardiac procedures. EVH techniques offer comparable technical outcomes to traditional methods while reducing morbidity, wound infections, and hospital stays and improving patient satisfaction. The success of EVH depends on seamless coordination between the surgeon, nursing staff, and radiologist, ensuring optimal patient care and improved overall prognosis.
Despite the widespread adoption of EVH, a significant gap exists in the literature regarding structured training programs for surgical teams. Proper harvesting technique is essential, as vein damage—including torn branches, adventitial disruption, and thermal injury—has been associated with lower graft patency and early failure. Study results have shown that clinicians with less experience in EVH are more likely to cause vascular injury, underscoring the need for comprehensive training.[24]
Vendor-led training programs should incorporate didactic sessions focused on equipment functionality and procedural techniques to bridge this gap. These should be reinforced with hands-on training using simulation models, cadaveric specimens, and real-time case observation. Additionally, operating room personnel should receive targeted instruction to ensure proficiency with EVH equipment and workflow coordination.
Beyond vendor-led programs, structured internal training is crucial for sustained skill development. Ideally, mentorship from experienced harvesters should be available during the initial learning phase, though this may not always be feasible. Clinicians new to saphenous vein harvesting should undergo detailed anatomical reviews and learn strategies for managing technical challenges, such as dual venous systems, large branches, and intraoperative bleeding.[25] Standardized training protocols will enhance technical proficiency, improve patient outcomes, and ensure long-term graft success.
Enhancing Healthcare Team Outcomes
Successful endoscopic vein harvesting (EVH) requires a multidisciplinary approach, where advanced clinicians, nurses, pharmacists, and other healthcare professionals work together to optimize patient outcomes and safety. Surgeons and advanced clinicians must have technical proficiency in EVH, ensuring precise dissection, minimal trauma, and preservation of vein integrity to maximize graft patency. Anesthesia teams are critical in maintaining hemodynamic stability, managing patient positioning, and minimizing complications such as carbon dioxide embolism. Nurses and surgical technologists are essential in preparing equipment, assisting intraoperatively, and monitoring patients postoperatively for wound complications, hematomas, or neuropathic pain.
Effective interprofessional communication and care coordination are vital to reducing errors and improving outcomes. Preoperative collaboration with radiologists ensures accurate venous mapping, identifying the best conduit for harvest and avoiding unnecessary complications. Pharmacists contribute by ensuring appropriate anticoagulation protocols and managing postoperative pain and infection prophylaxis. Postoperatively, coordinated follow-up with vascular teams, physical therapists, and wound care specialists enhances patient recovery, mobility, and long-term graft viability. Regular team briefings, structured training, and standardized protocols help improve efficiency, patient safety, and overall team performance, leading to better surgical outcomes and patient satisfaction in EVH.
Media
(Click Image to Enlarge)
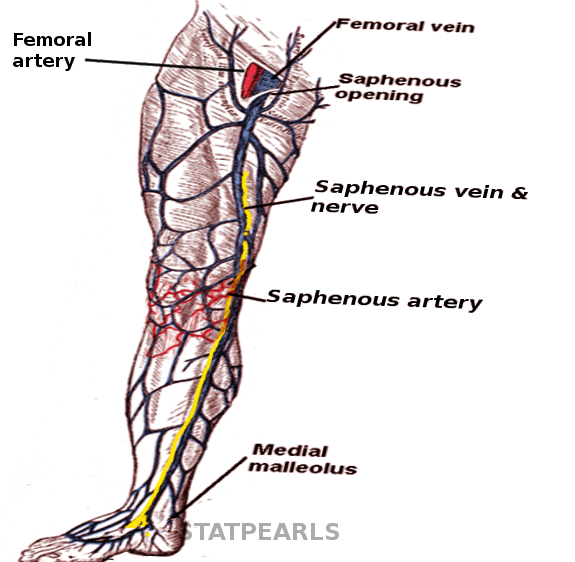
Saphenous Neurovasculature. The greater saphenous vein follows a distinct course: ascending anterior to the medial malleolus, traversing the distal third of the medial tibial surface, crossing it obliquely, and continuing posteriorly along the medial knee border. From there, it ascends along the medial aspect of the thigh, ultimately draining into the femoral vein.
Contributed by S Bhimji, MD
References
Zingaro C, Cefarelli M, Berretta P, Matteucci S, Pierri M, Di Eusanio M. Endoscopic vein-graft harvesting in coronary artery bypass surgery: Tips and tricks. Multimedia manual of cardiothoracic surgery : MMCTS. 2019 Jul 9:2019():. doi: 10.1510/mmcts.2019.019. Epub 2019 Jul 9 [PubMed PMID: 31290620]
Allen K, Cheng D, Cohn W, Connolly M, Edgerton J, Falk V, Martin J, Ohtsuka T, Vitali R. Endoscopic Vascular Harvest in Coronary Artery Bypass Grafting Surgery: A Consensus Statement of the International Society of Minimally Invasive Cardiothoracic Surgery (ISMICS) 2005. Innovations (Philadelphia, Pa.). 2005 Winter:1(2):51-60 [PubMed PMID: 22436545]
Level 3 (low-level) evidenceLi G, Zhang Y, Wu Z, Liu Z, Zheng J. Mid-term and long-term outcomes of endoscopic versus open vein harvesting for coronary artery bypass: A systematic review and meta-analysis. International journal of surgery (London, England). 2019 Dec:72():167-173. doi: 10.1016/j.ijsu.2019.11.003. Epub 2019 Nov 9 [PubMed PMID: 31707009]
Level 1 (high-level) evidenceKim DY, Song H, Kim HW, Jo GH, Kang J. Early Outcomes of Endoscopic Vein Harvesting during the Initial Learning Period. The Korean journal of thoracic and cardiovascular surgery. 2015 Jun:48(3):174-9. doi: 10.5090/kjtcs.2015.48.3.174. Epub 2015 Jun 5 [PubMed PMID: 26078923]
Portugal IB, Ribeiro Ide L, Sousa-Rodrigues CF, Monte-Bispo RF, Rocha AC. Distribution of saphenous vein valves and its practical importance. Revista brasileira de cirurgia cardiovascular : orgao oficial da Sociedade Brasileira de Cirurgia Cardiovascular. 2014 Oct-Dec:29(4):564-8. doi: 10.5935/1678-9741.20140038. Epub [PubMed PMID: 25714210]
Level 2 (mid-level) evidenceCheatle T. The long saphenous vein: to strip or not to strip? Seminars in vascular surgery. 2005 Mar:18(1):10-4 [PubMed PMID: 15791547]
Bonde P, Graham AN, MacGowan SW. Endoscopic vein harvest: advantages and limitations. The Annals of thoracic surgery. 2004 Jun:77(6):2076-82 [PubMed PMID: 15172271]
Level 1 (high-level) evidencevan Diepen S, Brennan JM, Hafley GE, Reyes EM, Allen KB, Ferguson TB, Peterson ED, Williams JB, Gibson CM, Mack MJ, Kouchoukos NT, Alexander JH, Lopes RD. Endoscopic harvesting device type and outcomes in patients undergoing coronary artery bypass surgery. Annals of surgery. 2014 Aug:260(2):402-8. doi: 10.1097/SLA.0000000000000377. Epub [PubMed PMID: 24368640]
Level 1 (high-level) evidenceManetta F, Yu PJ, Mattia A, Karaptis JC, Hartman AR. Bedside Vein Mapping for Conduit Size in Coronary Artery Bypass Surgery. JSLS : Journal of the Society of Laparoendoscopic Surgeons. 2017 Apr-Jun:21(2):. doi: 10.4293/JSLS.2016.00083. Epub [PubMed PMID: 28439192]
Mahmood D, Rosati F, Petsikas D, Payne D, Torkan L, Bisleri G. Endoscopic saphenous vein harvesting with a non-sealed approach. Multimedia manual of cardiothoracic surgery : MMCTS. 2019 Apr 9:2019():. doi: 10.1510/mmcts.2019.009. Epub 2019 Apr 9 [PubMed PMID: 30990577]
Brown EN, Kon ZN, Tran R, Burris NS, Gu J, Laird P, Brazio PS, Kallam S, Schwartz K, Bechtel L, Joshi A, Zhang S, Poston RS. Strategies to reduce intraluminal clot formation in endoscopically harvested saphenous veins. The Journal of thoracic and cardiovascular surgery. 2007 Nov:134(5):1259-65 [PubMed PMID: 17976458]
Chernyavskiy A, Volkov A, Lavrenyuk O, Terekhov I, Kareva Y. Comparative results of endoscopic and open methods of vein harvesting for coronary artery bypass grafting: a prospective randomized parallel-group trial. Journal of cardiothoracic surgery. 2015 Nov 12:10():163. doi: 10.1186/s13019-015-0353-3. Epub 2015 Nov 12 [PubMed PMID: 26563714]
Level 2 (mid-level) evidenceSampath HK, Lee TJH, Cher CE, Liang S, Cheong OO, Kofidis T, Vitaly S, Sazzad F. A Comprehensive Clinical Outcome Analysis of Endoscopic Vessel Harvesting for Coronary Artery Bypass Surgery. Journal of clinical medicine. 2024 Jun 11:13(12):. doi: 10.3390/jcm13123405. Epub 2024 Jun 11 [PubMed PMID: 38929933]
Level 2 (mid-level) evidenceMa GT, Liu XR, Zhang CJ, Liu JZ, Miao Q, Jiang C, Mao R. [Endoscopic Saphenous Vein Harvesting versus Open Vein Harvesting Techniques]. Zhongguo yi xue ke xue yuan xue bao. Acta Academiae Medicinae Sinicae. 2015 Aug:37(4):420-3. doi: 10.3881/j.issn.1000-503X.2015.04.009. Epub [PubMed PMID: 26564458]
Siddiqui S, Whooley J, Miceli A, Bartolozzi F, Soo A. Endoscopic vein harvesting: a guide for approaching difficult cases and assessing patients preoperatively. Interactive cardiovascular and thoracic surgery. 2022 Aug 3:35(3):. doi: 10.1093/icvts/ivac142. Epub [PubMed PMID: 35640590]
Level 3 (low-level) evidenceRaja SG, Sarang Z. Endoscopic vein harvesting: technique, outcomes, concerns & controversies. Journal of thoracic disease. 2013 Nov:5 Suppl 6(Suppl 6):S630-7. doi: 10.3978/j.issn.2072-1439.2013.10.01. Epub [PubMed PMID: 24251019]
Suarez-Pierre A, Terasaki Y, Magruder JT, Kapoor A, Grant MC, Lawton JS. Complications of CO(2) insufflation during endoscopic vein harvesting. Journal of cardiac surgery. 2017 Dec:32(12):783-789. doi: 10.1111/jocs.13249. Epub 2017 Nov 23 [PubMed PMID: 29169212]
Lopes RD, Hafley GE, Allen KB, Ferguson TB, Peterson ED, Harrington RA, Mehta RH, Gibson CM, Mack MJ, Kouchoukos NT, Califf RM, Alexander JH. Endoscopic versus open vein-graft harvesting in coronary-artery bypass surgery. The New England journal of medicine. 2009 Jul 16:361(3):235-44. doi: 10.1056/NEJMoa0900708. Epub [PubMed PMID: 19605828]
Level 1 (high-level) evidenceMarkar SR, Kutty R, Edmonds L, Sadat U, Nair S. A meta-analysis of minimally invasive versus traditional open vein harvest technique for coronary artery bypass graft surgery. Interactive cardiovascular and thoracic surgery. 2010 Feb:10(2):266-70. doi: 10.1510/icvts.2009.222430. Epub 2009 Nov 26 [PubMed PMID: 19942633]
Level 1 (high-level) evidenceZenati MA, Gaziano JM, Collins JF, Biswas K, Gabany JM, Quin JA, Bitondo JM, Bakaeen FG, Kelly RF, Shroyer AL, Bhatt DL. Choice of vein-harvest technique for coronary artery bypass grafting: rationale and design of the REGROUP trial. Clinical cardiology. 2014 Jun:37(6):325-30. doi: 10.1002/clc.22267. Epub 2014 Mar 14 [PubMed PMID: 24633760]
Belyayev L, Stock EM, Hattler B, Bakaeen FG, Kinlay S, Quin JA, Haime M, Biswas K, Zenati MA. Complete Coronary Revascularization and Outcomes in Patients Who Underwent Coronary Artery Bypass Grafting: Insights from The REGROUP Trial. The American journal of cardiology. 2024 Apr 15:217():127-135. doi: 10.1016/j.amjcard.2024.01.015. Epub 2024 Jan 23 [PubMed PMID: 38266796]
Wagner TH, Hattler B, Stock EM, Biswas K, Bhatt DL, Bakaeen FG, Gujral K, Zenati MA. Costs of Endoscopic vs Open Vein Harvesting for Coronary Artery Bypass Grafting: A Secondary Analysis of the REGROUP Trial. JAMA network open. 2022 Jun 1:5(6):e2217686. doi: 10.1001/jamanetworkopen.2022.17686. Epub 2022 Jun 1 [PubMed PMID: 35727582]
Eckey H, Heseler S, Hiligsmann M. Economic Evaluation of Endoscopic vs Open Vein Harvesting. The Annals of thoracic surgery. 2023 May:115(5):1144-1150. doi: 10.1016/j.athoracsur.2022.09.017. Epub 2022 Sep 20 [PubMed PMID: 37096651]
Krishnamoorthy B, Critchley WR, Venkateswaran RV, Barnard J, Caress A, Fildes JE, Yonan N. A comprehensive review on learning curve associated problems in endoscopic vein harvesting and the requirement for a standardised training programme. Journal of cardiothoracic surgery. 2016 Apr 8:11():45. doi: 10.1186/s13019-016-0442-y. Epub 2016 Apr 8 [PubMed PMID: 27059309]
Kiani S, Desai PH, Thirumvalavan N, Kurian DJ, Flynn MM, Zhao X, Poston RS. Endoscopic venous harvesting by inexperienced operators compromises venous graft remodeling. The Annals of thoracic surgery. 2012 Jan:93(1):11-7; discussion 17-8. doi: 10.1016/j.athoracsur.2011.06.026. Epub 2011 Oct 13 [PubMed PMID: 21996436]