Introduction
Peripheral vascular disease (PVD) includes peripheral arterial disease (PAD) and venous disease. PAD is a chronic progressive atherosclerotic disease leading to partial or total peripheral vascular occlusion. PAD typically affects the abdominal aorta, iliac arteries, lower limbs, and occasionally the upper extremities.[1] PAD affects nearly 200 million people worldwide with increasing global importance due to longer life expectancy and prolonged risk factor exposure.[2][3] Patients with PAD have a variable disease presentation and course with some patients remaining asymptomatic and with others progressing to arterial ulceration, claudication, resting limb ischemia, and limb loss.[4] PAD is a cardiovascular disease equivalent, with associated high risk fatal and non-fatal cardiovascular events frequently occurring, such as myocardial infarction and stroke.[5] PAD is a progressive, debilitating systemic disease that requires interprofessional involvement for improved patient outcomes.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Peripheral vascular disease is primarily driven by progressive atherosclerotic disease resulting in the reduction of major organ blood flow and end-organ ischemia. The process of atherosclerosis is complex, with the involvement of numerous cells, proteins, and pathways. Important non-modifiable and modifiable risk factors have been identified in the advancement of atherosclerosis.
Risk factors include:[4][6][7][8]
- Tobacco use
- Diabetes mellitus
- Hypertension
- HIV
- High cholesterol
- Age more than 50 years
- Elevated homocysteine levels
- BMI greater than 30
- Family history of cardiovascular disease
Of the above risk factors, smoking is associated with the highest risk of PAD development with an odds ratio of 2.7 (95% CI 2.4–3.1). History of cardiovascular disease and diabetes are also significant risk factors with odds ratios of 2.6 (95% CI 2.2-3) and 1.9 (1.7-2.1), respectively.[9]
Epidemiology
Peripheral vascular disease affects nearly 200 million people worldwide, including approximately 40 to 45 million Americans.[10] The disease is uncommon in younger populations; however, incidence increases sharply, with over 20% of people over 80 years old having PAD.[11] Data on gender differences is conflicting. In the Framingham study, intermittent claudication (IC) was more prevalent in men compared to women (1.9% to 0.8%; ratio 2.38).[12] This finding was consistent with the Rotterdam study that found men were 1.83 times more likely to have IC, with a prevalence of 2.2% in men and 1.2% in women.[13] However, a gender shift in prevalence occurs when the diagnosis of PAD is based on the ankle-brachial pressure index (ABI). For example, the Rotterdam study found the prevalence of ABI-based diagnosis of PAD to be 20.5% in women and 16.9% in adults, with a ratio of 0.82. Other studies, such as the Cardiovascular Health Study (CHS) and a population-based study, found no significant difference in ABI-based diagnosis of PAD between men and women. Proposed explanations for differences between ABI versus IC-defined PAD gender differences are that women are more likely to have atypical and late presentations and have intrinsically lower ABI values.[14]
Racial and socioeconomic disparities also exist. In regards to race, the CHS found African Americans to have an odds ratio of 2.12 for PAD compared to Non-Hispanic whites when adjusting for known risk factors.[15] The compilation of three studies addressing the impact of race on the risk of PAD found odds ratios of 2.3 to 3.1 for African Americans compared to Non-Hispanic whites when adjusting for confounders.[16] A socioeconomic survey study found patients with lower poverty-income ratios (PIR) to have a nearly 2 fold increase in the risk of PAD compared to higher PIR. Furthermore, the study found a lower educational level to be significantly associated with PAD (OR 2.8, 95% CI 1.96–4.0, p<0.0001).[17]
Pathophysiology
Peripheral vascular disease is primarily driven by the progression of atherosclerotic disease leading to macro and microvascular dysfunction. PAD typically affects the lower extremity vascular beds, but larger arteries, such as the abdominal aorta and iliac arteries, are frequently involved. More severe disease can involve multilevel and/or diffuse disease. The pathophysiology of atherosclerosis is a complex inflammatory response with the involvement of various vascular cells, thrombotic factors, and cholesterol and inflammatory molecules.
Atherosclerosis begins with lipoprotein accumulation within the intimal layer of large arteries. The lipoprotein presence within the endothelium leads to lipid oxidation and cytokine response with the infiltration of lymphocytes and macrophages.[18] Macrophages consume these oxidized lipids and form foam cells leading to the development of "fatty streaks."[19] Although not clinically significant, these fatty streaks can eventually develop into more advanced plaques consisting of necrotic lipid cores and smooth muscle cells (SMC). SMC and endothelial cells secrete cytokines and growth factors, leading to migration of SMC to the luminal side of the plaque and extracellular matrix synthesis and eventual formation of a fibrous plaque. Fibrous plaque stability is principally dependent on its composition, with more vulnerable plaques consisting of a thinner fibrous cap and more numerous inflammatory cells.
Atherosclerotic plaque builds up slowly over decades within the wall of the vessel. Plaque accumulation results in vascular stenosis and frequent vascular dilation to maximize end-organ perfusion. Once the vessel dilation capacity is maximized, the plaque continues to accumulate, which further compromises the lumen occasionally, leading to critical narrowing of the artery. As narrowing progresses and obstructs the artery, collateral circulatory beds frequently develop to preserve distal perfusion and tissue viability. These collateral circulatory pathways are unable to match the blood supply provided by a healthy vessel completely. IC results when blood flow distal to the occlusion is sufficiently compromised, resulting in fixed oxygen delivery that is unable to match oxygen demand.[20] The most severe form of PAD is critical limb ischemia, which is defined as limb pain at rest or impending limb loss.[21]
Acute ischemia may ensue if in-situ vascular thrombosis occurs or a cardioembolic source suddenly occludes the narrowed vessel.[22] Arterial thrombosis secondary to progressive atherosclerotic disease, and thrombosis represents 40% of acute limb ischemia (ALI) cases.[23] Atherosclerotic fibrous plaque rupture leads to exposure of subendothelial collagen and inflammatory cells, causing platelet adhesion and aggregation with rapid in-situ thrombosis of the vessel. Patients with in-situ vascular thrombosis tend to have improved outcomes compared to embolic causes due to the presence of extensive collateral circulation. Embolic ALI causes represent 30% of ALI cases, with the femoral artery being the most common site.[23] ALI is a vascular emergency with an immediate physician consultation required for the preservation of limb viability.
History and Physical
Diagnosis of peripheral vascular disease can be difficult due to the increasing prevalence of similarly presenting comorbid conditions and large numbers of patients having an asymptomatic or atypical presentation.[24] The clinical presentation of PAD is often dependent on the severity of arterial insufficiency and the presence of comorbid conditions, which may alter or mask the symptoms of underlying vascular disease.
Atypical presentation of PAD occurs when patients have existing comorbidities such as lumbosacral disease, spinal stenosis, or advanced diabetes mellitus - all of which may alter the perception of pain. Atypical pain is characterized by pain unrelated to physical activity, pain that occurs both at rest and exertion, and pain lasting longer than 10 minutes after exercise cessation.[25] Pseudo claudication refers to neuropathic pain observed in patients with spinal stenosis and can be differentiated from PAD with a thorough history and physical examination. Patients with pseudo claudication tend to have pain characterized by weakness and paresthesias that is irrespective of the degree of physical activity and usually is relieved by sitting down or changing body positioning rather than rest.[20]
Patients with hemodynamically significant PAD based on ABI testing are more likely to have asymptomatic rather than symptomatic disease. This illustrates the importance of maintaining a high clinical suspicion of underlying PAD for effective secondary prevention. Over 50% of patients with PAD are asymptomatic.[26] The prevalence of asymptomatic PAD may partly be explained by older individuals misinterpreting their symptoms as normal aging processes. Additionally, patients with mild to moderate PAD may be unable to exercise to a capacity where significant oxygen demand is required. Thus a mismatch between supply and demand does not occur, and patients remain asymptomatic.
Intermittent claudication is the most classic symptom of PAD, characterized by an exercise-induced cramping sensation with associated fatigue, weakness, and or pressure. It is not uncommon for patients to deny pain, and therefore asking about discomfort while ambulating is a more useful screening question. Symptoms are exacerbated by leg elevation and relieved by placing the limb in a dependent position. Paresthesias, lower extremity weakness, stiffness, and cool extremities may also be present. Anatomically the level of obstruction is usually seen one level above the area of discomfort; for example, patients with aortoiliac disease will have buttock and thigh symptoms. 70% to 80% of patients have stable intermittent claudication over 10 years; however, a portion of patients may progress through debilitating ischemic rest pain, critical limb ischemia, and eventual amputation.[27] Critical limb ischemia is manifested by pain at rest, nonhealing wounds or ulcers, and gangrene in one or both legs.
The physical exam begins with a general inspection with attention to fingernail tar indicative of cigarette smoking, scars from previous vascular surgeries, and the presence of amputations. A focused cardiovascular examination begins with a pulse examination to determine rate, rhythm, and strength. Chest auscultation should be performed to evaluate for pulmonary diseases such as chronic obstructive pulmonary disease (COPD) and pulmonary fibrosis, and heart sounds or murmurs. Neurological examination is essential to evaluate for pseudo claudication. Examination of the limbs should involve assessment for pulselessness, pallor, muscular atrophy, cool or cyanotic skin, or pain with palpation.[28] Lower extremity ulcers may be arterial, venous, neuropathic, or a combination of two or more. Ulcers secondary to arterial insufficiency are tender and typically have ragged borders with a dry base and pale or necrotic centers.
Evaluation
The diagnosis of peripheral vascular disease can be sufficiently made based on patient risk factors, clinical presentation, and physical exam findings. Occasionally patients can present with atypical symptoms, and objective data can establish the diagnosis. Assessment begins with accounting for known PAD risk factors, including smoking, diabetes, hypertension, hypercholesterolemia, and obesity. Intermittent claudication must be distinguished from neurological, musculoskeletal, or vascular disorders, which may present similarly to PAD. Physical exam findings of the lower extremities may demonstrate shiny skin with coolness to palpation, reduced or absent pulses, abnormal capillary refill time, pallor with leg elevation, dependent rubor, and auscultation of bruits in major vessels, including the femoral and popliteal arteries.[29] Advanced disease may manifest as nonhealing ulcers or gangrene.
Measurement of the ankle-brachial index (ABI) is a cost-effective noninvasive objective measure for PAD diagnosis. The ABI is obtained by measuring the systolic ankle pressure ratio to the systolic brachial pressure. The test is performed by placing a blood pressure cuff above the level of the ankle and placing a Doppler ultrasonography probe on the dorsalis pedis or posterior tibialis and then inflating the cuff until the signal from the probe ceases. The cuff is then slowly deflated, and the return of the Doppler probe signal marks the systolic ankle pressure. The process is then repeated for the opposite leg. The ankle pressure of each leg is then divided by the highest systolic pressure of either brachial artery. A normal ABI ratio ranges from 0.9 to 1.2, and values less than 0.9 are diagnostic of PAD. Noncompressible vessels, as seen in people with diabetes and those with advanced kidney disease and may have falsely elevated ratios.[30] Individuals with abnormally high ABI ratios have higher all-cause mortality compared to normal ABI ratios. Further diagnostic evaluation for these patients often warrants a toe-brachial index (TBI), which is the comparison of the toe systolic pressure to the higher systolic brachial pressure.[20] These particular patients illustrate the vital importance of clinical history and physical examination in the initial evaluation of patients with suspected PAD.
Duplex ultrasonography is a safe and cost-effective method of determining PAD location, stenosis severity, and length of stenosis or occlusion. 2-dimensional imaging, along with color Doppler, provides an accurate assessment of lesion stenosis, hemodynamic severity, and plaque characteristics. Doppler ultrasonography can be used in routine follow-up post-procedure for surveillance of patency. This diagnostic modality can assist in decision-making when further intervention is contemplated.[31]
Magnetic resonance angiography (MRA) or computed tomography angiography (CTA) both provide excellent high-quality vascular imaging. The advantages of MRA include the ability to identify small runoff vessels that sometimes may not be seen with digital subtraction angiography (DSA). Compared with DSA, MRA has 90% sensitivity and 97% specificity in identifying hemodynamically significant lesions.[31] CTA has similar diagnostic accuracy to MRA, with both imaging techniques useful for determining candidacy for bypass surgery versus angioplasty.
Treatment / Management
Patients diagnosed with peripheral vascular disease require a reasoned approach to account for age, risk factors, disease severity, and functional status. Management is divided into two broad categories aimed at decreasing cardiovascular events and improving symptoms. Persons with PAD are at increased risk of coronary artery disease mortality (relative risk = 6.6), cardiovascular mortality (relative risk = 5.9), and all-cause mortality (relative risk = 3.1).[32] Therefore PAD management begins with lifestyle modification to prevent disease progression with the addition of medical and interventional therapy required for improved symptomatic control and cardiovascular event risk reduction.
Cardiovascular Risk Factor Modification
Aggressive risk factors modification is essential to lowering cardiovascular risk. Smoking cessation reduces the risk of PAD progression, cardiovascular events, including myocardial infarction and stroke, and critical limb ischemia.[33] Patient education, along with the use of behavioral therapy, nicotine replacement therapy, or pharmacological therapy, can be used to reduce smoking and improve cardiovascular outcomes. Statin therapy has been effectively shown to reduce cardiovascular events and all-cause mortality and reduce the need for revascularization and should be routinely used in patients with PAD. Hypertension management with blood pressure reduction to less than 140/90 in nondiabetic and 130/80 in diabetic patients has been shown to improve outcomes.[34] Diabetes is a risk factor for symptomatic and asymptomatic PAD by 1.5 to 4 fold, respectively, and a hemoglobin A1c target of less than 7% should be achieved with less stringent goals for individuals with extensive comorbidities.[35](B3)
Exercise Therapy
Randomized trials have shown supervised exercise therapy programs to have significant improvement in claudication symptoms. A meta-analysis of 27 studies found exercise significantly improved pain-free walking distance by 269 feet and total walking distance by nearly 400 feet.[36] Exercise programs typically consist of 30- to 45-minute length sessions conducted 4 to 5 times a week over the course of 12 weeks. A meta-analysis of five trials found no improvement in mortality with exercise therapy programs.[36](A1)
Pharmacotherapy
Pharmacological therapy for intermittent claudication (IC) management can be offered to patients who have not benefited from exercise therapy and risk factor modification.[37] Two medications approved for IC treatment include cilostazol and naftidrofuryl. Cilostazol inhibits phosphodiesterase type 3 and has demonstrated antiplatelet effect, vasodilatory properties, and inhibition of smooth muscle cell proliferation.[38] A meta-analysis of over 2000 patients found individuals on cilostazol had significantly longer pain-free and total walking distances.[38] Naftidrofuryl is a 5-hydroxytryptamine-2-receptor antagonist that inhibits glucose uptake and increases adenosine triphosphate levels. It has fewer side effects than cilostazol and should be considered where available.[39](A1)
Daily aspirin is recommended for overall cardiovascular care. No consensus has been reached on the most effective dose.
Revascularization
Patients who have debilitating symptoms unresponsive to risk factor modification and exercise and pharmacological therapy may be candidates for endovascular, surgical, or combined endovascular and surgical intervention. Indications for intervention include individuals with incapacitating claudication interfering with daily activity and limb salvage in patients with critical limb ischemia manifested by ischemic pain at rest, ulceration, and gangrene. The decision on surgical versus percutaneous intervention is dependent on many factors, including the patient's functional status and surgical risk, skills of the operator, anatomic location and extent of disease, presence of multifocal vascular lesions, and patient preference.[40] An interprofessional team approach involving an internist, interventionalist, and vascular surgeon should be undertaken for personalized patient care to improve outcomes and patient satisfaction.
Differential Diagnosis
A provider has to take into account various differential diagnoses when a patient presents with the above-mentioned signs and symptoms. Following are some of the most important ones:
Neurological
- Nerve root compression
- Spinal stenosis
- Peripheral neuropathy
- Nerve entrapment
Musculoskeletal
- Medial tibial stress syndrome
- Osteoarthritis
- Muscle strain
- Baker cyst
Vascular
- Chronic venous insufficiency
- Thrombophlebitis
- Deep venous thrombosis
- Raynaud phenomenon
- Thromboangiitis obliterans
Prognosis
The overall prognosis of patients with peripheral vascular disease must take into account patient risk factors, cardiovascular health, and disease severity. In terms of limb health at 5 years, nearly 80% of patients will have stable claudication symptoms. Only 1% to 2% of patients will progress to critical limb ischemia in 5 years. 20 to 30% of patients with PAD will die within 5 years, with 75% of those deaths attributed to cardiovascular causes.[32]
Complications
Peripheral vascular disease can affect several systems in the body leading to a number of complications as listed below:
- Acute coronary syndrome
- Stroke
- Nonhealing ulcer
- Gangrene
- Amputation
- Deep vein thrombosis
- Erectile dysfunction
Consultations
- Vascular surgery
- Interventional cardiology
- Endocrinology
- Radiology
- Internal medicine
Deterrence and Patient Education
Patient management for the desired outcomes is based on a holistic approach that includes non-pharmacological lifestyle modification and pharmacological management, such as:
- Smoking cessation
- Ambulatory blood pressure monitoring
- Medication and exercise therapy compliance
- Cholesterol management through diet and statin therapy
- Weight reduction
- HbA1c goal of less than 7% (or more for significant comorbid conditions or hypoglycemia)
- Regular follow up with an interprofessional team
Enhancing Healthcare Team Outcomes
Peripheral arterial disease is a progressive systemic disease with poor long-term outcomes. Although symptoms of claudication remain stable for many years, these patients are at high risk of fatal and nonfatal cardiovascular events. Interprofessional coordination is necessary for identifying patients at risk of disease, preventing secondary progression, and presenting patients with various options for their disease. Primary care providers are essential for patient education regarding risk factors for cardiovascular disease and management of tobacco abuse, hypercholesterolemia, hypertension, and diabetes mellitus. Cardiologists should be involved, given nearly 75% of patients with PAD die from cardiovascular events. Vascular surgeons and endovascular specialists' input provides patients with various options for refractory disease. Vascular medicine specialists and podiatrists are very frequently vital members of the interprofessional team. Nurses are valuable for their familiarity with the patient and for updates on how the patient's condition has progressed. Pharmacists are needed for patient and physician education on potential medication side effects and drug-to-drug interactions.
Current guidelines by the American College of Cardiology recommend patients with symptoms of IC undergo ABI testing. [Level 2] Patients diagnosed with PAD and unresponsive to exercise therapy should receive cilostazol for symptomatic improvement and increased walking distance. [Level I] Endovascular procedures are recommended in patients who have not responded to exercise and pharmacological therapy and who have debilitating symptoms.[34] [Level 1]
Media
(Click Image to Enlarge)

Peripheral Arterial Disease Non-healing necrotic ulceration and gangrene of the 3rd digit secondary to PAD. Contributed by Mark A. Dreyer, DPM, FACFAS
(Click Image to Enlarge)
Peripheral Arterial Disease - High Grade Stenosis of Dorsalis Pedis Artery of the foot. Contribution by Mark A. Dreyer, DPM, FACFAS
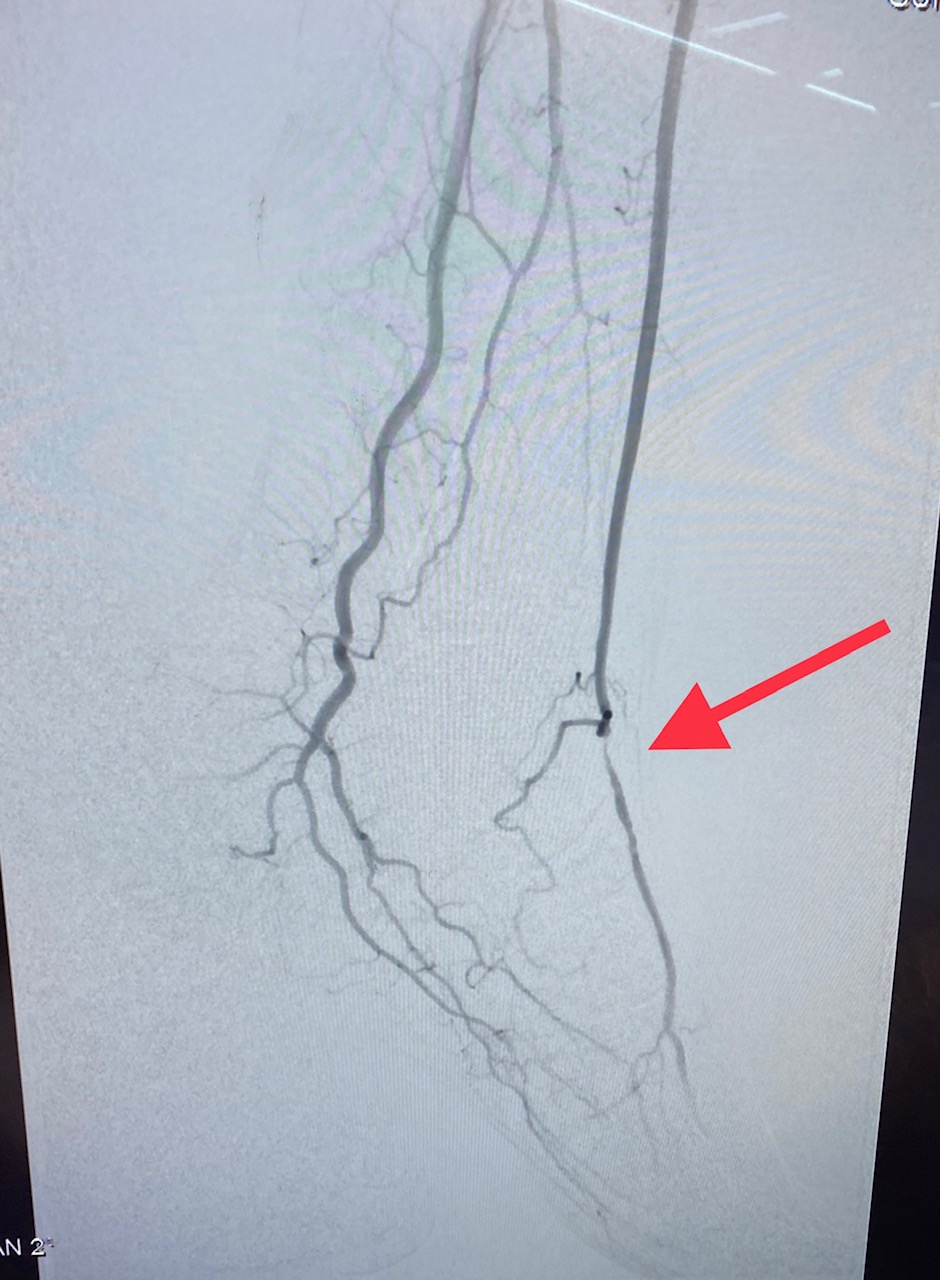
(Click Image to Enlarge)
Peripheral Arterial Disease - Chronic Total Occlusion of Left Superficial Femoral Artery Contribution by Mark A. Dreyer, DPM, FACFAS
(Click Image to Enlarge)
Peripheral Arterial Disease - Chronic Total Occlusion of Left Superficial Femoral Artery after atherectomy. Contribution by Mark A. Dreyer, DPM, FACFAS
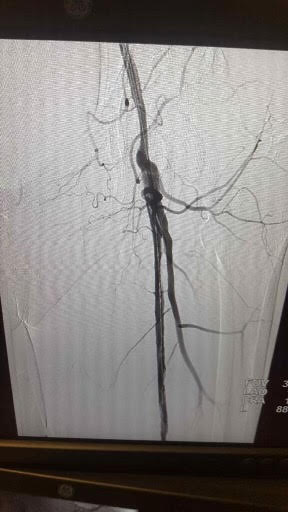
(Click Image to Enlarge)

Peripheral Arterial Disease - Occluded anterior tibial artery Contribution by Mark A. Dreyer, DPM, FACFAS
References
European Stroke Organisation, Tendera M, Aboyans V, Bartelink ML, Baumgartner I, Clément D, Collet JP, Cremonesi A, De Carlo M, Erbel R, Fowkes FG, Heras M, Kownator S, Minar E, Ostergren J, Poldermans D, Riambau V, Roffi M, Röther J, Sievert H, van Sambeek M, Zeller T, ESC Committee for Practice Guidelines. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: the Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). European heart journal. 2011 Nov:32(22):2851-906. doi: 10.1093/eurheartj/ehr211. Epub 2011 Aug 26 [PubMed PMID: 21873417]
Meijer WT, Grobbee DE, Hunink MG, Hofman A, Hoes AW. Determinants of peripheral arterial disease in the elderly: the Rotterdam study. Archives of internal medicine. 2000 Oct 23:160(19):2934-8 [PubMed PMID: 11041900]
Fowkes FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UK, Williams LJ, Mensah GA, Criqui MH. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet (London, England). 2013 Oct 19:382(9901):1329-40. doi: 10.1016/S0140-6736(13)61249-0. Epub 2013 Aug 1 [PubMed PMID: 23915883]
Level 1 (high-level) evidenceKrishna SM, Moxon JV, Golledge J. A review of the pathophysiology and potential biomarkers for peripheral artery disease. International journal of molecular sciences. 2015 May 18:16(5):11294-322. doi: 10.3390/ijms160511294. Epub 2015 May 18 [PubMed PMID: 25993296]
Subherwal S, Patel MR, Kober L, Peterson ED, Bhatt DL, Gislason GH, Olsen AM, Jones WS, Torp-Pedersen C, Fosbol EL. Peripheral artery disease is a coronary heart disease risk equivalent among both men and women: results from a nationwide study. European journal of preventive cardiology. 2015 Mar:22(3):317-25. doi: 10.1177/2047487313519344. Epub 2014 Jan 7 [PubMed PMID: 24398369]
Wakabayashi I, Sotoda Y. [Alcohol drinking and peripheral arterial disease of lower extremity]. Nihon Arukoru Yakubutsu Igakkai zasshi = Japanese journal of alcohol studies & drug dependence. 2014 Feb:49(1):13-27 [PubMed PMID: 24818355]
Periard D, Cavassini M, Taffé P, Chevalley M, Senn L, Chapuis-Taillard C, de Vallière S, Hayoz D, Tarr PE, Swiss HIV Cohort Study. High prevalence of peripheral arterial disease in HIV-infected persons. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2008 Mar 1:46(5):761-7. doi: 10.1086/527564. Epub [PubMed PMID: 18230043]
Level 2 (mid-level) evidenceKhandanpour N, Loke YK, Meyer FJ, Jennings B, Armon MP. Homocysteine and peripheral arterial disease: systematic review and meta-analysis. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2009 Sep:38(3):316-22. doi: 10.1016/j.ejvs.2009.05.007. Epub 2009 Jun 27 [PubMed PMID: 19560951]
Level 1 (high-level) evidencePrabhakaran D, Anand S, Gaziano TA, Mbanya JC, Wu Y, Nugent R, Sampson UKA, Fowkes FGR, Naidoo NG, Criqui MH. Peripheral Artery Disease. Cardiovascular, Respiratory, and Related Disorders. 2017 Nov 17:(): [PubMed PMID: 30212080]
Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Jordan LC, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, O'Flaherty M, Pandey A, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Spartano NL, Stokes A, Tirschwell DL, Tsao CW, Turakhia MP, VanWagner LB, Wilkins JT, Wong SS, Virani SS, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation. 2019 Mar 5:139(10):e56-e528. doi: 10.1161/CIR.0000000000000659. Epub [PubMed PMID: 30700139]
Shu J, Santulli G. Update on peripheral artery disease: Epidemiology and evidence-based facts. Atherosclerosis. 2018 Aug:275():379-381. doi: 10.1016/j.atherosclerosis.2018.05.033. Epub 2018 May 22 [PubMed PMID: 29843915]
Kannel WB, McGee DL. Update on some epidemiologic features of intermittent claudication: the Framingham Study. Journal of the American Geriatrics Society. 1985 Jan:33(1):13-8 [PubMed PMID: 3965550]
Murabito JM, Evans JC, Nieto K, Larson MG, Levy D, Wilson PW. Prevalence and clinical correlates of peripheral arterial disease in the Framingham Offspring Study. American heart journal. 2002 Jun:143(6):961-5 [PubMed PMID: 12075249]
Level 2 (mid-level) evidenceAboyans V, Criqui MH, McClelland RL, Allison MA, McDermott MM, Goff DC Jr, Manolio TA. Intrinsic contribution of gender and ethnicity to normal ankle-brachial index values: the Multi-Ethnic Study of Atherosclerosis (MESA). Journal of vascular surgery. 2007 Feb:45(2):319-27 [PubMed PMID: 17264011]
Level 2 (mid-level) evidenceNewman AB, Siscovick DS, Manolio TA, Polak J, Fried LP, Borhani NO, Wolfson SK. Ankle-arm index as a marker of atherosclerosis in the Cardiovascular Health Study. Cardiovascular Heart Study (CHS) Collaborative Research Group. Circulation. 1993 Sep:88(3):837-45 [PubMed PMID: 8353913]
Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circulation research. 2015 Apr 24:116(9):1509-26. doi: 10.1161/CIRCRESAHA.116.303849. Epub [PubMed PMID: 25908725]
Pande RL, Creager MA. Socioeconomic inequality and peripheral artery disease prevalence in US adults. Circulation. Cardiovascular quality and outcomes. 2014 Jul:7(4):532-9 [PubMed PMID: 24987053]
Level 2 (mid-level) evidenceRafieian-Kopaei M, Setorki M, Doudi M, Baradaran A, Nasri H. Atherosclerosis: process, indicators, risk factors and new hopes. International journal of preventive medicine. 2014 Aug:5(8):927-46 [PubMed PMID: 25489440]
Lusis AJ. Atherosclerosis. Nature. 2000 Sep 14:407(6801):233-41 [PubMed PMID: 11001066]
Level 3 (low-level) evidenceOlin JW, Sealove BA. Peripheral artery disease: current insight into the disease and its diagnosis and management. Mayo Clinic proceedings. 2010 Jul:85(7):678-92. doi: 10.4065/mcp.2010.0133. Epub [PubMed PMID: 20592174]
Varu VN, Hogg ME, Kibbe MR. Critical limb ischemia. Journal of vascular surgery. 2010 Jan:51(1):230-41. doi: 10.1016/j.jvs.2009.08.073. Epub [PubMed PMID: 20117502]
Kim HO, Kim W. Elucidation of the Diagnosis and Treatment of Peripheral Arterial Disease. Korean circulation journal. 2018 Sep:48(9):826-827. doi: 10.4070/kcj.2018.0155. Epub 2018 Jun 11 [PubMed PMID: 30088357]
Olinic DM, Stanek A, Tătaru DA, Homorodean C, Olinic M. Acute Limb Ischemia: An Update on Diagnosis and Management. Journal of clinical medicine. 2019 Aug 14:8(8):. doi: 10.3390/jcm8081215. Epub 2019 Aug 14 [PubMed PMID: 31416204]
Dhaliwal G, Mukherjee D. Peripheral arterial disease: Epidemiology, natural history, diagnosis and treatment. The International journal of angiology : official publication of the International College of Angiology, Inc. 2007 Summer:16(2):36-44 [PubMed PMID: 22477268]
McDermott MM, Greenland P, Liu K, Guralnik JM, Criqui MH, Dolan NC, Chan C, Celic L, Pearce WH, Schneider JR, Sharma L, Clark E, Gibson D, Martin GJ. Leg symptoms in peripheral arterial disease: associated clinical characteristics and functional impairment. JAMA. 2001 Oct 3:286(13):1599-606 [PubMed PMID: 11585483]
Level 2 (mid-level) evidenceHøyer C, Sandermann J, Petersen LJ. The toe-brachial index in the diagnosis of peripheral arterial disease. Journal of vascular surgery. 2013 Jul:58(1):231-8. doi: 10.1016/j.jvs.2013.03.044. Epub 2013 May 18 [PubMed PMID: 23688630]
Dormandy JA, Rutherford RB. Management of peripheral arterial disease (PAD). TASC Working Group. TransAtlantic Inter-Society Consensus (TASC). Journal of vascular surgery. 2000 Jan:31(1 Pt 2):S1-S296 [PubMed PMID: 10666287]
Level 1 (high-level) evidenceBailey MA, Griffin KJ, Scott DJ. Clinical assessment of patients with peripheral arterial disease. Seminars in interventional radiology. 2014 Dec:31(4):292-9. doi: 10.1055/s-0034-1393964. Epub [PubMed PMID: 25435653]
Hennion DR, Siano KA. Diagnosis and treatment of peripheral arterial disease. American family physician. 2013 Sep 1:88(5):306-10 [PubMed PMID: 24010393]
Resnick HE, Lindsay RS, McDermott MM, Devereux RB, Jones KL, Fabsitz RR, Howard BV. Relationship of high and low ankle brachial index to all-cause and cardiovascular disease mortality: the Strong Heart Study. Circulation. 2004 Feb 17:109(6):733-9 [PubMed PMID: 14970108]
Olin JW, Kaufman JA, Bluemke DA, Bonow RO, Gerhard MD, Jaff MR, Rubin GD, Hall W, American Heart Association. Atherosclerotic Vascular Disease Conference: Writing Group IV: imaging. Circulation. 2004 Jun 1:109(21):2626-33 [PubMed PMID: 15173045]
Criqui MH, Langer RD, Fronek A, Feigelson HS, Klauber MR, McCann TJ, Browner D. Mortality over a period of 10 years in patients with peripheral arterial disease. The New England journal of medicine. 1992 Feb 6:326(6):381-6 [PubMed PMID: 1729621]
Jonason T, Bergström R. Cessation of smoking in patients with intermittent claudication. Effects on the risk of peripheral vascular complications, myocardial infarction and mortality. Acta medica Scandinavica. 1987:221(3):253-60 [PubMed PMID: 3591463]
Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, Hiratzka LF, Murphy WR, Olin JW, Puschett JB, Rosenfield KA, Sacks D, Stanley JC, Taylor LM Jr, White CJ, White J, White RA, Antman EM, Smith SC Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Hunt SA, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B, American Association for Vascular Surgery, Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, ACC/AHA Task Force on Practice Guidelines Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease, American Association of Cardiovascular and Pulmonary Rehabilitation, National Heart, Lung, and Blood Institute, Society for Vascular Nursing, TransAtlantic Inter-Society Consensus, Vascular Disease Foundation. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006 Mar 21:113(11):e463-654 [PubMed PMID: 16549646]
Level 3 (low-level) evidenceAmerican Diabetes Association. 2. Classification and Diagnosis of Diabetes. Diabetes care. 2016 Jan:39 Suppl 1():S13-22. doi: 10.2337/dc16-S005. Epub [PubMed PMID: 26696675]
Lane R, Harwood A, Watson L, Leng GC. Exercise for intermittent claudication. The Cochrane database of systematic reviews. 2017 Dec 26:12(12):CD000990. doi: 10.1002/14651858.CD000990.pub4. Epub 2017 Dec 26 [PubMed PMID: 29278423]
Level 1 (high-level) evidenceSociety for Vascular Surgery Lower Extremity Guidelines Writing Group, Conte MS, Pomposelli FB, Clair DG, Geraghty PJ, McKinsey JF, Mills JL, Moneta GL, Murad MH, Powell RJ, Reed AB, Schanzer A, Sidawy AN, Society for Vascular Surgery. Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. Journal of vascular surgery. 2015 Mar:61(3 Suppl):2S-41S. doi: 10.1016/j.jvs.2014.12.009. Epub 2015 Jan 28 [PubMed PMID: 25638515]
Level 1 (high-level) evidenceThompson PD, Zimet R, Forbes WP, Zhang P. Meta-analysis of results from eight randomized, placebo-controlled trials on the effect of cilostazol on patients with intermittent claudication. The American journal of cardiology. 2002 Dec 15:90(12):1314-9 [PubMed PMID: 12480040]
Level 1 (high-level) evidenceNorgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, TASC II Working Group. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Journal of vascular surgery. 2007 Jan:45 Suppl S():S5-67 [PubMed PMID: 17223489]
Level 3 (low-level) evidenceComerota AJ. Endovascular and surgical revascularization for patients with intermittent claudication. The American journal of cardiology. 2001 Jun 28:87(12A):34D-43D [PubMed PMID: 11434898]