Introduction
The use of point-of-care ultrasound (POCUS) has expanded considerably over the past two decades allowing for enhanced and swift evaluations, rapid triage, improved diagnostic capabilities in austere situations, and real-time assessment of focused clinical questions in critically ill patients in the intensive care unit (ICU).[1] Emergency medicine physicians have led the way in establishing and educating bedside use of ultrasound. In 2001, the American College of Emergency Physicians (ACEP) published the first Emergency Ultrasound Guidelines to clarify the primary indications, the scope of practice, training, and continuing education regarding the use of emergency ultrasound.[2]
These guidelines have continued to expand alongside the ever-growing use of ultrasound. They have been adopted by several other specialties, especially in applying “procedural ultrasound” to assist in real-time guidance of vascular access, peripheral nerve blockade, and pre-surgical evaluations.[3][4]
The main difference between POCUS and dedicated ultrasound exams is the ability to rapidly answer a focused clinical question, facilitate serial examinations in clinical deterioration, or guide a bedside procedure rather than provide a detailed report with the grading of pathology.[2][5] With small, portable ultrasound models becoming available, advanced diagnostics are becoming more accessible in remote environments and on the battlefield. Physicians and advanced paramedical providers in these settings are becoming trained to perform extended focused assessment with sonography in trauma (eFAST), optic nerve sheath ultrasound (ONSUS) for the evaluation of intracranial hypertension, inferior vena cava collapsibility assessments for the evaluation of volume status, and countless other examples of image-guided procedures.[6][7] This article will focus on optic nerve sheath ultrasound for the diagnosis, monitoring, and management of elevated intracranial pressure (ICP).
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The eye is an ideal configuration for ultrasound imaging as it is superficial with well-demarcated fluid-filled structures that serve as an excellent medium for ultrasound beam transduction. At least a basic understanding of ocular anatomy is required to perform an ONSUS. Identifying anterior structures will increase success in measuring the optic nerve sheath in the correct plane.
The eyeball rests in a membranous sac called the Tenon capsule, surrounded by periocular fat, soft tissue, and the orbital walls. It attaches via the corneoscleral junction and the optic nerve, with extraocular muscle tendons piercing the Tenon sac, inserting into the sclera, and allowing for eyeball mobility on multiple axes. Two fluid-filled structures that require identification in the study include the anterior chamber (AC) and posterior chamber (PC), which are separated by the lens and both harbor anechoic fluid. Posterior to the PC is the retina with a hyperechoic nervous membrane.[8]
Posterior to the retina and optic disc, one can identify the optic nerve by its anechoic core, flanked by a hyperechoic sheath on the medial and lateral borders in the transverse plane. The optic nerve can be thought of as an outpouching of intact brain tissue with the intraorbital component fully encapsulated by dura, arachnoid, and pia matter, allowing the optic nerve sheath to transmit cerebral spinal fluid and fluctuate in size based on changes in intracranial pressure.[9][10] The meningeal cover of the optic nerve is the continuation of the dural and subarachnoid space.[11] The bulbous portion of the optic nerve, approximately 3 mm posterior to the globe, appears to be the most distensible and sensitive to changes in ICP based on in-vivo models of elevated ICP and artificial creations of elevated ICP in cadaveric models.[9][12]
The upper limit of the normal ONSD includes:
- 4 mm in infants.
- 5 mm in children.
- 5 mm in adults.
ONSD shows linear increment till 7.5 mm, after which it plateaus off.[13]
Indications
Ocular ultrasound can be performed for various reasons, including vision loss, headache, and trauma. It can be very beneficial in identifying or excluding retinal detachment, foreign bodies, lens dislocation, vitreous hemorrhage, and other superficial abnormalities that can cause loss of eyesight. ONSUS is usually performed in the setting of suspected or confirmed traumatic brain injury (TBI), intracranial hypertension, or optic neuritis.[14] ONSUS is non-invasive and avoids the risk of infection, hemorrhage, or ionizing radiation that are inevitable with intracranial monitors and computed tomography (CT).[15]
ONSUS can also be used to help “rule out” elevated ICP in non-acute trauma settings, such as troubleshooting a malfunctioning intraventricular device, before or following lumbar punctures, or while evaluating the safety of neuraxial anesthesia in patients with a previous history of elevated ICP. It should be emphasized that these readings should be evaluated in the overall clinical context, as such applications are not well studied or validated.[16][17][18][19][20]
ONSD is currently considered the best non-invasive modality for dynamic estimation of ICP.[21] POCUS measurements have shown ONSD to be significantly correlating with ICP.[22] ICP can be calculated using the formula ONSD: nICPONSD = 5.00 × ONSD − 13.92 mmHg.[23] This is a holy grail in assessing critical patients in whom invasive ICP monitoring is either unavailable or is contraindicated.[21] This has been found helpful in the evaluation of the following cohorts of patients:
- Idiopathic intracranial hypertension.[24][25]
- Intracranial hypotension.[26]
- Hypoxic-ischemic encephalopathy.[11]
- Perioperative neurosurgical patients.[27]
- Shunt evaluation.[28]
- Head injury.[29]
- Ischemic strokes- With every 0.1 cm increment in ONSD, the odds ratio for mortality increased 4.2 times.[30][31]
- Hematoma progression in hemorrhagic strokes.[32]
Contraindications
Surface ultrasound remains a safe modality with little to no risk to adult patients. However, if an open globe injury is suspected, there is potential for further ocular injury, and the study should not proceed without consultation or assistance from an ophthalmologist.[33][34]
Equipment
The advantage of ONSUS is that it can be performed with most ultrasound equipment that is abundantly available in emergency departments and ICUs throughout the United States. There are commercially available high-frequency ocular ultrasound units designed for dedicated studies of the eye, but most conventional ultrasound units with a high frequency (7 to 10 MHz or higher) linear array probes are sufficient to visualize the optic nerve with the closed eye technique.[35][36] Additional equipment may include a clear sterile intravenous catheter adhesive to create a barrier and ultrasound gel as a conduction medium.
Personnel
Typically, ONSUS can be performed by an individual and requires no additional assistance in patient positioning. Depending on space constraints, it can be useful to have an assistant familiar with ultrasound to capture images, adjust depth, gain, and other functions to optimize imaging.
Preparation
Awake and alert patients should be briefed on the procedure. Obtunded, intubated, or heavily sedated patients should have a gross eye evaluation for signs and symptoms of globe rupture or hyphema. If there is evidence of globe rupture, including visible conjunctival or scleral defect, severe chemosis, 360-degree conjunctival hemorrhage, hypotony, or total hyphema, the procedure should be aborted to avoid further herniation of intraocular contents, and an ophthalmologist should be consulted.[37][38]
It can be beneficial to instruct awake patients to "look ahead" with a closed eye or to examine the eye orientation in obtunded patients before the procedure to orient the ultrasound beam in the transverse plane and avoid oblique slices of the optic nerve. Some practitioners will apply petroleum jelly or ophthalmic ointment to the eyes to avoid air trapping before applying a clear plastic adhesive dressing. Ultrasound gel should be applied liberally to the adhesive before scanning.[39]
The patient's position should be dictated by comfort and ease of examination but will typically be done in the supine to 30 degrees "head up" position. Although theoretical concerns may exist for changes in ICP and ocular nerve sheath diameter (ONSD) relative to patient position and ventilator settings, these changes do not appear to manifest in in-vivo models.[40][41] Several small studies have shown no significant change in ONSD with changes to patient position, the elevation of positive end-expiratory pressure, or even the artificial creation of pneumoperitoneum in laparoscopic surgeries.[42][43][44]
Technique or Treatment
After applying a sterile dressing over a closed eye and copious ultrasound gel, the high-frequency ultrasound transducer should be placed over the eye with little to no contact with the sterile dressing in the transverse plane. The sonographer's hand should be placed on a non-compressible surface (the patient's nose, midface, or forehead) to avoid direct globe pressure, discomfort, and distortion of anatomy. Small movements nasally and temporally followed by caudad and cephalad should be executed to capture the optic nerve sheath in the same plane as the AC, PC, and lens to avoid obliquing the image. Once the anechoic streak posterior to the optic disc is visualized, the image should be captured, and measurements can be taken from the saved image. The optic nerve is relatively cylindrical and symmetric, theoretically making a single view acceptable for measurement.[14]
However, the dogma of "one view is no view" should be applied in all ultrasonographic studies, and another image should be captured in the sagittal plane. After measuring 3 mm posterior to the globe, use electronic calipers to measure the distance of decreased echogenicity between the hyperechoic demarcations of the sheath. A large discrepancy between images captured in separate planes should alert the sonographer to possible artefactual or off-axis errors, and they should rescan in both planes. Once optimal images are captured in two planes, the mean should be determined to estimate the true ONSD. Both eyes should be scanned, and bilateral measurements should be considered.
If difficulty in acquiring an image during the ultrasound study is encountered, one should try to center the focal ultrasound beam transversely through the plane of the lens. The contralateral eye can be assessed to estimate the location and orientation of the pupil on the studied eye. Increasing the volume of an ultrasound gel buffer can improve the quality of the image. Increasing the gain can help enhance discernment between the actual nerve sheath and nerve. Color Doppler can help visualize the retinal artery near the posterior globe as a reference point.
Once the optic nerve sheath diameter is determined, it requires evaluation in the overall clinical context. Earlier studies have most commonly used a cutoff of 5.0 mm with excellent sensitivity as well as positive and negative predictive values, but cutoffs correlating to elevations of ICP greater than 20 mm Hg have varied from less than 5 mm to greater than 6 mm in different papers. One meta-analysis of 12 studies that compared optic nerve sheath values to CT evidence of elevated ICP yielded a specificity of 92.3% and a sensitivity of 95.6% utilizing a 5 mm cutoff in adult patients.[45]
A-mode Vs. B-mode Scan
A-mode scan is ideally advocated owing to the 'blooming' artifact during the B-mode scan.[46][47] However, it is easy to choose a distance on the optic nerve behind the globe in the B-mode scan. The B-mode scan is also easy when assessing non-compliant patients.[47] There is no significant difference in ONSD measurements with straight or lateral gaze tests on B-mode studies.[47]
Point of Measurement of ONSD
Three millimeters posterior to the globe corresponds to the bulbous (wide) portion of the optic nerve and is the site of maximum pressure changes within the nerve.[48][49][50][51] One study showed an area under the curve (AUC) of 0.956 for ONSD at 3 mm. Some studies, however, have shown no significant differences during the measurement of ONSD between 3 and 5 mm.[52]
The basic steps in measuring ONSD using ocular ultrasound can be summarized as follows:
- Supine positioning of the patient.
- The high-frequency linear probe (which allows better contrast between the nerve and the retro bulbar fat) is placed on the closed upper eyelid after applying a gel.[53]
- Acoustic output needs to be adjusted ALARA ('as low as reasonably achievable) principle to protect the lens and retina.
- The probe needs to be adjusted to display the entry of the optic nerve into the globe.
- ONSD measurement needs to be ideally taken 3 mm behind the eye globe. The point where the optic nerve and the ophthalmic artery cross is also recommended.
- Multiple values for each eye and then averaged to reduce the risk of deviation.[11][50][53]
- Same equipment, methodology, window, contrast, and brightness are advocated.[51]
Complications
ONSUS is safe and benign in the absence of an open globe. However, if an open globe injury is suspected, there is potential for further ocular injury, and the study should not proceed without consultation or assistance from an ophthalmologist.[33][34] It is worth noting that despite the reasonably good sensitivity and specificity shown in several studies, imagining the optic nerve sheath in the traditional visual axis, and even the mean measurements of the ONSD captured in the transverse and sagittal plane, have been questioned by several authors.
Copetti et al. challenge that conventional views of the optic nerve sheath in several studies are more likely to be an artifact (potentially acoustic shadow cast from the lamina cribrosa) rather than the optic nerve itself. False positives, created by artifacts or excessive pressure on the globe itself, could result in unmerited treatment, invasive monitoring, or additional unindicated studies. Copetti suggests utilizing color doppler to identify the retinal artery and measuring the optic nerve from the lateral position.[54]
Clinical Significance
There are broad applications of ONSUS in both advanced medical centers and battlefield environments. It is often difficult and potentially life-threatening to transport critically ill intensive care unit patients to radiology suites. The mortality rate of inter-hospital transfer of critically ill patients has been reported as high as 2%, with adverse event rates as high as 68%.[55] Several studies have shown that CT scans usually result in therapeutic changes in only about half of all cases (39% to 68%); only judicious use of ICU radiographic studies should be considered.[56][57]
Head CT accounts for more than 25% of ICU inter-hospital transports, and depending on the indication, ONSUS may be a modality in improving the decision-making process for obtaining such imaging.[58] If a multisystem trauma patient with a known, stable intracranial hemorrhage and known baseline ONSD experiences a neurological decline in the ICU, it could potentially be worthwhile to perform serial ONSUS on the patient to rule out intracranial hypertension or herniation if the risks of transport are significant and evolution of the hemorrhage without intracranial hypertension would not change management. This is why it is paramount to perform early, and frequent ONSUS in patients at risk for developing increased ICP, as a significant change in ONSD is far more suggestive of changes in ICP than a single absolute number.
Medics and physicians have used ultrasound in many environments, including high altitude, polar, battlefield, and in-flight expeditions, when other imaging is not readily available.[7] Traumatic brain injury (TBI) remains a common battlefield injury, with over 200000 DoD-reported cases between 2010 to 2018. Over 80% of these TBIs are classified as mild and do not require neurosurgical intervention, but evaluation in austere locations can be difficult.[59]
ONSUS provides the ability for rapid triage and the minimally invasive evaluation of intracranial hypertension in an equivocal clinical setting and provides useful data for the early medical treatment of intracranial hypertension while arranging evacuation to definitive neurosurgical care. Though ONSUS is not specifically mentioned by the most recent Joint Trauma System Clinical Practice Guideline on Traumatic Brain/Severe Head Injury (2 March 2017), the authors note that “treatment of known or suspected intracranial hypertension remains a cornerstone of therapy in patients with severe brain injury.” Further recommendations are that after conservative management (head of the bed elevation 30 to 45 degrees, SBP goals greater than 100 to 110 mm Hg, normoventilation with PaCo2 35 to 40 mm Hg, blood glucose less than 180 mg/dl, PaO2 greater than 60 mmHg, seizure prophylaxis, etc.) treatment with 3% saline with a target serum sodium goal of 150 to 160 should be instituted if there is no contraindication. When utilizing invasive ICP monitoring, a treatment goal of less than 22 mmHg is often cited.[60][61]
Since invasive ICP monitors require some neurosurgical expertise, and traditional cutoffs of ONSD of 5 mm typically correlate to an ICP greater than 20 mmHg, ONSUS could be utilized as an aid in the decision-making process to start hypertonic therapy and as a real-time monitor of clinical effects.
A positive 30 degrees test (ONSD assessment in primary and 30 degrees from primary gaze) differentiates raised ICP due to fluid overload from that of infiltrative pathologies. [62] ‘Crescent sign’ is seen in chronic ICP compared to acute forms.[63]
Invasive methods, though considered the gold standard for ICP measurement, harbinger significant risks of infection and hemorrhage, are not readily available, and have significant financial constraints, especially in low- and middle-income nations.[64] It is a bedside, non-invasive, portable, easily performed, rapid, cheap, reproducible, efficacious, free of radiation hazards, and does not have a steep learning curve.[64][65]
Competence can be easily attained despite any formal radiology training.[65] Pocket-sized ultrasound is also now available.[66]
Limitations of the study include:
- Is operator dependent[53]
- Influence by type of settings (ER vs. ICU)[53]
- A meta-analysis has demonstrated a wide range of diagnostic odds of measurement in quantifying raised ICP[11][64]
- The optic nerve sheath is not perfectly circular and is a complex system comprising arachnoid trabeculae, pillars, and septa compartmentalizing the subarachnoid space[67]
- ONSD expansion persisted even after the normalization of raised ICP owing to the impaired retraction capability of the ONS[68]
- Alongside ICP, other factors may govern the optic nerve sheath in vivo
- Movement of the eyeball, axial length, myopia, lesions, and optic canal at the sphenoid bone can influence the ONSD[51]
Enhancing Healthcare Team Outcomes
ONSUS remains a relatively new modality for the assessment of ICP. Initial studies have shown that it is an extremely easy skill to acquire and can be performed bilaterally in less than 5 minutes by experienced operators.[14][45] Interestingly, research regarding the training of ONSUS in non-physician Special Operations Combat Medic (SOCM) trainees with minimal to no ultrasound experience has shown that after a 5-minute tutorial, trainees were able to obtain statistically non-significant measurement differences in ONSD when compared to expert physicians.[15]
Additional research has suggested that novice ultrasound users can obtain proficiency with this scan in as little as 25 exams, while an experienced sonographer might become proficient with as few as ten scans.[14] Given the safety profile of surface ultrasound and its expansion of utility in physician and non-physician training, the skill of ONSUS can be acquired and utilized by the entire health care team.[15] [Level 1]
Systematic review and meta-analysis have shown that ONSD of more than 5.00 to 5.70 mm has a concurrent ICP value above 20 mm Hg.[28][69] Systematic review and meta-analysis showed a mean ONSD in the included studies of 5.82 mm.[53]
ONSD/eyeball transverse diameter (mean value of 0.18) is more reliable than ONSD measurement alone.[11][47] This is accountable due to the following reasons:
- Significant correlation between ONSD and ETD
- Standard deviation between the normal and pathological values for ONSD is often overlapping
- The ratio is independent of demographic variables such as sex, height, weight, and BMI.[11]
ONSD reacts to ICP in real-time. Within the effective range, the chances of plastic deformation and over-distention of the ONS are minimal.[50][70] It is a very useful adjunct. to other standard diagnostic modalities.[53] However, unified methods and a range of ONSD values must be established. [64]
Consensus on the ONSD monitoring as a noninvasive surrogate marker of intracranial pressure monitoring has advocated a checklist for quality assurance pertaining to probe selection, patient safety, positioning, image acquisition, and methods of measurement.[71]
Nursing, Allied Health, and Interprofessional Team Interventions
In the right clinical setting or environment, ONSUS could provide enough information to institute neuroprotective measures or medical management in anticipation of further imaging, evacuation, or neurosurgical intervention. All healthcare team members should understand the ramifications of an elevated or increasing ONSD and familiarize themselves with ICP lowering techniques.
Nursing, Allied Health, and Interprofessional Team Monitoring
ONSUS can be taught to virtually any medical professional, even with limited ultrasound experience.[15] This may include paramedical, nursing, physician assistant, and physician providers. In many medical centers that offer neurosurgical services, there is not a neurosurgeon “in-house“ 24/7. Therefore, initial evaluation and interim monitoring will often be the responsibility of emergency medicine, intensive care, and nursing providers. There is a considerable utility in teaching this modality to any team that will commonly care for neurosurgical or critically ill patients.
Media
(Click Image to Enlarge)
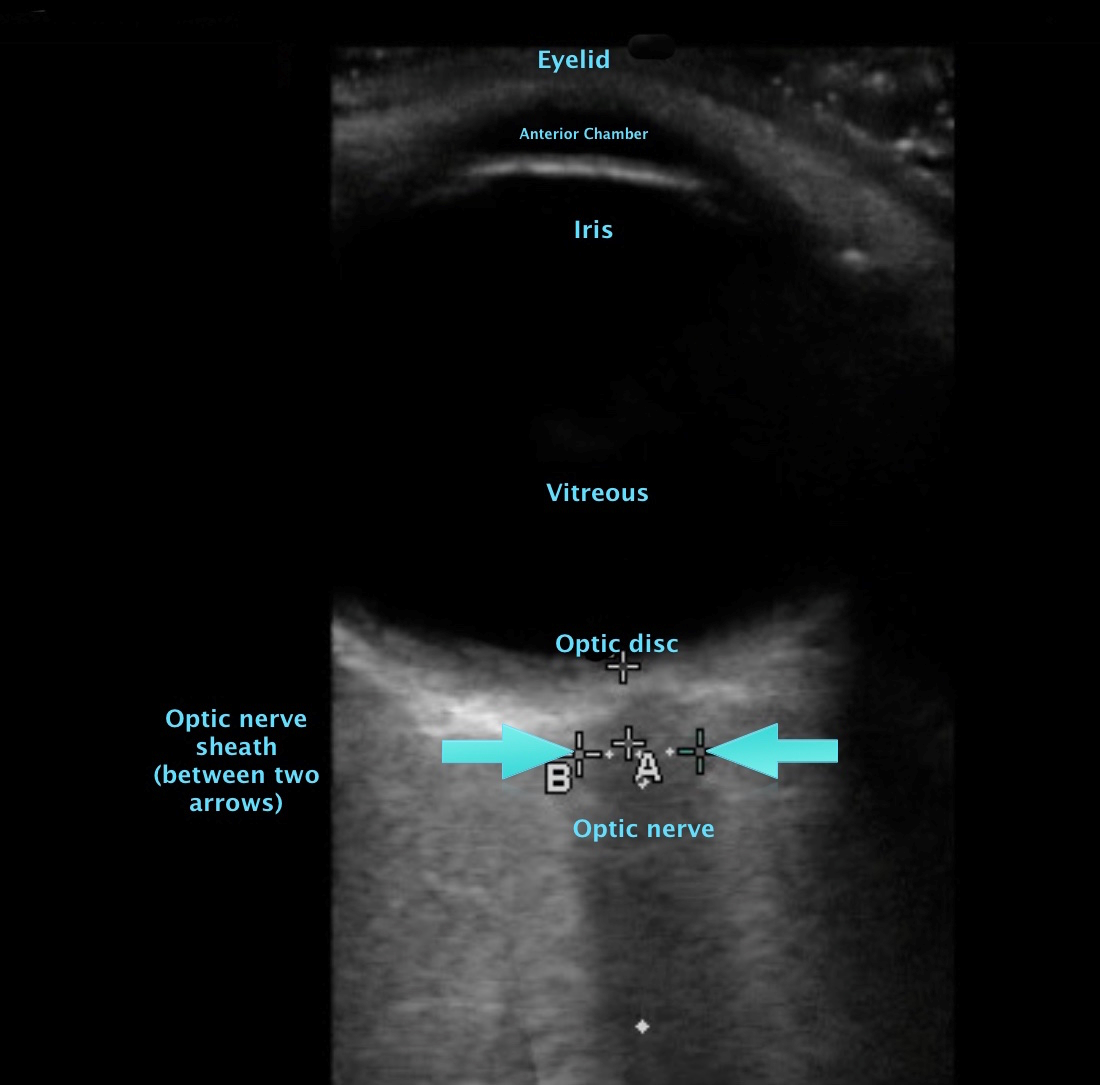
optic nerve sheath measurement Contributed by Dr. Claire Shelvin
(Click Image to Enlarge)

ultrasound in the transverse (a) and parasagittal (b) plane Contributed by Dr. Claire Shelvin
(Click Image to Enlarge)
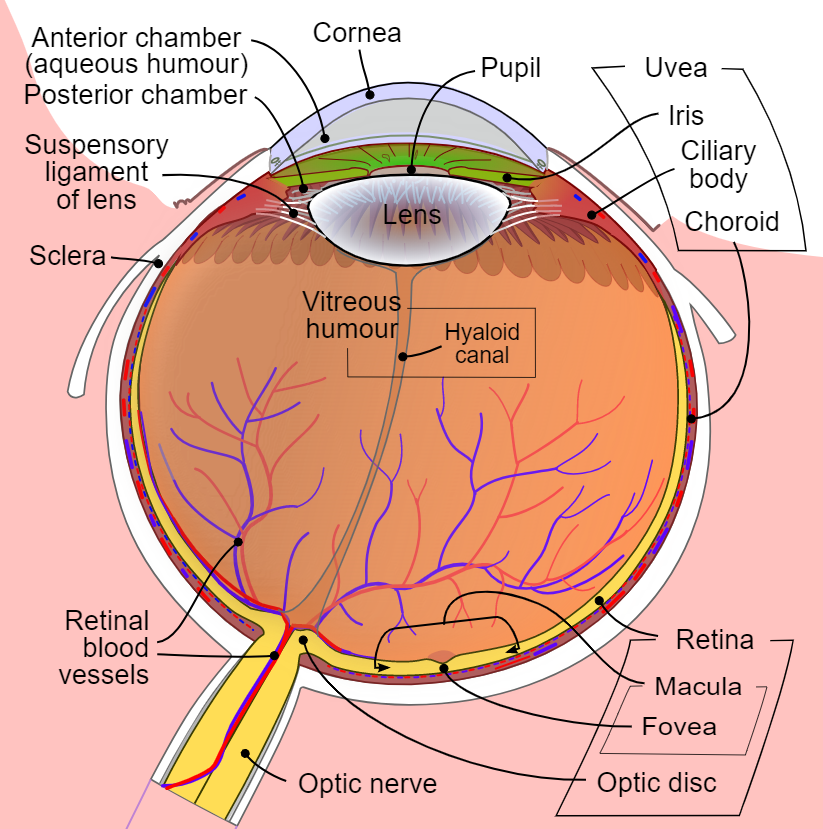
Diagram of the human eye in English. It shows the lower part of the right eye after a central and horizontal section, Ocular Anatomy Contributed by Wikimedia Users Rhcastilhos. And Jmarchn (CC BY-SA 3.0 https://creativecommons.org/licenses/by-sa/3.0/deed.en)
References
Varsou O, The Use of Ultrasound in Educational Settings: What Should We Consider When Implementing this Technique for Visualisation of Anatomical Structures? Advances in experimental medicine and biology. 2019 [PubMed PMID: 31338774]
Level 3 (low-level) evidenceAmerican College of Emergency Physicians. ACEP emergency ultrasound guidelines-2001. Annals of emergency medicine. 2001 Oct [PubMed PMID: 11574810]
Level 1 (high-level) evidenceBeal EW,Sigmond BR,Sage-Silski L,Lahey S,Nguyen V,Bahner DP, Point-of-Care Ultrasound in General Surgery Residency Training: A Proposal for Milestones in Graduate Medical Education Ultrasound. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2017 Dec [PubMed PMID: 28649711]
Mahmood F,Matyal R,Skubas N,Montealegre-Gallegos M,Swaminathan M,Denault A,Sniecinski R,Mitchell JD,Taylor M,Haskins S,Shahul S,Oren-Grinberg A,Wouters P,Shook D,Reeves ST, Perioperative Ultrasound Training in Anesthesiology: A Call to Action. Anesthesia and analgesia. 2016 Jun [PubMed PMID: 27195630]
Whitson MR,Mayo PH, Ultrasonography in the emergency department. Critical care (London, England). 2016 Aug 15 [PubMed PMID: 27523885]
Nations JA,Browning RF, Battlefield applications for handheld ultrasound. Ultrasound quarterly. 2011 Sep [PubMed PMID: 21873854]
Gharahbaghian L,Anderson KL,Lobo V,Huang RW,Poffenberger CM,Nguyen PD, Point-of-Care Ultrasound in Austere Environments: A Complete Review of Its Utilization, Pitfalls, and Technique for Common Applications in Austere Settings. Emergency medicine clinics of North America. 2017 May [PubMed PMID: 28411935]
Roque PJ,Hatch N,Barr L,Wu TS, Bedside ocular ultrasound. Critical care clinics. 2014 Apr [PubMed PMID: 24606775]
Helmke K,Hansen HC, Fundamentals of transorbital sonographic evaluation of optic nerve sheath expansion under intracranial hypertension II. Patient study. Pediatric radiology. 1996 Oct [PubMed PMID: 8805600]
Moretti R,Pizzi B, Ultrasonography of the optic nerve in neurocritically ill patients. Acta anaesthesiologica Scandinavica. 2011 Jul [PubMed PMID: 21463263]
Zhu S,Cheng C,Zhao D,Zhao Y,Liu X,Zhang J, The clinical and prognostic values of optic nerve sheath diameter and optic nerve sheath diameter/eyeball transverse diameter ratio in comatose patients with supratentorial lesions. BMC neurology. 2021 Jul 2 [PubMed PMID: 34215217]
Liu D,Kahn M, Measurement and relationship of subarachnoid pressure of the optic nerve to intracranial pressures in fresh cadavers. American journal of ophthalmology. 1993 Nov 15 [PubMed PMID: 8238213]
Hylkema C, Optic Nerve Sheath Diameter Ultrasound and the Diagnosis of Increased Intracranial Pressure. Critical care nursing clinics of North America. 2016 Mar [PubMed PMID: 26873762]
Tayal VS,Neulander M,Norton HJ,Foster T,Saunders T,Blaivas M, Emergency department sonographic measurement of optic nerve sheath diameter to detect findings of increased intracranial pressure in adult head injury patients. Annals of emergency medicine. 2007 Apr [PubMed PMID: 16997419]
Betcher J,Becker TK,Stoyanoff P,Cranford J,Theyyunni N, Military trainees can accurately measure optic nerve sheath diameter after a brief training session. Military Medical Research. 2018 Dec 20 [PubMed PMID: 30572931]
Caffery TS,Perret JN,Musso MW,Jones GN, Optic nerve sheath diameter and lumbar puncture opening pressure in nontrauma patients suspected of elevated intracranial pressure. The American journal of emergency medicine. 2014 Dec [PubMed PMID: 25284485]
Level 2 (mid-level) evidenceHassen GW,Al-Juboori M,Koppel B,Akfirat G,Kalantari H, Real time optic nerve sheath diameter measurement during lumbar puncture. The American journal of emergency medicine. 2018 Apr [PubMed PMID: 29338967]
Singleton J,Dagan A,Edlow JA,Hoffmann B, Real-time optic nerve sheath diameter reduction measured with bedside ultrasound after therapeutic lumbar puncture in a patient with idiopathic intracranial hypertension. The American journal of emergency medicine. 2015 Jun [PubMed PMID: 25595270]
Level 3 (low-level) evidenceKarmaniolou I,Petropoulos G,Theodoraki K, Management of idiopathic intracranial hypertension in parturients: anesthetic considerations. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2011 Jul [PubMed PMID: 21519980]
Level 3 (low-level) evidenceAtanassoff PG,Alon E,Weiss BM,Lauper U, Spinal anaesthesia for caesarean section in a patient with brain neoplasma. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 1994 Feb [PubMed PMID: 8131237]
Level 3 (low-level) evidenceSitanaya SN,Kamayanti F,Nugroho HA,Prabowo B, Comparing ultrasonographic optic nerve sheath diameter to head computed tomography scan to predict intracranial pressure elevation. SAGE open medicine. 2022 [PubMed PMID: 35198210]
Cannata G,Pezzato S,Esposito S,Moscatelli A, Optic Nerve Sheath Diameter Ultrasound: A Non-Invasive Approach to Evaluate Increased Intracranial Pressure in Critically Ill Pediatric Patients. Diagnostics (Basel, Switzerland). 2022 Mar 21 [PubMed PMID: 35328319]
Hanafi MG,Verki MM,Parei SN, Ultrasonic Assessment of Optic Nerve Sheath to Detect Increased Intracranial Pressure. Journal of medical ultrasound. 2019 Apr-Jun [PubMed PMID: 31316215]
Dağdelen K,Ekici M, Measuring optic nerve sheath diameter using ultrasonography in patients with idiopathic intracranial hypertension. Arquivos de neuro-psiquiatria. 2022 May 20 [PubMed PMID: 35613208]
Korsbæk JJ,Hagen SM,Schytz HW,Vukovic-Cvetkovic V,Wibroe EA,Hamann S,Jensen RH, Transorbital sonography: A non-invasive bedside screening tool for detection of pseudotumor cerebri syndrome. Cephalalgia : an international journal of headache. 2022 Apr 25 [PubMed PMID: 35469442]
Wang LJ,Zhang Y,Li C,Liu Y,Dong YN,Cui L,Xing YQ, Ultrasonographic optic nerve sheath diameter as a noninvasive marker for intracranial hypotension. Therapeutic advances in neurological disorders. 2022 [PubMed PMID: 35186123]
Level 3 (low-level) evidenceKalim Z,Siddiqui OA,Nadeem A,Hasan M,Rashid H, Assessment of Optic Nerve Sheath Diameter and Its Postoperative Regression among Patients Undergoing Brain Tumor Resection in a Tertiary Care Center. Journal of neurosciences in rural practice. 2022 Apr [PubMed PMID: 35694055]
Gauthey M,Tessaro MO,Breitbart S,Kulkarni AV,Davis AL, Reliability and feasibility of optic nerve point-of-care ultrasound in pediatric patients with ventricular shunts. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2022 Apr 20 [PubMed PMID: 35441844]
Level 2 (mid-level) evidenceŞık N,Ulusoy E,Çitlenbik H,Öztürk A,Er A,Yılmaz D,Duman M, The role of sonographic optic nerve sheath diameter measurements in pediatric head trauma. Journal of ultrasound. 2022 Apr 8 [PubMed PMID: 35396696]
Patel R,Chowdhury MAB,Gul S,Fahy BG,Gonzalez A,Fitzpatrick D,DePortu G,Weeks E,Elie-Turenne MC,Ocampo S,Ponnaluri S,Pizzi MA, Ultrasound of Optic Nerve Sheath Diameter and Stroke Outcomes. Critical care explorations. 2021 Nov [PubMed PMID: 34841250]
Oliveira BDD,Lima FO,Homem HDC,Figueirêdo AA,Freire VMB,Maia Carvalho FM, Optic Nerve Sheath Diameter Detects Intracranial Hypertension in Acute Malignant Middle Cerebral Artery Infarction. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2022 Mar [PubMed PMID: 35032755]
Xu H,Li Y,Liu J,Chen Z,Chen Q,Xiang Y,Zhang M,He W,Zhuang Y,Yang Y,Chen W,Chen Y, Dilated Optic Nerve Sheath Diameter Predicts Poor Outcome in Acute Spontaneous Intracerebral Hemorrhage. Cerebrovascular diseases (Basel, Switzerland). 2022 [PubMed PMID: 34569518]
Bates A,Goett HJ, Ocular Ultrasound . 2019 Jan [PubMed PMID: 29083793]
Kilker BA,Holst JM,Hoffmann B, Bedside ocular ultrasound in the emergency department. European journal of emergency medicine : official journal of the European Society for Emergency Medicine. 2014 Aug [PubMed PMID: 24002686]
Canakci Y,Koksal O,Durak VA, The value of bedside ocular ultrasound assessment of optic nerve sheath diameter in the detection of increased intracranial pressure in patients presenting to the emergency room with headache. Nigerian journal of clinical practice. 2018 Jun [PubMed PMID: 29888727]
Matalia J,Shirke S,Kekatpure M, An alternate technique for assessing optic nerve in papilledema by ultrasound B scan. The American journal of emergency medicine. 2015 Jul [PubMed PMID: 25921967]
Cherry PM, Rupture of the globe. Archives of ophthalmology (Chicago, Ill. : 1960). 1972 Nov [PubMed PMID: 4634787]
Chronopoulos A,Ong JM,Thumann G,Schutz JS, Occult globe rupture: diagnostic and treatment challenge. Survey of ophthalmology. 2018 Sep - Oct [PubMed PMID: 29649485]
Level 3 (low-level) evidenceEngelbert PR,Palma JK, Petroleum Jelly: A Novel Medium for Ocular Ultrasound. The Journal of emergency medicine. 2015 Aug; [PubMed PMID: 26014760]
Romagnuolo L,Tayal V,Tomaszewski C,Saunders T,Norton HJ, Optic nerve sheath diameter does not change with patient position. The American journal of emergency medicine. 2005 Sep [PubMed PMID: 16140179]
Level 2 (mid-level) evidenceKim SH,Kim HJ,Jung KT, Position does not affect the optic nerve sheath diameter during laparoscopy. Korean journal of anesthesiology. 2015 Aug [PubMed PMID: 26257848]
Verdonck P,Kalmar AF,Suy K,Geeraerts T,Vercauteren M,Mottrie A,De Wolf AM,Hendrickx JF, Optic nerve sheath diameter remains constant during robot assisted laparoscopic radical prostatectomy. PloS one. 2014 [PubMed PMID: 25369152]
You AH,Song Y,Kim DH,Suh J,Baek JW,Han DW, Effects of positive end-expiratory pressure on intraocular pressure and optic nerve sheath diameter in robot-assisted laparoscopic radical prostatectomy: A randomized, clinical trial. Medicine. 2019 Apr [PubMed PMID: 30946349]
Level 1 (high-level) evidenceChin JH,Kim WJ,Lee J,Han YA,Lim J,Hwang JH,Cho SS,Kim YK, Effect of Positive End-Expiratory Pressure on the Sonographic Optic Nerve Sheath Diameter as a Surrogate for Intracranial Pressure during Robot-Assisted Laparoscopic Prostatectomy: A Randomized Controlled Trial. PloS one. 2017 [PubMed PMID: 28107408]
Level 1 (high-level) evidenceOhle R,McIsaac SM,Woo MY,Perry JJ, Sonography of the Optic Nerve Sheath Diameter for Detection of Raised Intracranial Pressure Compared to Computed Tomography: A Systematic Review and Meta-analysis. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2015 Jul [PubMed PMID: 26112632]
Level 1 (high-level) evidenceDe Bernardo M,Vitiello L,De Pascale I,Capasso L,Cornetta P,Rosa N, Optic Nerve Ultrasound Evaluation in Idiopathic Intracranial Hypertension. Frontiers in medicine. 2022 [PubMed PMID: 35299843]
Kim DH,Jun JS,Kim R, Ultrasonographic measurement of the optic nerve sheath diameter and its association with eyeball transverse diameter in 585 healthy volunteers. Scientific reports. 2017 Nov 21 [PubMed PMID: 29162911]
Robba C,Santori G,Czosnyka M,Corradi F,Bragazzi N,Padayachy L,Taccone FS,Citerio G, Optic nerve sheath diameter measured sonographically as non-invasive estimator of intracranial pressure: a systematic review and meta-analysis. Intensive care medicine. 2018 Aug [PubMed PMID: 30019201]
Level 1 (high-level) evidenceKim DH,Jun JS,Kim R, Measurement of the Optic Nerve Sheath Diameter with Magnetic Resonance Imaging and Its Association with Eyeball Diameter in Healthy Adults. Journal of clinical neurology (Seoul, Korea). 2018 Jul [PubMed PMID: 29856162]
Wang LJ,Chen LM,Chen Y,Bao LY,Zheng NN,Wang YZ,Xing YQ, Ultrasonography Assessments of Optic Nerve Sheath Diameter as a Noninvasive and Dynamic Method of Detecting Changes in Intracranial Pressure. JAMA ophthalmology. 2018 Mar 1 [PubMed PMID: 29392301]
Vaiman M,Gottlieb P,Bekerman I, Quantitative relations between the eyeball, the optic nerve, and the optic canal important for intracranial pressure monitoring. Head & face medicine. 2014 Aug 17 [PubMed PMID: 25130267]
Petrou S,Raio C,Klein L,Felicetta M, Posterior Globe Depth for Optic Nerve Sheath Diameter Measurement in Ocular Ultrasound in Healthy Volunteers. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2021 Dec 19 [PubMed PMID: 34927283]
Montorfano L,Yu Q,Bordes SJ,Sivanushanthan S,Rosenthal RJ,Montorfano M, Mean value of B-mode optic nerve sheath diameter as an indicator of increased intracranial pressure: a systematic review and meta-analysis. The ultrasound journal. 2021 Jul 2 [PubMed PMID: 34215966]
Level 1 (high-level) evidenceCopetti R,Cattarossi L, Optic nerve ultrasound: artifacts and real images. Intensive care medicine. 2009 Aug [PubMed PMID: 19367390]
Level 3 (low-level) evidenceBeckmann U,Gillies DM,Berenholtz SM,Wu AW,Pronovost P, Incidents relating to the intra-hospital transfer of critically ill patients. An analysis of the reports submitted to the Australian Incident Monitoring Study in Intensive Care. Intensive care medicine. 2004 Aug [PubMed PMID: 14991102]
Level 2 (mid-level) evidenceAliaga M,Forel JM,De Bourmont S,Jung B,Thomas G,Mahul M,Bisbal M,Nougaret S,Hraiech S,Roch A,Chaumoitre K,Jaber S,Gainnier M,Papazian L, Diagnostic yield and safety of CT scans in ICU. Intensive care medicine. 2015 Mar [PubMed PMID: 25518950]
Level 2 (mid-level) evidenceCaruana M,Culp K, Intrahospital transport of the critically ill adult: a research review and implications. Dimensions of critical care nursing : DCCN. 1998 May-Jun [PubMed PMID: 9633345]
Indeck M,Peterson S,Smith J,Brotman S, Risk, cost, and benefit of transporting ICU patients for special studies. The Journal of trauma. 1988 Jul [PubMed PMID: 3135417]
Lazarus R,Helmick K,Malik S,Gregory E,Agimi Y,Marion D, Continuum of the United States military's traumatic brain injury care: adjusting to the changing battlefield. Neurosurgical focus. 2018 Dec 1 [PubMed PMID: 30544329]
Bratton SL,Chestnut RM,Ghajar J,McConnell Hammond FF,Harris OA,Hartl R,Manley GT,Nemecek A,Newell DW,Rosenthal G,Schouten J,Shutter L,Timmons SD,Ullman JS,Videtta W,Wilberger JE,Wright DW, Guidelines for the management of severe traumatic brain injury. IX. Cerebral perfusion thresholds. Journal of neurotrauma. 2007 [PubMed PMID: 17511547]
Carney N,Totten AM,O'Reilly C,Ullman JS,Hawryluk GW,Bell MJ,Bratton SL,Chesnut R,Harris OA,Kissoon N,Rubiano AM,Shutter L,Tasker RC,Vavilala MS,Wilberger J,Wright DW,Ghajar J, Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery. 2017 Jan 1 [PubMed PMID: 27654000]
Caffery TS,Musso MW, Questions regarding the utility of the 30-degree test in measuring optic nerve sheath diameters in ED patients. The American journal of emergency medicine. 2015 Apr [PubMed PMID: 25744151]
Level 3 (low-level) evidenceBhosale A,Shah VM,Shah PK, Accuracy of crescent sign on ocular ultrasound in diagnosing papilledema. World journal of methodology. 2017 Sep 26 [PubMed PMID: 29026691]
Bittencourt Rynkowski C,Caldas J, Ten Good Reasons to Practice Neuroultrasound in Critical Care Setting. Frontiers in neurology. 2021 [PubMed PMID: 35095741]
Dinsmore M,Venkatraghavan L, Clinical applications of point-of-care ultrasound in brain injury: a narrative review. Anaesthesia. 2022 Jan [PubMed PMID: 35001377]
Level 3 (low-level) evidenceJohnson GGRJ,Jelic T,Derksen A,Unger B,Zeiler FA,Ziesmann MT,Gillman LM, Accuracy of Optic Nerve Sheath Diameter Measurements in Pocket-Sized Ultrasound Devices in a Simulation Model. Frontiers in medicine. 2022 [PubMed PMID: 35308521]
Killer HE, Laeng HR, Flammer J, Groscurth P. Architecture of arachnoid trabeculae, pillars, and septa in the subarachnoid space of the human optic nerve: anatomy and clinical considerations. The British journal of ophthalmology. 2003 Jun:87(6):777-81 [PubMed PMID: 12770980]
Wu GB,Tian J,Liu XB,Wang ZY,Guo JY, Can optic nerve sheath diameter assessment be used as a non-invasive tool to dynamically monitor intracranial pressure? Journal of integrative neuroscience. 2022 Mar 22 [PubMed PMID: 35364642]
Dubourg J,Javouhey E,Geeraerts T,Messerer M,Kassai B, Ultrasonography of optic nerve sheath diameter for detection of raised intracranial pressure: a systematic review and meta-analysis. Intensive care medicine. 2011 Jul [PubMed PMID: 21505900]
Level 1 (high-level) evidenceChen LM,Wang LJ,Hu Y,Jiang XH,Wang YZ,Xing YQ, Ultrasonic measurement of optic nerve sheath diameter: a non-invasive surrogate approach for dynamic, real-time evaluation of intracranial pressure. The British journal of ophthalmology. 2019 Apr [PubMed PMID: 30361274]
Hirzallah MI,Lochner P,Hafeez MU,Lee AG,Krogias C,Dongarwar D,Manchanda R,Ouellette L,Hartman ND,Ertl M,Schlachetzki F,Robba C, Quality assessment of optic nerve sheath diameter ultrasonography: Scoping literature review and Delphi protocol. Journal of neuroimaging : official journal of the American Society of Neuroimaging. 2022 Jun 16 [PubMed PMID: 35711135]
Level 2 (mid-level) evidence