
Introduction
The tracheal bronchus is a rare congenital anomaly described as a collection of bronchial variations arising from the trachea directed towards the upper lung lobe. Usually, they arise within 2 cm of the carina but can arise anywhere from the cricoid cartilage to the carina. Some authors opine that if this abnormal bronchus supplies the entire upper lung lobe, then it is called bronchus suis or pig bronchus.[1][2] This category does not include bronchi originating from the main bronchus.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
There are three embryological theories mechanism tracheal bronchus formation.
- The reduction theory suggests it results from the reduction of a previously developed bronchus.
- The migration theory explains it to be the extension or migration of a part of the developed hyparterial branching pattern to a different location either on the trachea or bronchus.
- The selection theory postulates that local morphogenesis disturbances cause bronchial abnormalities, claiming that bronchus can arise if the bronchial mesenchyme comes in contact with the tracheal epithelium.[3]
Epidemiology
In multiple studies done on the pediatric population, tracheal bronchus is present in 0.9 to 3% of the population studied, with the majority of the cases arising from the right lateral wall. The prevalence of right-sided is up to 0.1 to 2%, and on the left side is reported to be 0.3 to 1%.[1] It has been found to been associated with other congenital abnormalities such as Down syndrome, VATER (vertebrae, anus, trachea, esophagus, renal), tracheoesophageal fistula, esophageal atresia, laryngeal and duodenal webs, spinal fusion defects, cardiac congenital defects, and hypoplastic lung. In the pediatric population, tracheal bronchus detected by flexible bronchoscopy had an incidence of 1.9% at a median age of 15 months (age range 1 month to 13 years), with no gender differences. There are reports associated with congenital pathologies reported in 92.3% cases with heart disease accounting for 69%, chromosomal abnormality 35%, and spinal fusion defect 11%.[4][5]
Pathophysiology
Any obstruction of the tracheal bronchus can lead to atelectasis, decrease ventilation, and infection. Hence in children, recurrent upper lobe pneumonia is a common presentation. These complications usually occur when the clinician does not diagnose the tracheal bronchus.[4] Patients frequently present with wheezing and hypoxia due to the narrowing of the aberrant bronchus and may be mistaken for asthma. Abnormal ventilation mechanics may contribute to patient symptoms [6]. There have been cases reporting tracheal bronchus associated with TB, leiomyoma, cancers, and as a source of bleeding leading to death. There is a lack of sufficient evidence of any association between a tracheal bronchus and its predisposition to any malignancy.[7][8][9][10]
One classification categorizes the tracheal bronchus about the carina anatomically:
- Type I is when the tracheal bronchus is more than 2 cm from the carina, and there is a narrowing of the distal trachea
- Type II is when the tracheal bronchus is more than 2 cm from the carina, but there is no narrowing of the distal trachea
- Type III is when the tracheal bronchus is less than 2 cm above the level of the carina
An additional classification system describes tracheal bronchi relative to the upper lobe bronchus and pulmonary arteries.
- A normal right upper lobe bronchus is termed eparterial as it arises cranial to the right pulmonary artery.
- A normal left upper lobe bronchus is called hyparterial as it arises caudal to the normal left pulmonary artery.
- An aberrant bronchus arising proximal to the upper lobe bronchus is called pre-eparterial on the right side and eparterial or pre-hyparterial on the left side.
- A bronchus arising distal to the upper lobe bronchus is called post eparterial on the right side and post hyparterial on the left side.[2][3]
Tracheal bronchus may be displaced or supernumerary.
- If the anatomic upper-lobe bronchus is missing a single branch, the tracheal bronchus is defined as displaced.
- If the right upper-lobe bronchus has a normal trifurcation into apical, posterior, and anterior segmental bronchi, the tracheal bronchus is defined as supernumerary.
The supernumerary bronchi may end blindly; in that case, they are also called tracheal diverticula. If they terminate in aerated or bronchiectasis lung tissue, the term for this is apical accessory lungs or tracheal lobes.[11]
Incidental intubation of tracheal bronchus can cause obstruction, pneumothorax, post obstructive pneumonia, and respiratory failure.[12]
History and Physical
Children may remain asymptomatic, however, most manifest early in the form of wheezing, stridor, refractory cough, pneumonia, atelectasis.[5] A tracheal bronchus may also be identified in adults, who are more often asymptomatic allowing for manifestation later in adulthood. Tracheal bronchus should be on the list of differentials in cases of persistent upper lobe pneumonia, atelectasis or air trapping, and chronic bronchitis. It can present with chronic symptoms of productive cough over multiple years and be treated multiple times for recurrent pneumonia with CT findings of bronchiectasis. In cases where tracheal bronchus is found incidentally e.g during intubation and in the perioperative setting, special attention should be paid. Extra care should be taken while intubating patients with tracheal bronchus as the tube can potentially obstruct or even migrate into the bronchus itself, thus resulting in atelectasis, hypoxemia, or both.
Fortunately, the malposition of the ETT is rare because most cases arise from the right side of the trachea approximately within 2 cm from the carina but still need to be considered in all patients with a tracheal bronchus. As tracheal bronchus can arise at any point from the trachea, there is no standard safe distance point from the incisor mark to prevent its obstruction either by insufflation of the cuff or by endotracheal tube entrance itself. Hence follow-up chest x-ray is of paramount importance in such cases.[4] One lung ventilation can be complicated by the presence of a tracheal bronchus. In such cases based on where the lesion site is located, certain measures can help anesthesiologists. Flexible bronchoscopy should be done before to find the location of the tracheal bronchus and its distance from the carina. Then either a double-lumen tube or uninvent tube with a bronchial blocker or a regular tracheal tube with the bronchial blocker is used. A double lumen tube can be left-sided or right-sided. Both the tubes are slightly different.
Based on normal anatomy left main bronchus is longer and divide into upper and lower secondary bronchus. While right main bronchus is much smaller and divides into apical, anterior, and posterior secondary bronchi. The left-sided double-lumen tube is preferred in most cases. The right-sided tube is used in selective cases where the right lung needs to be isolated. In right-sided tracheal bronchus, a right-sided tube is contraindicated given it can easily block the tracheal bronchus from its tracheal cuff. Based on the location of tracheal bronchus and its origin, one-lung ventilation for procedures such as thoracotomy, lobectomy, segmentectomy can be achieved either by the opposite side double-lumen tube. The position of the endobronchial tube should be confirmed with flexible tracheobronchoscopy. Lung isolation is achieved by either clamping the tracheal tube or endobronchial tube depending on which side the procedure is performed.
Similarly uninvent tube can be used, which has 2 lumens within a single tube and has a tracheal and endobronchial cuff of in-build bronchial blocker. Another technique employed is the use of bronchial blockers for the tracheal bronchus and a regular endotracheal tube for the rest of the lung.
Some reports preferred left-sided double-lumen tube overuse of bronchial blockers for tracheal bronchus.[13] Cases have reported the use of a Fogarty catheter along with the uninvent tube to be effective in providing successful lung isolation in the presence of tracheal bronchus. Other potential solutions include the use of a Fogarty catheter in the tracheal bronchus with a bronchial blocker located in the right main bronchus.[14]
Evaluation
Chest X-ray and CT chest occasionally can show tracheal bronchus. However, most cases are incidental findings on bronchoscopy. Multi-detector CT (MDCT) with 3D image reconstruction is the gold-standard test in detecting congenital tracheobronchial anomalies. MDCT allows the making of a direct diagnosis of tracheal bronchus non-invasively. Faster acquisition time, increased anatomic coverage, and decreased sedation requirement in comparison to bronchoscopy make 3D reconstruction imaging an ideal modality for detecting tracheobronchial anomalies. Also, 3D-CT is a powerful tool in diagnosing the relationship between tracheal and arterial tree, which would be ideal if the patient were to undergo surgical intervention. Reconstruction images have overcome the limitations of axial CT images, which included failure to identify subtle tracheal stenosis, a craniocaudal extension of the airway disease, and disease limited to airways obliquely located to axial planes. Findings seen on imaging in symptomatic patients include bronchiectasis, focal emphysema, and focal cystic malformations.[15][16][17]
A retrospective cross-sectional analysis on 20 individuals of different tracheobronchial anomalies (stenosis, tracheomalacia, tracheal bronchus, agenesis) compared the diagnostic benefit of MRI, MDCT, and 3D with confirmation by bronchoscopy or surgery. The study found that MDCT was superior to MRI in diagnosing anomalies. In 12 patients who underwent both MDCT and 3D, researchers determined that 3D added specific information in seven cases; in three cases, it played a crucial role in attempting surgical interventions, while in another four cases, it added specific information regarding surgical planning.[18]
FDG PET scan has a limited role in differentiating inflammatory versus malignant lesion of the tracheal bronchus; hence, after definitive surgery, specimens are sent for histopathologic evaluation.[19]
Treatment / Management
Currently, the mainstay of the treatment of tracheal bronchus is symptomatic management. Asymptomatic cases require only observation, whereas symptomatic tracheal bronchus is treated based on the severity of symptoms. Given the broad range of symptoms that tracheal bronchus can present, medical management includes bronchodilators, inhaled corticosteroids, muscarinic antagonists, and antibiotics. However, if the symptoms are refractory to medication, then surgical treatment is the next step in management. Segmentectomy and lobectomy have been performed for the treatment of recurrent pneumonia resulting from the tracheal bronchus and have shown to be curative.
One lung ventilation with the use of bronchial blocker in cases of unilateral thoracotomy or use of a double-lumen endotracheal tube is an option for intubation in these patients. Use of small caliber tubes, keeping the endotracheal tube high above the carina level by withdrawing it a little, and confirmation via fiber optic bronchoscope to double-check that there is no tracheal bronchus obstruction is done by anesthetics.[20][21](B3)
Differential Diagnosis
- Pneumonia
- Tracheal stenosis
- Tracheomalacia
- Bronchomalacia
- Congenital heart, esophageal, laryngeal abnormalities and syndromes (Down syndrome, VACTERAL, i.e., vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies, and limb abnormalities)
- Accessory or supernumerary bronchus
- Asthma
Prognosis
Based on treatment, tracheal bronchus has good outcomes. There are no numerical figures available to compare the outcomes of a patient who underwent surgical treatment for tracheal bronchus. However, there was a case series of children that reported positive outcomes at 2 to 10 years, which was strictly observational. A pediatric case who underwent right upper lobectomy ended up on tracheostomy with a resultant decrease in frequency.[22] Another case report reported an uneventful outcome at 12 months after upper lobe lobectomy via thoracoscopy in a 1-year-old patient.
Only two cases of thoracoscopic upper lobe lobectomy/segmentectomy in adults have appeared in the literature for tracheal bronchus performed with the uneventful course.[23][24]
Complications
- Recurrent pneumonia
- Atelectasis
- Acute respiratory failure
- Aspiration pneumonia if there is communication with the esophagus
- Congestive heart failure if coexisting congenital heart anomaly
Deterrence and Patient Education
A literature review does not reveal any underlying genetic factors that predispose more towards developing tracheobronchial anomalies. Preventive strategies still require outlining after determining the genetic predisposition to this congenital anomaly.
Pearls and Other Issues
The tracheal bronchus is often overlooked in patients presenting with recurrent lung infections.
Familiarization with the different anatomic variants of the tracheobronchial tree play a critical role in outpatient as well during intraoperative settings.
Enhancing Healthcare Team Outcomes
Congenital tracheobronchial anomalies such as tracheal bronchus should be a consideration in patients who present with recurrent respiratory infections, but they may also present as nonspecific pulmonary symptoms or may be asymptomatic altogether. Initial treatment should be focused on managing symptoms medically but may eventually require surgical intervention. MDCT with 3D is the most helpful diagnostic study in exploring the relationship between the tracheobronchial anomalies and surrounding vascular structures. Patients with tracheal bronchus should be handled with extra care during intubation as malposition may cause atelectasis, leading to hypoxia.
Managing tracheal bronchus requires an interprofessional healthcare team. The patient's primary care physician and pulmonologist should be well aware of tracheal bronchus and its relation to different syndromes. The anesthesiologist should be made aware of tracheal bronchus and be able to troubleshoot and diagnose a problem if the need arises. Nursing staff can assist during any procedure, counsel on medical management, and monitor symptoms and note patient compliance with any treatment, as well as assessing the effectiveness of the treatment. The pharmacist should have involvement with the medical management of the condition, ensuring that there are no contraindications, drug interactions and that dosing is age-appropriate. This interprofessional team paradigm, with open communication between disciples, helps ensure the best possible patient outcomes. [Level 5]
Media
(Click Image to Enlarge)
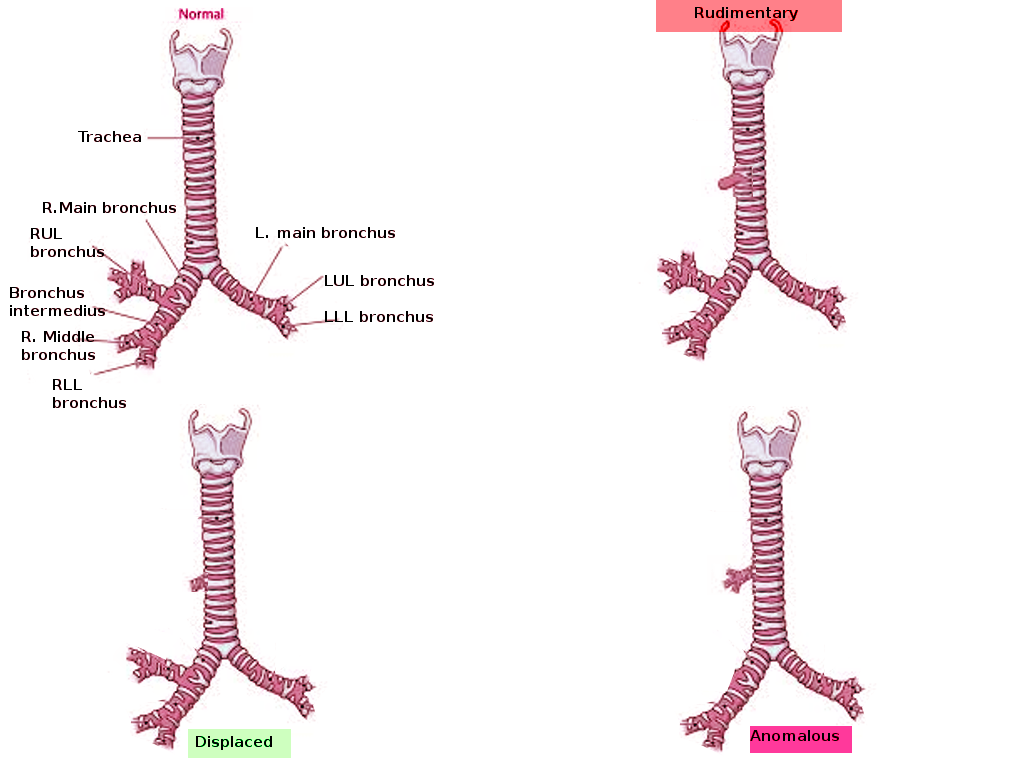
Types of tracheal bronchus Image courtesy S Bhimji MD
(Click Image to Enlarge)
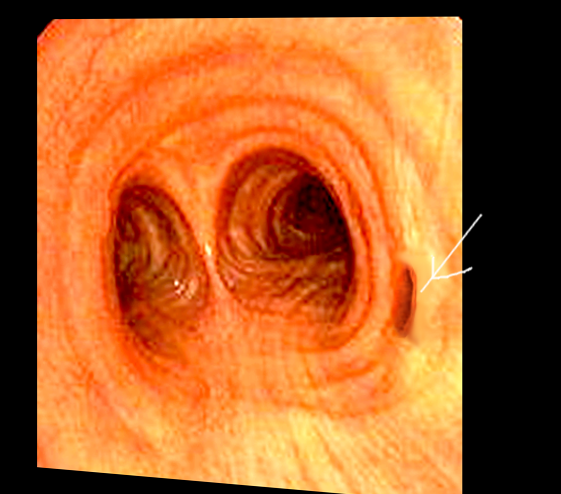
Tracheal bronchus-bronschoscopy Image courtesy S Bhimji MD
References
Lawrence DA, Branson B, Oliva I, Rubinowitz A. The wonderful world of the windpipe: a review of central airway anatomy and pathology. Canadian Association of Radiologists journal = Journal l'Association canadienne des radiologistes. 2015 Feb:66(1):30-43. doi: 10.1016/j.carj.2014.08.003. Epub [PubMed PMID: 25623009]
Chassagnon G, Morel B, Carpentier E, Ducou Le Pointe H, Sirinelli D. Tracheobronchial Branching Abnormalities: Lobe-based Classification Scheme. Radiographics : a review publication of the Radiological Society of North America, Inc. 2016 Mar-Apr:36(2):358-73. doi: 10.1148/rg.2016150115. Epub 2016 Feb 1 [PubMed PMID: 26824513]
Setty SP, Michaels AJ. Tracheal bronchus: case presentation, literature review, and discussion. The Journal of trauma. 2000 Nov:49(5):943-5 [PubMed PMID: 11086789]
Level 3 (low-level) evidencePérez Ruiz E, Caro Aguilera P, Valdivielso AI, Sanchís Cárdenas S, Martínez García Y, Pérez Frías J. Tracheal bronchus diagnosed in children undergoing flexible bronchoscopy. Paediatric respiratory reviews. 2018 Sep:28():26-30. doi: 10.1016/j.prrv.2018.03.009. Epub 2018 May 19 [PubMed PMID: 29914745]
Ghaye B, Szapiro D, Fanchamps JM, Dondelinger RF. Congenital bronchial abnormalities revisited. Radiographics : a review publication of the Radiological Society of North America, Inc. 2001 Jan-Feb:21(1):105-19 [PubMed PMID: 11158647]
Qi S, Zhang B, Yue Y, Shen J, Teng Y, Qian W, Wu J. Airflow in Tracheobronchial Tree of Subjects with Tracheal Bronchus Simulated Using CT Image Based Models and CFD Method. Journal of medical systems. 2018 Mar 1:42(4):65. doi: 10.1007/s10916-017-0879-0. Epub 2018 Mar 1 [PubMed PMID: 29497841]
Level 2 (mid-level) evidenceTuon FF, Siqueira AM, Litvoc MN, Lopes MH. Tuberculosis and tracheal bronchus. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2007 Sep:11(5):467-8 [PubMed PMID: 17331782]
Level 3 (low-level) evidenceTamura M, Murata T, Kurumaya H, Ohta Y. Leiomyoma of an accessory tracheal bronchus. The Annals of thoracic surgery. 2004 Dec:78(6):2163-5 [PubMed PMID: 15561062]
Level 3 (low-level) evidenceNicolaou N, Du Plessis A. Squamous carcinoma arising from a true tracheal bronchus: Management and case report. International journal of surgery case reports. 2015:6C():256-8. doi: 10.1016/j.ijscr.2014.12.005. Epub 2014 Dec 19 [PubMed PMID: 25549955]
Level 3 (low-level) evidenceIsmail M, Vukasinov P, Liao HI, Mir P. Hemoptysis in a previously healthy elderly patient with an unrecognized tracheal bronchus: A case report. Respiratory medicine case reports. 2017:22():34-35. doi: 10.1016/j.rmcr.2017.06.002. Epub 2017 Jun 2 [PubMed PMID: 28649488]
Level 3 (low-level) evidenceBerrocal T, Madrid C, Novo S, Gutiérrez J, Arjonilla A, Gómez-León N. Congenital anomalies of the tracheobronchial tree, lung, and mediastinum: embryology, radiology, and pathology. Radiographics : a review publication of the Radiological Society of North America, Inc. 2004 Jan-Feb:24(1):e17 [PubMed PMID: 14610245]
Lai KM, Hsieh MH, Lam F, Chen CY, Chen TL, Chang CC. Anesthesia for patients with tracheal bronchus. Asian journal of anesthesiology. 2017 Dec:55(4):87-88. doi: 10.1016/j.aja.2017.09.002. Epub 2017 Oct 26 [PubMed PMID: 29122588]
Lee HL, Ho AC, Cheng RK, Shyr MH. Successful one-lung ventilation in a patient with aberrant tracheal bronchus. Anesthesia and analgesia. 2002 Aug:95(2):492-3, table of contents [PubMed PMID: 12145079]
Level 3 (low-level) evidenceLee DK, Kim YM, Kim HZ, Lim SH. Right upper lobe tracheal bronchus: anesthetic challenge in one-lung ventilated patients -A report of three cases-. Korean journal of anesthesiology. 2013 May:64(5):448-50. doi: 10.4097/kjae.2013.64.5.448. Epub 2013 May 24 [PubMed PMID: 23741569]
Level 3 (low-level) evidenceBaden W, Schaefer J, Kumpf M, Tzaribachev N, Pantalitschka T, Koitschev A, Ziemer G, Fuchs J, Hofbeck M. Comparison of imaging techniques in the diagnosis of bridging bronchus. The European respiratory journal. 2008 May:31(5):1125-31. doi: 10.1183/09031936.00045907. Epub [PubMed PMID: 18448507]
Level 3 (low-level) evidenceSuzuki M, Matsui O, Kawashima H, Takemura A, Matsubara K, Hayashi N, Koda W, Shibata Y. Radioanatomical study of a true tracheal bronchus using multidetector computed tomography. Japanese journal of radiology. 2010 Apr:28(3):188-92. doi: 10.1007/s11604-009-0405-5. Epub 2010 May 1 [PubMed PMID: 20437128]
Jugpal TS, Garg A, Sethi GR, Daga MK, Kumar J. Multi-detector computed tomography imaging of large airway pathology: A pictorial review. World journal of radiology. 2015 Dec 28:7(12):459-74. doi: 10.4329/wjr.v7.i12.459. Epub [PubMed PMID: 26753061]
Laroia AT, Thompson BH, Laroia ST, van Beek E Jr. Modern imaging of the tracheo-bronchial tree. World journal of radiology. 2010 Jul 28:2(7):237-48. doi: 10.4329/wjr.v2.i7.237. Epub [PubMed PMID: 21160663]
Schweigert M, Dubecz A, Ofner D, Stein HJ. Tracheal bronchus associated with recurrent pneumonia. The Ulster medical journal. 2013 May:82(2):94-6 [PubMed PMID: 24082287]
Level 3 (low-level) evidenceMoon YJ, Kim SH, Park SW, Lee YM. The implications of a tracheal bronchus on one-lung ventilation and fibreoptic bronchoscopy in a patient undergoing thoracic surgery: a case report. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2015 Apr:62(4):399-402. doi: 10.1007/s12630-014-0293-8. Epub 2014 Dec 16 [PubMed PMID: 25510236]
Level 3 (low-level) evidenceConacher ID. Implications of a tracheal bronchus for adult anaesthetic practice. British journal of anaesthesia. 2000 Aug:85(2):317-20 [PubMed PMID: 10992847]
Level 3 (low-level) evidenceRahmanian R, Zheng J, Chadha NK, Kozak FK, Campbell AI, Ludemann JP. False carina: a distinct variant of tracheal bronchus. International journal of pediatric otorhinolaryngology. 2015 Apr:79(4):623-8. doi: 10.1016/j.ijporl.2015.01.023. Epub 2015 Jan 25 [PubMed PMID: 25683591]
Level 3 (low-level) evidenceXu XF, Chen L, Wu WB, Zhu Q. Thoracoscopic right posterior segmentectomy of a patient with anomalous bronchus and pulmonary vein. The Annals of thoracic surgery. 2014 Dec:98(6):e127-9. doi: 10.1016/j.athoracsur.2014.09.059. Epub 2014 Dec 1 [PubMed PMID: 25468123]
Level 3 (low-level) evidenceYurugi Y, Nakamura H, Taniguchi Y, Miwa K, Fujioka S, Haruki T, Takagi Y, Matsuoka Y, Kubouchi Y. Case of thoracoscopic right upper lobectomy for lung cancer with tracheal bronchus and a pulmonary vein variation. Asian journal of endoscopic surgery. 2012 May:5(2):93-5. doi: 10.1111/j.1758-5910.2011.00115.x. Epub [PubMed PMID: 22776372]
Level 3 (low-level) evidenceShih FC, Lee WJ, Lin HJ. Tracheal bronchus. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2009 Mar 31:180(7):783. doi: 10.1503/cmaj.080280. Epub [PubMed PMID: 19332762]
Rasooly AJ, Noor S, Ullah S, Baryali AT, Haidary AM. Forty days old infant with Pig Bronchus, presenting with recurrent pneumonia: A Case Report. Pediatric health, medicine and therapeutics. 2023:14():379-383. doi: 10.2147/PHMT.S429852. Epub 2023 Oct 30 [PubMed PMID: 37927398]
Level 3 (low-level) evidence