Introduction
Graves orbitopathy (Graves eye disease or Graves ophthalmopathy) is a constellation of signs and symptoms related to the orbit and surrounding tissues in patients with Graves disease. It can also sporadically occur in patients who are euthyroid or even hypothyroid as a result of chronic thyroiditis.[1] It is an autoimmune process affecting retro-ocular tissues.[1] In its severe form, it can be sight-threatening; thus, prompt evaluation and timely referral and management become of utmost importance.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The culprit antibody in Graves’ disease is the thyroid-stimulating hormone (TSH) receptor antibody. Its main site of action is on TSH receptors in the thyroid. However, TSH receptors are present in various extrathyroidal tissues. Evidence has suggested that the expression of the TSH receptor is in higher concentration in retro-ocular tissue in patients with Graves disease.[2]
Of note, research has implicated several risk factors, which increase the predisposition of patients with Graves’ disease to develop orbitopathy. In general, higher titers of TSH receptor antibodies link to increased extra-thyroidal manifestations of Graves disease, including Graves eye disease. Other risk factors include female gender, certain genetic factors (however, specific genes or mutations remain unidentified in having a direct causal relationship), and exposure to radioiodine as a treatment modality for Graves disease.[3] Smoking is the most significant modifiable risk factor. Graves eye disease tends to be more severe and less responsive to immunomodulatory therapy in those patients who smoke. The mechanism of how smoking is related to Graves eye disease is postulated to be by it affecting both humoral and cell-mediated immunity and suppression of natural killer T cells.[1]
Several cell types play a role in the pathogenesis of Graves orbitopathy. Fibroblasts are stimulated by TSH receptor antibodies as well as by T-cells (mediated by cytokine production) to initiate two pathways.[4] The first is to produce glycosaminoglycans (GAGs), the most pertinent of which is hyaluronic acid. The accumulation of these hydrophilic molecules leads to extraocular muscle swelling. The second pathway is through adipogenesis. Thus the combination of muscle swelling resulting in increased extraocular muscle volume with excess retro-ocular fat results in proptosis and the other clinical manifestations of Graves orbitopathy.
There is also a postulate that IGF-1 receptors, which are present in fibroblasts, when stimulated via TSH receptor antibodies, also synergistically stimulate GAG production.
Upper eyelid retraction occurs as a result of inflammation and fibrosis of Müller's muscle or a phenomenon called pseudo-lid retraction. This situation occurs when there is restriction of the inferior rectus muscle and thus resultant overactivity of the levator palpebrae complex.[5] In general, the most commonly affected extra-ocular muscles are the inferior rectus and medial rectus muscles.
Epidemiology
Graves’ orbitopathy has been said to occur in as many as 25 to 50% of patients diagnosed with Graves' disease. One study reported that the incidence of clinically apparent Graves orbitopathy was 16 per 100000 in females and 2.9 per 100000 in males. It is, however, also important to realize that an even larger proportion of patients may have MRI evidence of Graves orbitopathy in the absence of clinical disease.[6][7][8]
History and Physical
History and physical examination are paramount to assess Graves orbitopathy.[9] In patient history, it is necessary to elicit if the patient is experiencing any symptoms. Not all those with proptosis will be symptomatic. Symptoms that may be present include a foreign-body sensation in the eyes with resultant tearing, pain or pressure in or behind the eye, and pain on moving the eye in any direction. Visual alterations may also be present in the form of diplopia, blurring, desaturation of color vision, or rarely complete loss of vision. Some patients may notice swelling around their eyes or redness, and others may report that they are unable to close their eyes completely.
On physical examination, the first step is to inspect the eyes for proptosis and comment on whether it is symmetrical or asymmetrical and, if an exophthalmometer should make available, objective measures of the degree of proptosis. Also, evaluate for conjunctival injection, chemosis, and periorbital edema. Upper eyelid retraction (although not specific to Graves orbitopathy) is often present. After inspecting the eyes, then determine if the patient can fully close their eyes; this is very important as it may identify those at risk for corneal damage through exposure keratopathy. Next, test the extraocular muscles by asking the patient to look in all directions. This test will help elicit if the patient is experiencing pain in a particular direction of gaze or can fully move the eye in a specific direction, which will subsequently reveal any potential entrapment of an extraocular muscle. Lastly, testing both visual acuity and color vision should be included as part of the comprehensive examination.
There is a multitude of eponymous signs to be cognizant of on physical examination. Some of these include hyperpigmentation of the superior fold of the eyelid (Jellinek's sign), hyperpigmentation of the inferior eyelid (Tella's sign), and fine tremors of the eyelids when closed (Rosenbach's sign). When looking at a close object, one notices the lack of convergence (Moebius' sign); on fundoscopic examination, the retinal arteries can sometimes be seen to be pulsating (Beck's sign). When placing a stethoscope over the closed eyelid, one can sometimes hear a systolic murmur (Snellen-Rieseman's sign).[10]
Evaluation
Once a physician has obtained the full history and physical examination as above, the next step (if not already done) is to obtain thyroid function tests. These should include a TSH and free T4. Also, testing TSH receptor antibody levels is important, not only to help confirm the diagnosis but also to be used as a measure of severity and in tracking response to treatment.[2]
There are a variety of scoring systems used to classify Graves orbitopathy. The first described was the modified NO SPECS criteria, which assist in classifying severity, but not necessarily clinical activity. There are four grades; 0 being no signs or symptoms, I is only limited signs (i.e., lid retraction/lag), II is involvement of soft tissues, III is the presence of proptosis, and IV is if there is any extra-ocular muscle involvement. [11] An additional scoring tool that is useful in classifying the disease as mild, moderate-to-severe, and sight-threatening is the EUGOGO (European Group on Graves’ Orbitopathy) classification.[5] The VISA classification is another means to assess severity. It takes into account vision changes, evidence of inflammation/congestion such as chemosis, conjunctival redness, strabismus/restricted motility of the eye and appearance (proptosis, lid retraction) or exposure (those symptoms and signs related to exposure keratopathy).[5] At this point, a scoring system should be applied to determine how clinically active the Graves’ orbitopathy is. This scoring system is called the CAS (clinical activity score). If a score is obtained and is more than or equal to 3 on the initial assessment, this is clinically active Graves orbitopathy.[12] A score of 4 or more on follow-up visits is considered clinically active as on follow-up evaluation, including dynamic changes. Such clinically active Graves orbitopathy should prompt both immediate ophthalmology evaluation as well as immediate initiation of treatment.
Next, evaluating a patient with Graves orbitopathy should include a consideration of imaging. MRI is a helpful modality in identifying those with clinically active disease, and this may help decide which patients may respond better to immunomodulatory therapy. MRI is also useful if the presentation of the orbitopathy is atypical or asymmetrical to exclude other ocular pathology that may be on the differential. Also, if one suspects there may be orbital nerve compression, an MRI would help to determine this. Concerning the CT scan, this imaging modality does not help in determining clinical activity but may be useful in the planning stages of orbital decompression surgery.[13]
Treatment / Management
The treatment options divide according to those that are supportive and those that are specific. The basis for the decision of which measures to implement is largely on disease severity.
Supportive measures are necessary for all patients. They include ensuring adequate ocular lubrication with lubricating eye drops, eye patches, and prism correction that may help with diplopia and finally elevating the head of the bed that may assist with swelling.
Selenium has been described in some studies to be of benefit in mild disease, but these studies took place in areas with a relative selenium deficiency; thus, the benefit is not certain in selenium-rich environments.[14](A1)
Additional considerations in management include smoking cessation and rendering the patient euthyroid. Such treatment includes thionamides, radioiodine, or surgery. Those with moderate to severe Graves' orbitopathy have a contraindication to radioiodine, and thus, thionamides or surgery would be the preferred option in most patients. Total thyroidectomy is preferred over subtotal thyroidectomy as more thyroid autoantigens get removed.[15] Those with mild eye disease are still candidates for any treatment modality.[16](A1)
Other treatment options include glucocorticoids. These should be options in patients with clinically active disease (CAS 3 or above) and those classified as having moderate-to-severe disease (EUGOGO classification). Oral prednisone or intravenous methylprednisolone can be considerations for moderate disease, but those with severe disease should start on IV therapy. In terms of IV dosing, various studies have quoted different regimens. Due to reduced adverse events and better outcomes, generally preferred is a weekly infusion of 500 mg of methylprednisolone for 6 weeks, followed by 250 mg infused weekly for another 6 weeks (a total dose of 4.5 g).[17] Care should be taken to monitor and prevent side effects of prolonged glucocorticoid use.(A1)
Second-line agents that are options if there is an intolerance or insufficient response to glucocorticoids include other immunomodulators such as rituximab and mycophenolate, external orbital radiation, or orbital decompression surgery.[18][19] Mycophenolate is still under investigation in the treatment of Graves orbitopathy. (B3)
Teprotumumab is an insulin-like growth factor-1 (IGF-1) receptor antagonist. It was approved by the US Food and Drug Administration (FDA) in 2020 for the use in active moderate-to-severe Graves orbitopathy. This was based on 2 studies each of which lasted 24 weeks. Teprotumumab was compared to a placebo in a combined total of 171 patients between the two studies with active moderate-to-severe Graves eye disease. Both studies demonstrated that Teprotumumab was superior to placebo in the reduction of proptosis and clinical activity score.[20][21] The first study by Smith et al. (2017) demonstrated that 69% of patients in the Teprotumumab group as opposed to 20% in the placebo group had a response at 24 weeks. A response was defined as having a 2 or more point reduction in the clinical activity score and a 2mm or more reduction in proptosis.[20] In the second study by Douglas et al. (2020) 83% of patients in the Teprotumumab group compared with only 10% in the placebo group had a proptosis response. Also, 59% of those in the Teprotumumab group had a clinical activity score of 0-1 compared with only 21% in the placebo group. In addition, the number needed to treat in this study was only 1.36.[21] Teprotumumab is an intravenous infusion with an initial dose of 10mg/kg followed by 20mg/kg every 3 weeks for 7 subsequent doses. Some of the reported adverse effects include nausea, diarrhea, alopecia, hyperglycemia, fatigue, and muscle spasms.
Sight-threatening Graves orbitopathy is a medical emergency. Patients should be immediately hospitalized and receive intravenous glucocorticoids, and they may also need urgent orbital decompression surgery.
Orbital decompression surgery has been shown to be best performed after steroids, when the eye disease is quiescent or emergently if the orbitopathy is sight-threatening. Indications for surgery include the development of optic neuropathy, excessive proptosis resulting in corneal complications, aesthetic indications, relief of pain, and severe inflammation or progressive eye disease that does not respond to other measures.[22] Orbital decompression surgery usually involves either removal of the roof, lateral wall, or the medial wall and the floor (transantral approach).[23] In addition, other surgical techniques have been described to correct various aspects of Graves orbitopathy. Some of these include removal of retroocular adipose tissue, which can assist cosmetically in patients with moderate Graves orbitopathy with proptosis.[24] Other surgical modalities include surgery to correct the lid retraction and restrictive myopathy.[25]
Regarding external beam radiation, its role is generally limited to those patients who do not respond to other treatment modalities. Side effects such as chronically dry eyes and a theoretical risk of tumor induction restrict its use. Its proposed mechanism of action is on modulating the immune system. The most common regimen is a 2-week course of 10 sessions with a cumulative dose of 20Gy.[25]
The management of Graves orbitopathy in children is largely similar to that of adults. Firstly one needs to render the child euthyroid, with antithyroid drugs being the first-line treatment. For the orbitopathy, clinical monitoring is often acceptable. Steroids can be used in select cases when no improvement or worsening of eye manifestations occurs despite being euthyroid. Surgery is rarely indicated, and orbital radiation has no role in juvenile Graves orbitopathy, given the potential risk for inducing tumor formation.[26]
In the pregnant patient, management is reasonably similar to the non-pregnant patient. Antithyroid drugs are the mainstay, radioactive iodine is contraindicated, and thyroidectomy is a consideration should the Graves disease be uncontrolled with maximal dosing of antithyroid medication. Propylthiouracil (PTU) is the preferred agent during the first trimester of pregnancy. Should the Graves orbitopathy be severe, there is a role for steroids and orbital decompression surgery, especially if sight-threatening.[27](B3)
Differential Diagnosis
- Orbital tumors:
- Primary
- Secondary/metastatic
- Myositis of the extraocular muscles (sarcoidosis)
- Orbital cellulitis
- Ocular myasthenia gravis
- Statin-induced extraocular muscle myopathy
- Hashimoto thyroiditis
- Histiocytosis
- Carotid cavernous fistula[28]
Prognosis
The natural course of Graves orbitopathy is varied. Some patients have stable mild orbitopathy, while others may develop either worsening or improvement of the disease after many years. One study showed that the development of moderate-to-severe orbitopathy over 18 months appeared in an average of 2.5% of patients. That same study showed 58% of patients with mild disease went into complete remission.[6]
Regarding the prognosis after treatment with glucocorticoids, which is the mainstay of therapy for active moderate-to-severe disease, a systematic review demonstrated that IV steroids were better than oral with an outcome measurement of symptom reduction. An 82% reduction occurred with IV vs. a 53% reduction with oral therapy.[29]
Complications
Complications of Graves eye disease range from clinically mild manifestations such as conjunctival inflammation and eye dryness, to severe sight-threatening complications such as extraocular muscle entrapment, corneal ulcers, and optic nerve compression.
Consultations
Necessary consults should include both endocrinology and ophthalmology.
Pearls and Other Issues
Important to note is that the clinical signs of lid lag and lid retraction are not specifically due to Graves orbitopathy. These signs can present in any thyrotoxic state due to sympathetic hyperactivity. The mechanism is related to excess catecholamines acting on the smooth muscle portion of the levator palpebrae superioris muscle called Muller's muscle, resulting in lid retraction and then subsequently lid lag.
Another important association is that of Graves orbitopathy and ocular myasthenia gravis. Not only is myasthenia gravis a differential for Graves orbitopathy, but the two diseases may also occur concurrently. Studies have shown that 0.2% of patients with thyroid disease develop myasthenia gravis, and conversely, in those with established myasthenia gravis, 5 to 7.5% of patients have or develop autoimmune thyroid disease. Therefore it is vital to be vigilant when examining the eye, paying particular attention towards the end of the examination to see if any fatiguability is present that will manifest as ptosis. Ptosis is not a clinical feature of Graves eye disease, and so when noticed, it should prompt further investigation for ruling out myasthenia gravis.[30][31]
Enhancing Healthcare Team Outcomes
Graves eye disease requires an interprofessional team approach. This includes the primary physician (whether hospitalist, primary care physician or the first point of contact with the patient), endocrinologist to render the patient euthyroid and assess the best treatment modality with an individualized approach, ophthalmologist to adequately examine the eye, track the progression and distinguish those who need orbital decompression surgery, pharmacist to assist with dosing of steroids and other immunomodulators, nursing staff to administer treatment when patients require hospitalization as well as counsel the patient as shown below, and finally a radiologist to interpret necessary imaging studies. This interprofessional team approach will ensure maximum patient benefit with minimal downside. [Level V]
Graves eye disease can be distressing to most patients. Important patient education includes smoking cessation as this is a significant risk factor for Graves orbitopathy, and also the importance of local measures, especially eye patches and lubricating eye drops to help prevent corneal complications. Patients require education to understand that little is known about the natural history of the disease and that regular follow up with both ophthalmology and endocrinology specialists is of vital importance to track progression and see if escalation of treatment at any point is necessary. Patients should understand that if they notice any change in their vision, or develop any new symptoms such as pain with eye movement, they should seek urgent medical attention.
Additionally, not to forget, the appearance of Graves eye disease can be emotionally distressing and physically debilitating depending on the disease severity. Social worker consult may be of benefit not only for the patient to be able to talk with someone, but also if the disease is sight-threatening, to coordinate any additional assistance that is available to them. Social workers would also be helpful ascertaining if the patient has strong psychosocial support and adequate follow-up potential as this disease process can be unpredictable.
Media
(Click Image to Enlarge)

Graves orbitopathy Image courtesy S Bhimji MD
(Click Image to Enlarge)
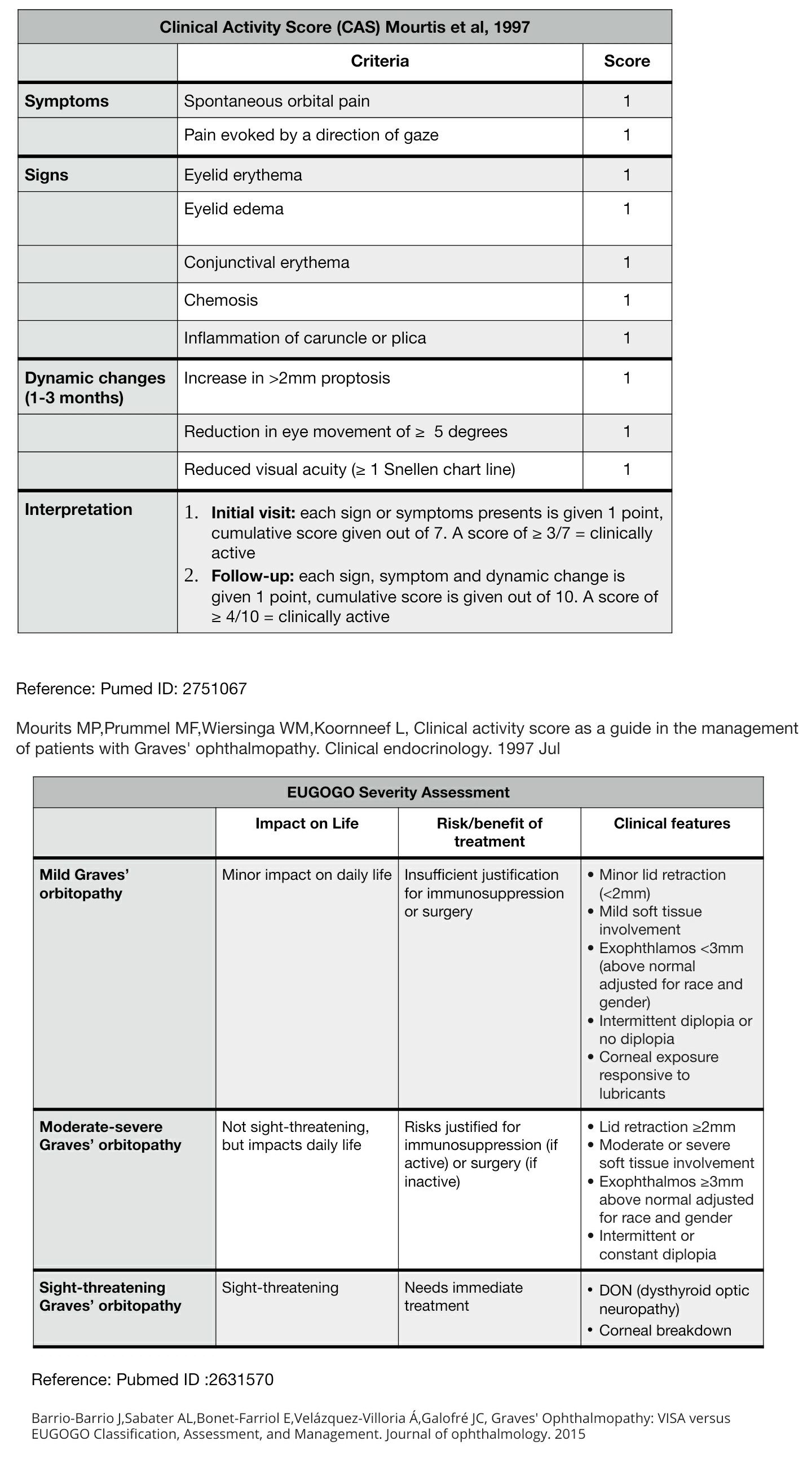
Graves Orbitopathy Tables Contributed by Tamaryn Fox, MD
References
Bahn RS. Graves' ophthalmopathy. The New England journal of medicine. 2010 Feb 25:362(8):726-38. doi: 10.1056/NEJMra0905750. Epub [PubMed PMID: 20181974]
Eckstein AK,Plicht M,Lax H,Neuhäuser M,Mann K,Lederbogen S,Heckmann C,Esser J,Morgenthaler NG, Thyrotropin receptor autoantibodies are independent risk factors for Graves' ophthalmopathy and help to predict severity and outcome of the disease. The Journal of clinical endocrinology and metabolism. 2006 Sep; [PubMed PMID: 16835285]
Şahlı E, Gündüz K. Thyroid-associated Ophthalmopathy. Turkish journal of ophthalmology. 2017 Apr:47(2):94-105. doi: 10.4274/tjo.80688. Epub 2017 Apr 1 [PubMed PMID: 28405484]
Valyasevi RW, Erickson DZ, Harteneck DA, Dutton CM, Heufelder AE, Jyonouchi SC, Bahn RS. Differentiation of human orbital preadipocyte fibroblasts induces expression of functional thyrotropin receptor. The Journal of clinical endocrinology and metabolism. 1999 Jul:84(7):2557-62 [PubMed PMID: 10404836]
Barrio-Barrio J, Sabater AL, Bonet-Farriol E, Velázquez-Villoria Á, Galofré JC. Graves' Ophthalmopathy: VISA versus EUGOGO Classification, Assessment, and Management. Journal of ophthalmology. 2015:2015():249125. doi: 10.1155/2015/249125. Epub 2015 Aug 17 [PubMed PMID: 26351570]
Tanda ML, Piantanida E, Liparulo L, Veronesi G, Lai A, Sassi L, Pariani N, Gallo D, Azzolini C, Ferrario M, Bartalena L. Prevalence and natural history of Graves' orbitopathy in a large series of patients with newly diagnosed graves' hyperthyroidism seen at a single center. The Journal of clinical endocrinology and metabolism. 2013 Apr:98(4):1443-9. doi: 10.1210/jc.2012-3873. Epub 2013 Feb 13 [PubMed PMID: 23408569]
Level 2 (mid-level) evidenceHiromatsu Y,Eguchi H,Tani J,Kasaoka M,Teshima Y, Graves' ophthalmopathy: epidemiology and natural history. Internal medicine (Tokyo, Japan). 2014; [PubMed PMID: 24583420]
Villadolid MC, Yokoyama N, Izumi M, Nishikawa T, Kimura H, Ashizawa K, Kiriyama T, Uetani M, Nagataki S. Untreated Graves' disease patients without clinical ophthalmopathy demonstrate a high frequency of extraocular muscle (EOM) enlargement by magnetic resonance. The Journal of clinical endocrinology and metabolism. 1995 Sep:80(9):2830-3 [PubMed PMID: 7673432]
Dickinson AJ, Perros P. Controversies in the clinical evaluation of active thyroid-associated orbitopathy: use of a detailed protocol with comparative photographs for objective assessment. Clinical endocrinology. 2001 Sep:55(3):283-303 [PubMed PMID: 11589671]
Level 2 (mid-level) evidenceSaraci G, Treta A. Ocular changes and approaches of ophthalmopathy in basedow - graves- parry- flajani disease. Maedica. 2011 Apr:6(2):146-52 [PubMed PMID: 22205899]
Werner SC. Modification of the classification of the eye changes of Graves' disease. American journal of ophthalmology. 1977 May:83(5):725-7 [PubMed PMID: 577380]
Mourits MP, Prummel MF, Wiersinga WM, Koornneef L. Clinical activity score as a guide in the management of patients with Graves' ophthalmopathy. Clinical endocrinology. 1997 Jul:47(1):9-14 [PubMed PMID: 9302365]
Level 1 (high-level) evidenceKirsch E, von Arx G, Hammer B. Imaging in Graves' orbitopathy. Orbit (Amsterdam, Netherlands). 2009:28(4):219-25 [PubMed PMID: 19839878]
Marcocci C, Kahaly GJ, Krassas GE, Bartalena L, Prummel M, Stahl M, Altea MA, Nardi M, Pitz S, Boboridis K, Sivelli P, von Arx G, Mourits MP, Baldeschi L, Bencivelli W, Wiersinga W, European Group on Graves' Orbitopathy. Selenium and the course of mild Graves' orbitopathy. The New England journal of medicine. 2011 May 19:364(20):1920-31. doi: 10.1056/NEJMoa1012985. Epub [PubMed PMID: 21591944]
Level 1 (high-level) evidenceChiovato L, Latrofa F, Braverman LE, Pacini F, Capezzone M, Masserini L, Grasso L, Pinchera A. Disappearance of humoral thyroid autoimmunity after complete removal of thyroid antigens. Annals of internal medicine. 2003 Sep 2:139(5 Pt 1):346-51 [PubMed PMID: 12965943]
Level 2 (mid-level) evidenceLaurberg P, Wallin G, Tallstedt L, Abraham-Nordling M, Lundell G, Tørring O. TSH-receptor autoimmunity in Graves' disease after therapy with anti-thyroid drugs, surgery, or radioiodine: a 5-year prospective randomized study. European journal of endocrinology. 2008 Jan:158(1):69-75. doi: 10.1530/EJE-07-0450. Epub [PubMed PMID: 18166819]
Level 1 (high-level) evidenceTu X, Dong Y, Zhang H, Su Q. Corticosteroids for Graves' Ophthalmopathy: Systematic Review and Meta-Analysis. BioMed research international. 2018:2018():4845894. doi: 10.1155/2018/4845894. Epub 2018 Nov 22 [PubMed PMID: 30596092]
Level 1 (high-level) evidenceSalvi M, Vannucchi G, Campi I, Rossi S, Bonara P, Sbrozzi F, Guastella C, Avignone S, Pirola G, Ratiglia R, Beck-Peccoz P. Efficacy of rituximab treatment for thyroid-associated ophthalmopathy as a result of intraorbital B-cell depletion in one patient unresponsive to steroid immunosuppression. European journal of endocrinology. 2006 Apr:154(4):511-7 [PubMed PMID: 16556712]
Level 3 (low-level) evidenceYe X, Bo X, Hu X, Cui H, Lu B, Shao J, Wang J. Efficacy and safety of mycophenolate mofetil in patients with active moderate-to-severe Graves' orbitopathy. Clinical endocrinology. 2017 Feb:86(2):247-255. doi: 10.1111/cen.13170. Epub 2016 Sep 7 [PubMed PMID: 27484048]
Smith TJ, Kahaly GJ, Ezra DG, Fleming JC, Dailey RA, Tang RA, Harris GJ, Antonelli A, Salvi M, Goldberg RA, Gigantelli JW, Couch SM, Shriver EM, Hayek BR, Hink EM, Woodward RM, Gabriel K, Magni G, Douglas RS. Teprotumumab for Thyroid-Associated Ophthalmopathy. The New England journal of medicine. 2017 May 4:376(18):1748-1761. doi: 10.1056/NEJMoa1614949. Epub [PubMed PMID: 28467880]
Douglas RS, Kahaly GJ, Patel A, Sile S, Thompson EHZ, Perdok R, Fleming JC, Fowler BT, Marcocci C, Marinò M, Antonelli A, Dailey R, Harris GJ, Eckstein A, Schiffman J, Tang R, Nelson C, Salvi M, Wester S, Sherman JW, Vescio T, Holt RJ, Smith TJ. Teprotumumab for the Treatment of Active Thyroid Eye Disease. The New England journal of medicine. 2020 Jan 23:382(4):341-352. doi: 10.1056/NEJMoa1910434. Epub [PubMed PMID: 31971679]
Garrity JA, Fatourechi V, Bergstralh EJ, Bartley GB, Beatty CW, DeSanto LW, Gorman CA. Results of transantral orbital decompression in 428 patients with severe Graves' ophthalmopathy. American journal of ophthalmology. 1993 Nov 15:116(5):533-47 [PubMed PMID: 8238212]
Ogura JH, Thawley SE. Orbital decompression of exophthalmos. Otolaryngologic clinics of North America. 1980 Feb:13(1):29-38 [PubMed PMID: 7367005]
Garrity JA. Orbital lipectomy (fat decompression) for thyroid eye disease: an operation for everyone? American journal of ophthalmology. 2011 Mar:151(3):399-400. doi: 10.1016/j.ajo.2010.10.036. Epub [PubMed PMID: 21335108]
San Miguel I, Arenas M, Carmona R, Rutllan J, Medina-Rivero F, Lara P. Review of the treatment of Graves' ophthalmopathy: The role of the new radiation techniques. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2018 Apr-Jun:32(2):139-145. doi: 10.1016/j.sjopt.2017.09.003. Epub 2017 Sep 21 [PubMed PMID: 29942184]
Gogakos AI, Boboridis K, Krassas GE. Pediatric aspects in Graves' orbitopathy. Pediatric endocrinology reviews : PER. 2010 Mar:7 Suppl 2():234-44 [PubMed PMID: 20467370]
Stafford IP, Dildy GA 3rd, Miller JM Jr. Severe Graves' ophthalmopathy in pregnancy. Obstetrics and gynecology. 2005 May:105(5 Pt 2):1221-3 [PubMed PMID: 15863589]
Level 3 (low-level) evidenceBoddu N, Jumani M, Wadhwa V, Bajaj G, Faas F. Not All Orbitopathy Is Graves': Discussion of Cases and Review of Literature. Frontiers in endocrinology. 2017:8():184. doi: 10.3389/fendo.2017.00184. Epub 2017 Jul 31 [PubMed PMID: 28824545]
Level 3 (low-level) evidenceStiebel-Kalish H, Robenshtok E, Hasanreisoglu M, Ezrachi D, Shimon I, Leibovici L. Treatment modalities for Graves' ophthalmopathy: systematic review and metaanalysis. The Journal of clinical endocrinology and metabolism. 2009 Aug:94(8):2708-16. doi: 10.1210/jc.2009-0376. Epub 2009 Jun 2 [PubMed PMID: 19491222]
Level 1 (high-level) evidenceRatanakorn D, Vejjajiva A. Long-term follow-up of myasthenia gravis patients with hyperthyroidism. Acta neurologica Scandinavica. 2002 Aug:106(2):93-8 [PubMed PMID: 12100368]
Yeh HH, Tung YW, Yang CC, Tung JN. Myasthenia gravis with thymoma and coexistent central hypothyroidism. Journal of the Chinese Medical Association : JCMA. 2009 Feb:72(2):91-3. doi: 10.1016/S1726-4901(09)70030-9. Epub [PubMed PMID: 19251538]
Level 3 (low-level) evidence