Introduction
The branches of the ophthalmic artery comprise the entire arterial supply to the eye. Most commonly the ophthalmic artery branches off of the internal carotid artery, distal to the cavernous sinus, then travels through the optic canal. The ophthalmic artery has multiple branches which separate into two categories: orbital branches and optical branches. The orbital arteries include the ciliary arteries, central retinal artery, and muscular arteries.[1]
- Long Posterior Ciliary Arteries: The long posterior ciliary arteries (1 to 2) travel near the optic nerve and pierce the posterior sclera to supply the choroid and ciliary muscle before joining the major arterial circle of the iris.[2] The major arterial circle of the iris distributes branches to the iris and ciliary body.
- Short Posterior Ciliary Arteries: The number of short posterior ciliary arteries vary per individual, often ranging between 6 to 12 arteries that branch off the ophthalmic artery as it crosses the optic nerve medially. These arteries supply the ciliary processes and optic disk. The arterioles branching from the posterior ciliary arteries supply the choroid. The perpendicular terminal arterioles supply choriocapillaris, the blood supply to Bruch’s membrane and outer retina.[3]
- Anterior Ciliary Arteries: There are seven anterior ciliary arteries that branch from the muscular arteries and run with the extraocular muscles. The anterior ciliary arteries supply the rectus muscles, conjunctiva, and sclera before joining the long posterior ciliary arteries to form the major arterial circle of the iris.[2] Each rectus muscle receives its vascular supply from two anterior ciliary arteries, except the lateral rectus which receives blood supply from only one anterior ciliary artery.
- Central Retinal Artery: It is the first branch of the ophthalmic artery. It is a terminal branch supplying the inner layer of the retina, and its occlusion can cause sudden visual loss. It travels inferiorly and within the optic nerve sheath to supply the inner two-thirds of the retina. The artery further divides into superior and inferior arcades, which form the blood-retina barrier.
- Muscular branches: The two muscular branches of the ophthalmic artery that supply extraocular muscles include the medial and lateral muscular branches. The medial artery being larger than the lateral muscular branch.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The structure of eye arteries is similar to that of arteries throughout the body. Arteries are considered rigid vessels in comparison to veins. The arterial wall consists of a tunica intima, tunica media, and tunica externa. Arteries in the eye are also susceptible to damage by glycosylation reactions and plaque deposition in patients with diabetes and hypertension which are two common risk factors for ocular pathology.[4]
Embryology
Eye development takes place from week 3 to week 10. Ocular blood vessels originate from mesenchyme. First, optic grooves grow outward, forming optic vesicles. The optic vesicles attach to the forebrain via the optic stalk which later becomes the optic nerve. On the inferior surface of the optic vesicles and stalk a C-shaped fissure, known as the choroidal fissure, forms. The choroidal fissure serves as the entrance point for blood vessels. Through this fissure, the hyaloid artery can access the growing lens.[5] By week 10, the distal portion of the hyaloid artery disintegrates, and the proximal portion remains as the central retinal artery.
Persistent fetal vasculature can lead to impairment in vision or even blindness. Ocular examination findings vary depending on degree and area of vessel persistence.[6]
Blood Supply and Lymphatics
Ocular lymphatics correlate more closely with the venous system. Findings show that ocular structures differ in their lymphatic makeup. The retina is lymphatic free, the lacrimal glands are lymphatic rich, and the iris is lymphatic inducible.[7]
Nerves
The ophthalmic artery and its branches travel near the optic nerve. The central retinal artery runs in the dural sheath of the optic nerve. The central retinal artery also has a sympathetic nerve plexus, called the nerve of Tiedemann that surrounds the neurovascular bundle.
Muscles
Ciliary muscles and the six extrinsic eye muscles receive vascular supply by branches of the ophthalmic artery. Long posterior ciliary arteries provide blood to the ciliary muscles. The superior, lateral, medial and inferior rectus muscles receive blood from anterior ciliary arteries. Each rectus muscle receives supply from two anterior ciliary arteries, except the lateral rectus which receives blood from only one artery. The lateral muscular artery also supplies the lateral and superior rectus as well as the superior oblique muscle. The medial muscular branch supplies the inferior and medial rectus and inferior oblique muscles.
Physiologic Variants
Most commonly the ophthalmic artery originates from the internal carotid artery. However, in 2 to 3% of individuals, the ophthalmic artery has a different origin. It has been found to arise from the anterior cerebral artery, middle cerebral artery, posterior communicating artery, or the middle meningeal artery. [5]
The most common variant is that of the ophthalmic artery originating from the middle meningeal artery.[8] During embryologic development, the stapedial artery, an orbital branch of the middle meningeal artery enters the orbit through the canal of Hyrtl to supply the developing eye.[1] Anastomoses between the ophthalmic artery and middle meningeal artery may persist.[8]
Surgical Considerations
Knowledge of the ophthalmic artery branches and origin is of significant importance in regards to treatment for head and neck tumors or persistent epistaxis.[8] Determination of the ophthalmic artery origin must occur before middle meningeal artery embolization. If the ophthalmic artery originates from the middle meningeal artery, its occlusion will expectedly result in severe visual impairment or blindness.
The ophthalmic artery branches distal to the cavernous sinus enter the optic canal. This short intracranial course is of surgical importance as it is the site of surgical intervention for ophthalmic artery aneurysms.[8] Surgical treatment for ophthalmic artery aneurysms should be done cautiously due to proximity to the optic nerve, optic canal, and clinoid process.
Clinical Significance
Central retinal artery occlusion (CRAO) is a stroke of the eye. The central retinal artery is an end artery; hence, its occlusion presents with sudden, painless monocular vision loss. CRAO is an ophthalmologic emergency. Individuals with carotid artery disease and atherosclerotic plaque deposition are at highest risk. Emboli are the most common etiology of CRAO. On ocular examination, patients may have a cherry-red spot (90%), retinal opacity in the posterior pole (58%), optic disk pallor (39%), retinal arterial attenuation (32%), optic disk edema (22%), intra-arterial emboli (20%), and/or cattle trucking (19%).[3] On fluorescein angiography, delayed filling time of the affected vessel may be present. Treatment includes acute reperfusion of the central retinal artery and prevention of future vascular ischemic events. Carotid duplex is the recommendation when a patient presents with painless, monocular vision loss because of the high risk of another ischemic event.[9][10]
The definition of amaurosis fugax is transient vision loss, often monocular and painless. The pathophysiology is similar to that of CRAO: occlusion or stenosis within the internal carotid circulation. Similar to CRAO, on ocular examination one may find cholesterol plaques (Hollenhorst plaques). Amaurosis fugax is also a manifestation of fibromuscular dysplasia and may be suggestive of brain ischemia in patients with this diagnosis. [11]
Retinoblastoma is a childhood ocular tumor. One treatment method is intra-arterial chemotherapy.[12] Selective occlusion of eye arteries has proven to have less systemic side effects in comparison to systemic chemotherapy.
Ocular manifestations of hypertension, aptly named hypertensive retinopathy, are seen as progressive microvascular changes. In its mild form, examination reveals mild arteriolar narrowing and arteriovenous nicking. [4] As the disease progresses there may be evidence of microaneurysms, hemorrhage, and cotton-wool spots.
Other Issues
The choriocapillaris supplies the outer layer of the retina including the fovea centralis, the area of the highest cone concentration in the retina.
The ophthalmic artery has branches that enter the eye (optic branches) and orbital branches. The orbital branches include:
- Lacrimal Artery: The second and largest branch of the ophthalmic artery. It enters the orbit and travels alongside the lacrimal nerve to supply the lacrimal gland. Its terminal branches supply the eyelids and conjunctiva.[13]
- Supraorbital Artery: This artery travels medially, through the supraorbital foramen to supply the levator palpebrae superioris, frontal sinus, and skin of the forehead.
- Posterior Ethmoidal Artery: Supplies the posterior ethmoidal sinuses and meninges.
- Anterior Ethmoidal Artery: Supplies the anterior/middle ethmoid and frontal sinuses.
- Medial Palpebral Artery: Creates two additional branches, superior and inferior medial palpebral arteries, all of which contribute to the eyelids blood supply.
Media
(Click Image to Enlarge)
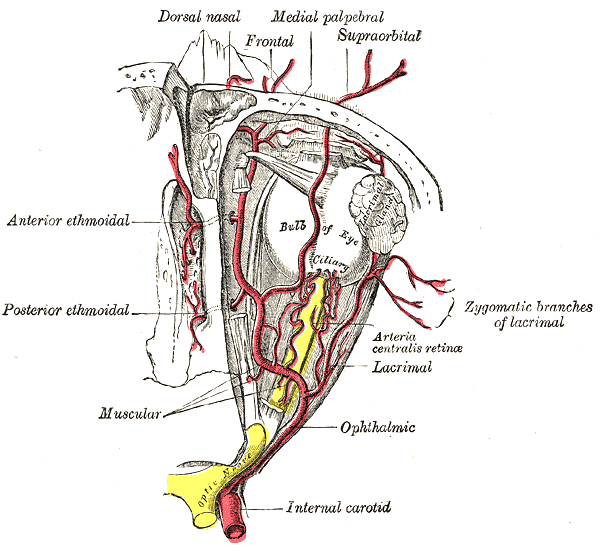
Arteries of the Eye. This illustration shows the anatomic relationships between the internal carotid artery and the ophthalmic artery and its branches.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Toma N. Anatomy of the Ophthalmic Artery: Embryological Consideration. Neurologia medico-chirurgica. 2016 Oct 15:56(10):585-591 [PubMed PMID: 27298261]
Rehman I, Mahabadi N, Ali T. Anatomy, Head and Neck, Eye Ciliary Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 29489160]
Varma DD, Cugati S, Lee AW, Chen CS. A review of central retinal artery occlusion: clinical presentation and management. Eye (London, England). 2013 Jun:27(6):688-97. doi: 10.1038/eye.2013.25. Epub 2013 Mar 8 [PubMed PMID: 23470793]
Wong TY, Mitchell P. Hypertensive retinopathy. The New England journal of medicine. 2004 Nov 25:351(22):2310-7 [PubMed PMID: 15564546]
Vignaud J, Hasso AN, Lasjaunias P, Clay C. Orbital vascular anatomy and embryology. Radiology. 1974 Jun:111(3):617-26 [PubMed PMID: 4828995]
Mehta A, Singh SR, Dogra M, Ram J. Persistent fetal vasculature - Clinical spectrum. Indian journal of ophthalmology. 2018 Dec:66(12):1860. doi: 10.4103/ijo.IJO_1042_18. Epub [PubMed PMID: 30451201]
Chen L. Ocular lymphatics: state-of-the-art review. Lymphology. 2009 Jun:42(2):66-76 [PubMed PMID: 19725271]
Michalinos A, Zogana S, Kotsiomitis E, Mazarakis A, Troupis T. Anatomy of the Ophthalmic Artery: A Review concerning Its Modern Surgical and Clinical Applications. Anatomy research international. 2015:2015():591961. doi: 10.1155/2015/591961. Epub 2015 Nov 9 [PubMed PMID: 26635976]
Tripathy K, Shah SS, Waymack JR. Central Retinal Artery Occlusion. StatPearls. 2024 Jan:(): [PubMed PMID: 29262124]
Hayreh SS. Central retinal artery occlusion. Indian journal of ophthalmology. 2018 Dec:66(12):1684-1694. doi: 10.4103/ijo.IJO_1446_18. Epub [PubMed PMID: 30451166]
Mettinger KL. Fibromuscular dysplasia and the brain. II. Current concept of the disease. Stroke. 1982 Jan-Feb:13(1):53-8 [PubMed PMID: 7039003]
Kim J, Do H, Egbert P. Enucleated eyes after failed intra-arterial infusion of chemotherapy for unilateral retinoblastoma: histopathologic evaluation of vitreous seeding. Clinical ophthalmology (Auckland, N.Z.). 2011:5():1655-8. doi: 10.2147/OPTH.S24318. Epub 2011 Nov 24 [PubMed PMID: 22174572]
Level 3 (low-level) evidenceBird B, Stawicki SP. Anatomy, Head and Neck, Ophthalmic Arteries. StatPearls. 2023 Jan:(): [PubMed PMID: 29493942]