Introduction
Migraine is a primary neurologic headache, often accompanied by nausea, vomiting, photophobia, phonophobia, or vertigo, and may present with or without aura.[1] It is prevalent in 11.7% of Americans with 17.1% in women, and 5.6% in men.[2] Migraine can be acute or chronic. Treatment of this condition includes beta-blockers, anticonvulsants, calcium channel blockers, tricyclic antidepressants, non-steroidal anti-inflammatory drugs, among others.[3] Migraine surgery is indicated when the condition is refractory to medical management.
Chronic migraine is defined by the International Headache Society classification of headache disorders (ICHD-3). It is described as:
- Headache occurring on ≥15 days/month
- Duration > 3 months
- Having features of migraine on ≥8 days/month
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
There are several theories for migraine generation. Previously, vasodilation of the cerebral vasculature was proposed as the mechanism, but it has been refuted by several experiments that showed an absence of migraine with the vasoactive intestinal peptide that increases the blood flow.[4] Similarly, the drugs precipitating migraine, like sildenafil do not cause sustained vascular changes.[5] There is evidence to show cortical and brainstem hyperexcitability in a headache,[6][7] and cortical spreading depression are responsible for the aura.[8] There is evidence that shows trigeminal afferents projecting to meninges and releasing pain mediators like substance P, calcitonin gene-related peptide, and neurokinin A, thus causing a vicious cycle of sterile meningitis.[9] The strongest clinical evidence points toward the peripheral origin of a migraine. This is supported by the beneficial effect of Botulinum toxin and peripheral neurolysis for a chronic migraine, which is detailed in the following paragraphs.
Migraine surgery focuses on the neurolysis of sensory branches of trigeminal and occipital nerves supplying the face and back of the head. These nerves include supraorbital, supratrochlear, zygomaticotemporal, auriculotemporal, and greater and lesser occipital nerves. Sometimes, the pain is also due to hypertrophic nasal turbinates or deviated nasal septum irritating branches of trigeminal nerves.
Indications
Migraine surgery is indicated when the disease is not controlled by conservative measures, which include medicines and behavioral therapy.
Contraindications
A confirmed psychiatric disease is a relative contraindication.
Personnel
A neurologist should initially evaluate all cases.
Preparation
The assessment of migraine severity can be done through several scales, of which the most commonly used is the Migraine Disability Assessment Questionnaire (MIDAS).[10] In this, 0 to 5 score is labeled as MIDAS grade I (little or no disability), 6 to 10 as MIDAS grade II (mild disability), 11 to 20 as MIDAS grade III (moderate disability), 21 and higher as MIDAS grade IV (severe disability).
The initial treatment of a migraine is with drugs and behavioral methods, but often, patients develop refractoriness to these therapies.[11][12] ICHD-3 beta has amended the definition of a refractory migraine as along with existent criteria, monthly migraine headaches of at least 8, with 15 or more headache days a month. A flowchart showing a management paradigm is shown in Figure 1.
When there is suspicion of a rhinogenic headache, the clinician can order a computed tomography (CT) scan of the nose and paranasal sinuses.
Technique or Treatment
Botulinum Toxin
Botulinum toxin has to be instilled into pericranial muscles at multiple sites according to pain. The safe and effective dose is 25 units in total after mixing with normal saline. This can be divided into 3 units for temporalis each side (total 6 units), 2.5 units at 4 frontalis sites (5 units unilaterally; 10 units for both sides), 3 units at corrugators on each side (total 6 units), and 3 units for procerus in the midline.[13] For occipital headaches, one can instill about 12.5 to 50 units on each side of the midline in the region of greater and lesser occipital nerves. Pain relief for 6 to 12 weeks indicates an appropriate candidate for the surgery.
Peripheral Neurolysis
Frontal headache: An eyelid incision is used. The orbital septum is retracted caudally and the orbicularis retracted cranially. The corrugator supercilii and depressor supercilii are resected, and the nerves are freed. Both supraorbital and supratrochlear vessels are sacrificed, and the supraorbital foramen is unroofed. The space made is filled with the medial orbital fat and fixed with 6-0 polyglactin 910. The incisions are then closed with 6-0 nylon sutures. This can be done bilaterally.[14]
Anterior Temporal headache: The procedure described is cutting of the zygomaticotemporal nerve. For a frontotemporal headache, it is combined with the procedure for frontal headaches by making 2 incisions, one in the upper tarsal crease and another at the superior temporal line.[15] These can also be done endoscopically.[14] The zygomaticotemporal nerve is found about 16-mm lateral to the lateral canthus and 6-mm cranial to it. A small incision of size 2 cm is made at this point and dissection is done in between the 2 layers of temporalis fascia. The nerve can be found at the lateral margin of orbit. It is cut and the end is buried deep into the muscle. The closure is done in layers.
Posterior temporal headache: For this, the auriculotemporal nerve is the culprit. The incision is made at the base of side burn of a size of 2 cm. The nerve along with the superficial temporal vessels are identified. The vessels are sacrificed. The nerve is isolated for about 1 to 2 cm, is cut, and then buried in the temporalis muscle. The incision is closed in layers.
Occipital headache: In case of an occipital migraine, occipital nerve neurolysis from semispinalis capitis muscle can be performed.[16] For diffuse occipital region pain, one should perform greater occipital neurolysis. A midline incision is made from external occipital protuberance to the C2 spinous process. The trapezius fascia is cut about 1cm off midline. The trapezius fibers are split in line and dissection is performed below it to find the greater occipital nerve. The semispinalis capitis muscle around the nerve is transected to free the nerve. Similarly, the trapezius muscle and fascia over the nerve are removed. The procedure can be repeated on the opposite side also. A pedicled fat is taken from the overlying skin and inserted between the nerve and the muscle and sutured there to be held in place. The incision is then closed with nylon 3-0.
For lateral occipital headache lesser occipital neurolysis or neurectomy can be performed. A 2-cm incision is made about 2 cm medial to the mastoid in the hairline. The thick temporal fascia is incised. The lesser occipital nerve is dissected out along with the vessel. The artery is coagulated and cut. The nerve is dissected out for about 1 to 2 cm, is cut and buried in the muscle. The incision is closed with nylon 3-0.
Occipital neurolysis though has immediate relief but also has high chances of recurrence,[16] and in such cases, alternative options like neuromodulation can be tried.
Rhinogenic headaches: If hypertrophied turbinates or deviated nasal septum is identified as the cause of headaches then turbinectomy or septoplasty is done in the standard manner. The branches of the maxillary nerve through sphenopalatine ganglion mediate this type of headaches and botulinum toxin treatment is not effective in such patients.
Neuromodulation for Migraine
Neuromodulation is done when there is a failure of medical management, peripheral neurolysis is not feasible or has failed. The foremost option is occipital nerve stimulation (ONS). It is done by placing electrodes around cervical dorsal nerves in the suboccipital region and connecting them first to a trial stimulator, and if successful to a permanently implantable pulse generator. Other options of neuromodulation include sphenopalatine ganglion stimulation,[17] supraorbital nerve stimulation,[18][19] and vagus nerve stimulation.[20][21] Though these have proved their beneficial roles in initial studies, large controlled trials are needed.
Nerve Decompression
The decompression of the nerves in trigger site areas (frontal, temporal, occipital) by removing the surrounding tissues including muscles and blood vessels can be useful in patients with medically refractory chronic migraines.[22]
Complications
Botulinum Toxin
One can have transient hollowness of muscles in which the drug is injected, especially the temporalis muscle. The incidence can be around 23%.[23] Other complications may be transient eyelid ptosis (when injected into the eyebrow muscles), or neck muscle weakness (when injected into the cervical region).
Peripheral Neurolysis/Neurectomy
Patients can have neuroma formation when a neurectomy is conducted. This can be prevented by burying the cut nerve end in the muscle. Infection, hemorrhage can be associated, but the incidence is low. Temporary paresthesia and itching in the area of surgery can also be found.[24]
Turbinate Surgery
One can have postoperative epistaxis, sinusitis, nasal dryness, or septal deviation.[23]
Neuromodulation
Lead migration can occur if they are not anchored properly. Infection can be associated, these can generally be managed with antibiotics, and rarely require implant removal.
Clinical Significance
A migraine is a common primary headache. A neurologist evaluates clinical features and the MIDAS score. Initial treatment is through medicines and behavioral therapy. Botulinum toxin is commonly used as a screening tool to identify the triggers. Peripheral neurolysis/neurectomy is an effective treatment for drug-refractory cases.
Enhancing Healthcare Team Outcomes
The migraine patient should be evaluated by an interprofessional team involving a neurologist, psychologist, psychiatrist, surgeon, specialty-trained neurology nurse, and allied health professionals. Appropriate case selection is necessary to have a successful outcome of the surgery. A pharmacist should be involved in helping the team with pharmaceutical selection and maintenance. Nurses should assist in patient education before and after surgery. One should follow the methodology as given in the flowchart.
Botulinum Toxin
Botulinum toxin (BT) is a toxin produced by Clostridium botulinum. It paralyzes muscles by inhibiting the release of acetylcholine from presynaptic terminals. It has 8 subtypes: A through H, of which type A is safe and effective for therapeutic usage.[25] Justinus Kerner discovered the idea of botulinum toxin to be used as a medical therapeutic, which he called botulinum toxin as "sausage poison." He did animal experiments and human experiments, including upon himself.[26] Scott initially used botulinum toxin for strabismus.[25] Thereafter, it was used in focal dystonia like blepharospasm,[27][28] cervical dystonia,[29][30] oromandibular dystonia,[31] laryngeal dystonia,[32] hemifacial spasm,[31][33] writer’s cramp,[34] spasticity, focal hyperhidrosis,[35] and to diagnose and treat trigger factors for migraine.[13] Botulinum toxin reduces migraine frequency and severity by decreasing the irritation of peripheral nerves by paralyzing the triggers, i.e., muscles, and decreasing the inflammatory mediators.[36] Evidence, including double-blinded controlled trials, suggest more than a 50% reduction in frequency and severity of migraines at 3 months, with efficacy lasting 3 to 4 months,[13][37][38] but some other blind trials did not show or show only modest effects of botulinum toxin over placebo.[39][40]
Though botulinum toxin can be used short term as an acute and prophylactic treatment,[13][37] its permanent use is difficult due to the development of resistance with time leading to a decrease in effect, and side-effects like muscle paralysis, muscle atrophy, and irritation, especially with higher doses.[13][41] Therefore, some recommend only using it as a screening tool before the neurolysis.[42]
Peripheral Neurolysis
The beneficial effect of peripheral neurolysis of supratrochlear and supraorbital nerves on migraine was discovered when Guyuron found that his patients were relieved of a debilitating migraine after brow lift surgery.[43] Subsequently, the group published a prospective study confirming the findings.[14] Neurolysis is performed after identification of trigger sites and when pain relief is more than 50% for at least 6 weeks by injecting BT. One can instill BT in the bilateral frontal, temporal, over corrugators, and occipital region (12.5 units each).[14][15] Examination of hypertrophied nasal turbinates irritating the nasal septum should be done.
Neuromodulation
Occipital nerve stimulation (ONS) can have benefits for pain in the distribution of both occipital and trigeminal nerves through the modulatory activity of the trigeminocervical complex. This consists of the trigeminal nucleus and portions of the upper 3 cervical dorsal nerves. It can result in 30% to 50% of patients having more than 50% pain relief.[44][45][46] This procedure has high rates of lead readjustments (around 50%) but that is minimally invasive.[46] ONS can also help in cluster headaches.[47] (Level I and II)
Media
(Click Image to Enlarge)
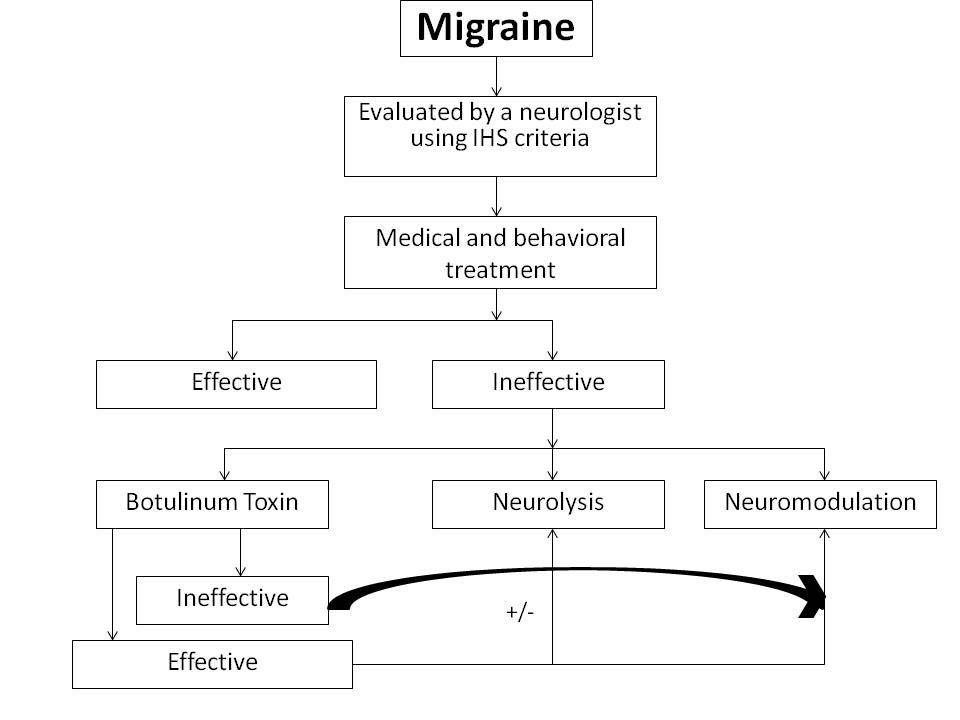
Flowchart for selecting patients for migraine surgery Contributed by Jitin Bajaj, MCh
References
Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia : an international journal of headache. 2013 Jul:33(9):629-808. doi: 10.1177/0333102413485658. Epub [PubMed PMID: 23771276]
Lipton RB, Bigal ME, Diamond M, Freitag F, Reed ML, Stewart WF, AMPP Advisory Group. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007 Jan 30:68(5):343-9 [PubMed PMID: 17261680]
Martelletti P, Katsarava Z, Lampl C, Magis D, Bendtsen L, Negro A, Russell MB, Mitsikostas DD, Jensen RH. Refractory chronic migraine: a consensus statement on clinical definition from the European Headache Federation. The journal of headache and pain. 2014 Aug 28:15(1):47. doi: 10.1186/1129-2377-15-47. Epub 2014 Aug 28 [PubMed PMID: 25169882]
Level 3 (low-level) evidenceRahmann A, Wienecke T, Hansen JM, Fahrenkrug J, Olesen J, Ashina M. Vasoactive intestinal peptide causes marked cephalic vasodilation, but does not induce migraine. Cephalalgia : an international journal of headache. 2008 Mar:28(3):226-36. doi: 10.1111/j.1468-2982.2007.01497.x. Epub [PubMed PMID: 18254893]
Level 1 (high-level) evidenceKruuse C, Thomsen LL, Birk S, Olesen J. Migraine can be induced by sildenafil without changes in middle cerebral artery diameter. Brain : a journal of neurology. 2003 Jan:126(Pt 1):241-7 [PubMed PMID: 12477710]
Level 1 (high-level) evidenceWelch KM, D'Andrea G, Tepley N, Barkley G, Ramadan NM. The concept of migraine as a state of central neuronal hyperexcitability. Neurologic clinics. 1990 Nov:8(4):817-28 [PubMed PMID: 1979655]
Welch KM, Nagesh V, Aurora SK, Gelman N. Periaqueductal gray matter dysfunction in migraine: cause or the burden of illness? Headache. 2001 Jul-Aug:41(7):629-37 [PubMed PMID: 11554950]
Parsons AA. Cortical spreading depression: its role in migraine pathogenesis and possible therapeutic intervention strategies. Current pain and headache reports. 2004 Oct:8(5):410-6 [PubMed PMID: 15361327]
Fusco M, D'Andrea G, Miccichè F, Stecca A, Bernardini D, Cananzi AL. Neurogenic inflammation in primary headaches. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2003 May:24 Suppl 2():S61-4 [PubMed PMID: 12811594]
Level 3 (low-level) evidenceStewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN. Validity of the Migraine Disability Assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain. 2000 Oct:88(1):41-52. doi: 10.1016/S0304-3959(00)00305-5. Epub [PubMed PMID: 11098098]
Ramadan NM, Schultz LL, Gilkey SJ. Migraine prophylactic drugs: proof of efficacy, utilization and cost. Cephalalgia : an international journal of headache. 1997 Apr:17(2):73-80 [PubMed PMID: 9137841]
Hepp Z, Dodick DW, Varon SF, Gillard P, Hansen RN, Devine EB. Adherence to oral migraine-preventive medications among patients with chronic migraine. Cephalalgia : an international journal of headache. 2015 May:35(6):478-88. doi: 10.1177/0333102414547138. Epub 2014 Aug 27 [PubMed PMID: 25164920]
Level 2 (mid-level) evidenceSilberstein S, Mathew N, Saper J, Jenkins S. Botulinum toxin type A as a migraine preventive treatment. For the BOTOX Migraine Clinical Research Group. Headache. 2000 Jun:40(6):445-50 [PubMed PMID: 10849039]
Level 1 (high-level) evidenceGuyuron B, Tucker T, Davis J. Surgical treatment of migraine headaches. Plastic and reconstructive surgery. 2002 Jun:109(7):2183-9 [PubMed PMID: 12045534]
Jose A, Nagori SA, Roychoudhury A. Surgical Management of Migraine Headache. The Journal of craniofacial surgery. 2018 Mar:29(2):e106-e108. doi: 10.1097/SCS.0000000000004078. Epub [PubMed PMID: 29068972]
Bovim G, Fredriksen TA, Stolt-Nielsen A, Sjaastad O. Neurolysis of the greater occipital nerve in cervicogenic headache. A follow up study. Headache. 1992 Apr:32(4):175-9 [PubMed PMID: 1582835]
Level 3 (low-level) evidenceKhan S, Schoenen J, Ashina M. Sphenopalatine ganglion neuromodulation in migraine: what is the rationale? Cephalalgia : an international journal of headache. 2014 Apr:34(5):382-91. doi: 10.1177/0333102413512032. Epub 2013 Nov 29 [PubMed PMID: 24293088]
Reed KL, Black SB, Banta CJ 2nd, Will KR. Combined occipital and supraorbital neurostimulation for the treatment of chronic migraine headaches: initial experience. Cephalalgia : an international journal of headache. 2010 Mar:30(3):260-71. doi: 10.1111/j.1468-2982.2009.01996.x. Epub 2010 Feb 15 [PubMed PMID: 19732075]
Level 3 (low-level) evidenceSchoenen J, Vandersmissen B, Jeangette S, Herroelen L, Vandenheede M, Gérard P, Magis D. Migraine prevention with a supraorbital transcutaneous stimulator: a randomized controlled trial. Neurology. 2013 Feb 19:80(8):697-704. doi: 10.1212/WNL.0b013e3182825055. Epub 2013 Feb 6 [PubMed PMID: 23390177]
Level 1 (high-level) evidenceMauskop A. Vagus nerve stimulation relieves chronic refractory migraine and cluster headaches. Cephalalgia : an international journal of headache. 2005 Feb:25(2):82-6 [PubMed PMID: 15658944]
Level 3 (low-level) evidenceHord ED, Evans MS, Mueed S, Adamolekun B, Naritoku DK. The effect of vagus nerve stimulation on migraines. The journal of pain. 2003 Nov:4(9):530-4 [PubMed PMID: 14636821]
Level 3 (low-level) evidenceChen G, You H, Juha H, Lou B, Zhong Y, Lian X, Peng Z, Xu T, Yuan L, Woralux P, Hugo AB, Jianliang C. Trigger areas nerve decompression for refractory chronic migraine. Clinical neurology and neurosurgery. 2021 Jul:206():106699. doi: 10.1016/j.clineuro.2021.106699. Epub 2021 May 20 [PubMed PMID: 34053808]
Guyuron B, Kriegler JS, Davis J, Amini SB. Comprehensive surgical treatment of migraine headaches. Plastic and reconstructive surgery. 2005 Jan:115(1):1-9 [PubMed PMID: 15622223]
Level 1 (high-level) evidenceTotonchi A, Guyuron B, Ansari H. Surgical Options for Migraine: An Overview. Neurology India. 2021 Mar-Apr:69(Supplement):S105-S109. doi: 10.4103/0028-3886.315999. Epub [PubMed PMID: 34003155]
Level 3 (low-level) evidenceScott AB. Botulinum toxin injection of eye muscles to correct strabismus. Transactions of the American Ophthalmological Society. 1981:79():734-70 [PubMed PMID: 7043872]
Level 3 (low-level) evidenceErbguth FJ, Naumann M. Historical aspects of botulinum toxin: Justinus Kerner (1786-1862) and the "sausage poison". Neurology. 1999 Nov 10:53(8):1850-3 [PubMed PMID: 10563638]
Ababneh OH, Cetinkaya A, Kulwin DR. Long-term efficacy and safety of botulinum toxin A injections to treat blepharospasm and hemifacial spasm. Clinical & experimental ophthalmology. 2014 Apr:42(3):254-61. doi: 10.1111/ceo.12165. Epub 2013 Aug 4 [PubMed PMID: 23844601]
Level 2 (mid-level) evidenceTruong D, Comella C, Fernandez HH, Ondo WG, Dysport Benign Essential Blepharospasm Study Group. Efficacy and safety of purified botulinum toxin type A (Dysport) for the treatment of benign essential blepharospasm: a randomized, placebo-controlled, phase II trial. Parkinsonism & related disorders. 2008:14(5):407-14. doi: 10.1016/j.parkreldis.2007.11.003. Epub 2008 Mar 5 [PubMed PMID: 18325821]
Level 1 (high-level) evidenceTsui JK, Eisen A, Stoessl AJ, Calne S, Calne DB. Double-blind study of botulinum toxin in spasmodic torticollis. Lancet (London, England). 1986 Aug 2:2(8501):245-7 [PubMed PMID: 2874278]
Level 1 (high-level) evidenceGreene P, Kang U, Fahn S, Brin M, Moskowitz C, Flaster E. Double-blind, placebo-controlled trial of botulinum toxin injections for the treatment of spasmodic torticollis. Neurology. 1990 Aug:40(8):1213-8 [PubMed PMID: 2199847]
Level 1 (high-level) evidenceJankovic J, Schwartz K, Donovan DT. Botulinum toxin treatment of cranial-cervical dystonia, spasmodic dysphonia, other focal dystonias and hemifacial spasm. Journal of neurology, neurosurgery, and psychiatry. 1990 Aug:53(8):633-9 [PubMed PMID: 2213039]
Brin MF, Blitzer A, Fahn S, Gould W, Lovelace RE. Adductor laryngeal dystonia (spastic dysphonia): treatment with local injections of botulinum toxin (Botox). Movement disorders : official journal of the Movement Disorder Society. 1989:4(4):287-96 [PubMed PMID: 2811888]
Brin MF, Fahn S, Moskowitz C, Friedman A, Shale HM, Greene PE, Blitzer A, List T, Lange D, Lovelace RE. Localized injections of botulinum toxin for the treatment of focal dystonia and hemifacial spasm. Movement disorders : official journal of the Movement Disorder Society. 1987:2(4):237-54 [PubMed PMID: 3504553]
Level 3 (low-level) evidenceLungu C, Karp BI, Alter K, Zolbrod R, Hallett M. Long-term follow-up of botulinum toxin therapy for focal hand dystonia: outcome at 10 years or more. Movement disorders : official journal of the Movement Disorder Society. 2011 Mar:26(4):750-3. doi: 10.1002/mds.23504. Epub 2011 Feb 1 [PubMed PMID: 21506157]
Level 2 (mid-level) evidenceSchnider P, Binder M, Auff E, Kittler H, Berger T, Wolff K. Double-blind trial of botulinum A toxin for the treatment of focal hyperhidrosis of the palms. The British journal of dermatology. 1997 Apr:136(4):548-52 [PubMed PMID: 9155956]
Level 1 (high-level) evidenceDurham PL, Cady R, Cady R. Regulation of calcitonin gene-related peptide secretion from trigeminal nerve cells by botulinum toxin type A: implications for migraine therapy. Headache. 2004 Jan:44(1):35-42; discussion 42-3 [PubMed PMID: 14979881]
Level 3 (low-level) evidenceBinder WJ, Brin MF, Blitzer A, Schoenrock LD, Pogoda JM. Botulinum toxin type A (BOTOX) for treatment of migraine headaches: an open-label study. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2000 Dec:123(6):669-76 [PubMed PMID: 11112955]
Freitag FG, Diamond S, Diamond M, Urban G. Botulinum Toxin Type A in the treatment of chronic migraine without medication overuse. Headache. 2008 Feb:48(2):201-9 [PubMed PMID: 18042229]
Level 1 (high-level) evidenceEvers S, Vollmer-Haase J, Schwaag S, Rahmann A, Husstedt IW, Frese A. Botulinum toxin A in the prophylactic treatment of migraine--a randomized, double-blind, placebo-controlled study. Cephalalgia : an international journal of headache. 2004 Oct:24(10):838-43 [PubMed PMID: 15377314]
Level 1 (high-level) evidenceAurora SK, Gawel M, Brandes JL, Pokta S, Vandenburgh AM, BOTOX North American Episodic Migraine Study Group. Botulinum toxin type a prophylactic treatment of episodic migraine: a randomized, double-blind, placebo-controlled exploratory study. Headache. 2007 Apr:47(4):486-99 [PubMed PMID: 17445098]
Level 1 (high-level) evidenceCoté TR, Mohan AK, Polder JA, Walton MK, Braun MM. Botulinum toxin type A injections: adverse events reported to the US Food and Drug Administration in therapeutic and cosmetic cases. Journal of the American Academy of Dermatology. 2005 Sep:53(3):407-15 [PubMed PMID: 16112345]
Level 2 (mid-level) evidenceJanis JE, Dhanik A, Howard JH. Validation of the peripheral trigger point theory of migraine headaches: single-surgeon experience using botulinum toxin and surgical decompression. Plastic and reconstructive surgery. 2011 Jul:128(1):123-131. doi: 10.1097/PRS.0b013e3182173d64. Epub [PubMed PMID: 21701329]
Level 2 (mid-level) evidenceGuyuron B, Varghai A, Michelow BJ, Thomas T, Davis J. Corrugator supercilii muscle resection and migraine headaches. Plastic and reconstructive surgery. 2000 Aug:106(2):429-34; discussion 435-7 [PubMed PMID: 10946944]
Popeney CA, Aló KM. Peripheral neurostimulation for the treatment of chronic, disabling transformed migraine. Headache. 2003 Apr:43(4):369-75 [PubMed PMID: 12656708]
Saper JR, Dodick DW, Silberstein SD, McCarville S, Sun M, Goadsby PJ, ONSTIM Investigators. Occipital nerve stimulation for the treatment of intractable chronic migraine headache: ONSTIM feasibility study. Cephalalgia : an international journal of headache. 2011 Feb:31(3):271-85. doi: 10.1177/0333102410381142. Epub 2010 Sep 22 [PubMed PMID: 20861241]
Level 1 (high-level) evidenceSilberstein SD, Dodick DW, Saper J, Huh B, Slavin KV, Sharan A, Reed K, Narouze S, Mogilner A, Goldstein J, Trentman T, Vaisman J, Ordia J, Weber P, Deer T, Levy R, Diaz RL, Washburn SN, Mekhail N. Safety and efficacy of peripheral nerve stimulation of the occipital nerves for the management of chronic migraine: results from a randomized, multicenter, double-blinded, controlled study. Cephalalgia : an international journal of headache. 2012 Dec:32(16):1165-79. doi: 10.1177/0333102412462642. Epub 2012 Oct 3 [PubMed PMID: 23034698]
Level 1 (high-level) evidenceMueller OM, Gaul C, Katsarava Z, Diener HC, Sure U, Gasser T. Occipital nerve stimulation for the treatment of chronic cluster headache - lessons learned from 18 months experience. Central European neurosurgery. 2011 May:72(2):84-9. doi: 10.1055/s-0030-1270476. Epub 2011 Mar 29 [PubMed PMID: 21448856]