Introduction
Kidney impairment is a worldwide public health issue with a rising incidence and prevalence, and it imparts a significant burden on the healthcare system with relatively poor outcomes.[1] Multiple myeloma is a plasma cell disorder characterized by the clonal proliferation of malignant plasma cells, producing monoclonal proteins and causing end-organ damage. It mainly affects older people and accounts for around 10% of all hematologic malignancies. Patients with multiple myeloma and other monoclonal gammopathies often have kidney dysfunction due to a wide range of associated pathologies.
The involvement of the kidney in multiple myeloma and other plasma cell dyscrasias is widespread. At the time of presentation, up to 50% of the patients have kidney involvement, which is associated with higher mortality.[2][3] Renal failure is the second most common cause of mortality in patients with multiple myeloma, second only to infections.[4]
A patient can fall anywhere on the spectrum of kidney impairment, ranging from mild and reversible acute kidney injury (AKI) to severe impairment needing hemodialysis. Some patients with multiple myeloma have a slow progression of kidney dysfunction over 6 months or more.[5][6] These patients tend to have chronic kidney disease (CKD) and can potentially need hemodialysis.
Monoclonal gammopathy-related renal disease can be classified into immunoglobulin-mediated or non-immunoglobulin–mediated, but considerable overlap and interaction between these categories can exist. In addition, the location of renal injury can be glomerular, tubulointerstitial, vascular, or a combination. Autoimmune involvement and complement activation are also common. The resulting pathophysiology includes AKI, CKD, proteinuria, hematuria, renal crystallopathy, and Fanconi syndrome.
Cast nephropathy is by far the most common renal disease associated with multiple myeloma, found in 40% to 60% of renal biopsies in patients with multiple myeloma and kidney disease. The term "myeloma kidney" usually refers to this entity.[4] However, cast nephropathy can also be found in other disorders causing renal protein overload, and the presence of cast nephropathy does not necessarily exclude other types of kidney disease secondary to monoclonal gammopathy.
Other types of kidney disease with monoclonal gammopathies are amyloidosis, monoclonal immunoglobulin deposition diseases, fibrillary glomerulonephritis, immunotactoid glomerulopathy, type I cryoglobulinemia, proliferative glomerulonephritis with monoclonal IgG deposits, C3 glomerulopathy with monoclonal gammopathy, and renal crystallopathies.[7]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Monoclonal gammopathies are characterized by the monoclonal proliferation of the lymphoplasmacytic cells in the bone marrow and monoclonal immunoglobulin (Ig) deposition in the tissues. In addition to multiple myeloma, other disorders with plasma cell clonal proliferation include Waldenstrom's macroglobulinemia, smoldering multiple myeloma, B-cell lymphocytosis, isolated plasmacytoma, low-grade chronic lymphocytic leukemia, and low-grade B-cell lymphomas (see Image. B-cell Plasma Definitions). While tumor burden may be low and not otherwise necessitate treatment, the monoclonal protein can cause pathology in the kidney, which swings the pendulum toward treatment.[7] Despite significant advances in treating multiple myeloma, the overall prognosis of renal recovery is still poor.[8][9]
Monoclonal protein (M-protein) exists in about 3% of adults older than 50 years and increases to 5% in those older than 70 years. If these patients do not meet the criteria for multiple myeloma—M-protein <3 g/dL and plasma cells on renal biopsy <10% and no other end-organ damage or multiple myeloma-defining events— the diagnosis of MGUS is made. In 2012, a classification of kidney disorders encompassing renal disorders caused by monoclonal protein (M-protein) from B-cell clones or a small plasma clone was established called "monoclonal gammopathy of renal significance." Patients in this category do not meet the diagnostic criteria for multiple myeloma or other B-cell malignancies; however, they have renal involvement, which often responds to treatment of the monoclonal protein.[10] In addition to renal pathology, excess M-protein can affect peripheral nerves and skin, leading to another recent classification of "monoclonal gammopathy of clinical significance."[10]
Proteins smaller than 15 kDa are freely filtered, and those larger than 60 kDa are restricted (in-between sizes are variably filtered).[11] Usually, carrier proteins, such as cubulin and megalin, bind to any filtered protein, transporting the protein to lysosomes to be degraded into amino acids. The amino acids are then reabsorbed through basolateral cells. Overload of any filtered protein overwhelms the transport mechanisms, and the protein causes direct tubular injury, leading to tubular cell injury and tubular necrosis. Therefore, the pathology of cast nephropathy can occasionally be seen in conditions causing significant proteinuria other than multiple myeloma. In addition, M-protein can also activate complement, causing autoimmune pathology.[10]
The underlying pathology of gammopathies is the overproduction of immunoglobulin fragments, most often light chains (κ or λ), by neoplastic plasma cells. Normally, light chains are produced at a higher rate than heavy chains and are filtered by the kidney and then degraded in the tubules; however, light chains produced by the neoplastic cells are often resistant to degradation.[4] The special characteristics of the individual light or heavy chains play a major role in determining which type of kidney injury occurs. The concentration of free light chains (FLCs) in the urine is crucial in determining renal injury. The varying amino acid composition and electrical charges of FLCs, which result in different isoelectric points, are likely contributing factors to their nephrotoxicity. The concept that not all FLCs can cause renal injury aligns with the idea that the intrinsic properties of these molecules can influence their nephrotoxic potential. It suggests that certain FLCs may have a higher propensity to cause renal damage than others.[12][13][14]
The combination of increased production and decreased degradation results in various renal disease patterns. As noted above, renal injury associated with monoclonal gammopathies can be categorized into immunoglobulin-mediated and non-immunoglobulin-mediated, although there is some overlap between these categories.
Epidemiology
Multiple myeloma is a relatively uncommon malignancy accounting for approximately 1% to 2% of all cancers and just above 17% of hematologic malignancies.[15] It has a predilection for males and is more common among people of African-American descent. Data from the US estimates an annual incidence of around 7 per 100,000 males and females annually.[16] The median age at diagnosis is between 65 and 74 years; only 2% of patients are younger than 40 years.[6] A small percentage of cases is familial, with an estimated 3 cases per 1000 patients with multiple myeloma.[17]
The prevalence of renal failure in patients with multiple myeloma varies depending on the stage of the disease and the definition used.[18] Still, it has been generally reported to affect 20% to 50% of patients with multiple myeloma, either when they are diagnosed or during their illness.[5][19][20] Impairment of kidney function in multiple myeloma leads to poor prognosis and increased mortality.[21]
Data from the United States Renal Data System (USRDS) and European Renal Association-European Dialysis and Transplant Association Registry have shown that multiple myeloma contributed to 1.5% of all cases of renal replacement therapy (RRT), and the 2-year mortality among patients with end-stage renal disease (ESRD) and multiple myeloma was 58% when compared to 31% among patients with just ESRD.[22]
Pathophysiology
Kidney involvement has been well documented in patients with plasma cell disorders secondary to the production of monoclonal immunoglobulin or its fragments, such as light or heavy chains. The various etiologies of renal disease are Ig-dependent and Ig-independent etiologies, glomerulopathies, and direct parenchymal invasion by plasma cells.
Risk factors that can predispose renal injury in patients with a history of monoclonal gammopathies include underlying chronic kidney disease (CKD), hypovolemia, electrolyte derangements (hypercalcemia, hyperuricemia), use of loop diuretics or nonsteroidal anti-inflammatory agents (NSAIDs), and administration of contrast dyes.
The combination of increased production and decreased degradation results in various renal disease patterns. As noted above, renal injury associated with monoclonal gammopathies can be categorized into immunoglobulin-mediated renal disease, immunoglobulin-mediated, and non-immunoglobulin-mediated glomerulopathies. However, there is an overlap between these categories. The most common causes of renal impairment are immunoglobulin-mediated, which will be discussed below.
Immunoglobulin-Mediated Renal Disease
Cast nephropathy is the most common kidney involvement of myeloma, in which proteinaceous casts obstruct the distal tubules and collecting ducts. Although usually found with multiple myeloma, any protein overload in the renal glomeruli and tubules can result in cast nephropathy pathology, which can be present concurrently with other types of multiple myeloma-related kidney diseases. Renal damage from cast nephropathy results both from direct nephrotoxic effects of light chains on proximal tubular cells and mechanical obstruction of distal tubules by the protein casts.[23][24]
The normal level of light chain excretion is <30 mg/day. However, excess light chain production in multiple myeloma can exceed the reabsorptive capacity, leading to increased excretion ranging from 100 mg to more than 20 g/day. Consequently, the light chains accumulate due to increased excretion of light chains, resistance to degradation, and saturation of endocytosis capacity. These light chains release proinflammatory cytokines and reactive oxygen species, causing damage to the proximal tubules and apoptosis.[25]
As the FLCs reach the distal tubules, they aggregate with uromodulin (formerly called Tamm-Horsfall mucoprotein), a protein released by the thick ascending limb of the loop of Henle. This aggregation leads to dense and obstructing intratubular casts in the distal tubules that can potentially start a giant cell reaction. This reaction leads to interstitial inflammation and fibrosis.[26][27][28][29] The result of these pathologic processes is the development and progression of interstitial fibrosis, as the obstructing casts may cause tubular rupture, further allowing the extravasation of monoclonal light chains into the interstitium.
Autopsy studies of patients with monoclonal gammopathy show that about 50% have evidence of cast nephropathy, even when the primary diagnosed renal disease is amyloidosis or crystalline podocytopathy. Tubular pH can affect cast formation depending on the M-protein characteristics. Cast nephropathy is often precipitated by radiocontrast agents, nonsteroidal anti-inflammatory drugs (NSAIDs), angiotensin-converting enzyme inhibitors (ACE-I)/angiotensin receptor blockers (ARBs), diuretics, or dehydration. Diuretics and hypovolemia are especially potent risk factors for precipitating cast nephropathy.[4][30]
The presence of light chain cast nephropathy is described as a "myeloma-defining event," and this can either be the first presentation of multiple myeloma or develop later during the course of illness.[31] Light chain cast nephropathy typically presents as AKI and progresses rapidly, with a drop in creatinine clearance observed over 1 to 3 months. However, in rare cases, kidney dysfunction gradually begins over 6 months or more. Of note, it is unusual for patients with persisting light chain cast nephropathy to have normal or stable kidney function beyond 6 months.
Amyloidosis is a systemic disorder with the extracellular accumulation of Congo red-positive fibrils in various tissues, such as skin, soft tissues, liver, kidney, heart, gastrointestinal tract, and peripheral nervous system. Cardiac involvement is an important cause of early mortality. These fibrils can have varied compositions, such as monoclonal light chains (AL), heavy chains (AH), or light and heavy chains (AHL). AL amyloidosis is the most common among these, accounting for over 94% of cases.[32] Its development indicates a poor prognosis as abnormal plasma cells produce many light chains that damage various organ systems.[33] The median survival period for AL amyloidosis is 2 to 3 years.[34] See StatPearls' companion reference, "Amyloidosis," for more information.[35]
Monoclonal immunoglobulin deposition disease (MIDD) has 3 subtypes based on the composition of the deposits: light chain deposition disease (LCDD), heavy chain deposition disease (HCDD), and light and heavy chain deposition disease (LHCDD). The difference between MIDD and amyloidosis is that the light (or heavy) chains in MIDD do not turn into fibrils, and the deposits are Congo-red negative.[26] Patients with MIDD generally present with nephrotic syndrome and kidney dysfunction.[36] Similar to AL amyloidosis, patients with MIDD generally present with albuminuria >0.5 g in 24 hours and kidney impairment, leading to ESRD if left untreated.[37]
Renal crystallopathies caused by monoclonal proteins are another cause of tubular injury and glomerulonephritis. See StatPearls' companion reference, "Calcium Deposition and Other Renal Crystal Diseases," for more information. Briefly, the primary renal crystallopathies are the following:
Light chain proximal tubulopathy is characterized by the accumulation and deposition of light chain monoclonal Igs in the proximal tubular cells, leading to proximal tubular injury and dysfunction. The light chains causing proximal tubular dysfunction are resistant to degradation by lysosomal proteases in tubular cells.[38] Consequently, there is an accumulation of these fragments within lysosomes, resulting in intracellular crystal formation. This can cause Fanconi syndrome, characterized by glucosuria, aminoaciduria, uricosuria, and phosphaturia. The proximal tubular changes can be subtle, and some patients may not develop any other clinical signs.[39][40][41]
Crystal-storing histiocytosis is an extremely rare entity associated with B-cell malignancies, such as multiple myeloma, characterized by needed-shaped crystal accumulation of monoclonal immunoglobulins in the histiocytes. These histiocytes are typically found in the bone marrow, and they can also be occasionally seen in extranodal tissues, the lungs, lymph nodes, skin, stomach, eyes, and kidneys.
Crystalglobulinemia is a rare disorder associated with paraproteinemia and multiple myeloma, as well as other malignancies. These microcrystals can cause vascular injury with thrombosis and occlusion, leading to end-organ damage.
Other rare immune-mediated paraproteinemic renal diseases: Thrombotic microangiopathy (TMA) can result from immunoglobulin-mediated endothelial damage or chemotherapy. The presence of monoclonal IgM (larger molecules than IgG) can result in hyperviscosity syndrome. Likewise, the deposition of monoclonal IgA can result in Iga vasculitis (Henoch-Schönlein purpura) or IgA nephropathy.[42][43][44]
Immune complex-mediated diseases confined to the glomerulus (glomerulonephritides)
Proliferative glomerulonephritis with monoclonal immunoglobulin deposits (PGNMID) presents with a combination of nephrotic syndrome, kidney dysfunction, and hematuria. As it is a monoclonal gammopathy-associated disease, it mimics immune-complex glomerulonephritis.[45][46] The deposits are usually IgG, are found only in the glomeruli, and consist of 1 type of heavy chain (gamma in the case of IgG) and 1 type of light chain (most often kappa). The complement system is usually activated. The affected glomeruli usually show endocapillary proliferation and membranoproliferative or membranous nephropathy.[7]
C3 glomerulopathies are very rare and characterized by complement dysregulation, resulting in C3 deposits in renal tissue with significantly fewer associated Ig deposits. M-protein acts as an autoantibody to activate C3 or C5 convertase, prolonging their normally short half-lives and activating the complement cascade. Clinically, presentations manifest as mild hematuria and proteinuria to florid glomerulonephritis.[47]
Fibrillary glomerulonephritis is primarily associated with polyclonal protein deposition but can also be associated with monoclonal protein (M-protein) deposits in the glomeruli; the underlying processes are most likely carcinoma, autoimmune disorders, and dysproteinemias. The disease is characterized by fibril structures resembling amyloidosis but without the amyloid form and Congo-red negative. The presentation includes proteinuria (usually a nephrotic range), hematuria, renal insufficiency, and hypertension. The prognosis is poor, with almost half progressing to ESRD within several years of diagnosis, despite treatment, and patients receiving a renal transplant have over a 30% rate of disease recurrence.[48]
Immunotactoid glomerulopathy is characterized by focal monoclonal deposits forming a membranoproliferative or diffuse proliferative pattern on histology. The presentation is similar to fibrillar glomerulonephritis, but the fibrils are larger. The deposits are located in microtubules of the glomerulus and arranged in parallel arrays with positive C3 staining but negative Congo-red staining.[10]
Cryoglobulinemia type I is also associated with M-protein precipitation. Type I cryoglobulinemia is characterized by precipitation of the M-protein at temperatures lower than 37 °C that redissolve when the solution is reheated. Characteristic findings are endocapillary proliferation with a membranoproliferative pattern.[10]
Non-Immunologlobulin–Mediated Diseases
Non-Ig–mediated causes of renal disease include hypercalcemia, volume depletion, sepsis, tumor lysis syndrome, medication toxicity, and plasma cell invasion of the renal parenchyma. These conditions can also exacerbate immunoglobulin-mediated diseases.
- Hypercalcemia is a common metabolic derangement in multiple myeloma, with 15% of patients having serum calcium >11 mg/dL at presentation. Moderate to severe hypercalcemia is a contributory factor in the development of AKI, as it causes renal vasoconstriction and promotes intratubular calcium deposition.[49] It also causes arginine vasopressin resistance, which leads to polyuria and volume depletion. Excess urine formation and resulting intravascular volume depletion increase the toxicity of filtered light chains.
- Nephrotoxic agents play a significant role in declining kidney function in patients with multiple myeloma. One of these agents is radiocontrast, which can potentially cause AKI.[50] Urinary light chain excretion and volume depletion are seen in almost all myeloma patients with radiocontrast-associated AKI. The contrast agent, light chains, and volume depletion can cause light chain precipitation and intratubular obstruction. Nonsteroidal anti-inflammatory drugs (NSAIDs) also cause AKI in multiple myeloma patients through similar mechanisms.[51] Other commonly used drugs for lytic lesions in patients with multiple myeloma are bisphonates. Zoledronate has been historically linked with acute tubular necrosis and pamidronate with the collapsing form of focal and segmental glomerulosclerosis.[52][53] Some drugs that are used in the management of multiple myeloma have been reported to be nephrotoxic, such as lenalidomide, bortezomib, carfilzomib, and ixazomib.
- Marked hyperuricemia (>15 mg/dL [893 micromol/L]) is present in up to 50% of patients with multiple myeloma and contributes to AKI.[54] However, raised uric acid levels as a part of tumor lysis syndrome are rare even after chemotherapy for monoclonal gammopathy.[55]
Histopathology
Cast nephropathy reveals chronic tubulointerstitial nephropathy, tubular atrophy, interstitial fibrosis, and laminated intratubular casts. This condition is characterized by dense, eosinophilic, homogeneous casts often laminated or fractured and partially surrounded by foreign body–type multinucleated giant cells. In addition, intratubular light chains may change in situ, leading to amyloid formation. Cast nephropathy begins in the collecting tubules, so biopsy samples should include some medullary tissue.[7]
Amyloidosis on light microscopy will show acellular deposits that are pinkish on hematoxylin and eosin (H&E), negative on periodic acid Schiff (PAS), and negative for silver stain. Lesions will be classically Congo-red positive and show "apple-green" birefringence under polarized light. Immunofluorescence will stain for 1 immunoglobulin component (usually κ or λ). Electron microscopy will show non-branching fibrils.[10]
Monoclonal immunoglobulin deposition disease (MIDD) shows histology dependent on the subtype—light chain, heavy chain, or mixed light and heavy chain (κ is the most common.) Light microscopy shows nodular mesangial expansion with glomerular and tubular basement membrane thickening, somewhat resembling Kimmelstiel-Wilson nodules. In contrast to amyloidosis, these tissue deposits are granular (instead of fibrillar), do not bind Congo red, and are electron-dense.[56][57]
Renal crystallopathies caused by monoclonal proteins are another cause of glomerulonephritis, although rarely, these can affect renal tubules as well. See StatPearls' companion reference, "Calcium Deposition and Other Renal Crystal Diseases," for more information. Briefly, the histopathology of renal crystallopathies includes the following:
- Light chain proximal tubulopathy is characterized by crystals that are needle-shaped, eosinophilic, stain red with mason trichrome, typically pale with PAS, and weakly birefringent on polarized microscopy. Standard immunofluorescence techniques often miss these crystals on frozen section specimens as they are inaccessible to antibody binding. These are almost always kappa light chains. Due to the loss of crystals during standard frozen sectioning, direct immunofluorescence (DIF) is not a proper method to demonstrate these structures.
- Crystalglobulinemia, a very rare disorder, is characterized by the accumulation of hypereosinophilic extracellular microcrystals of monoclonal proteins primarily within the systemic and renal microvasculature.
- Crystal-storing histiocytosis demonstrates needed-shaped crystal accumulation of monoclonal immunoglobulins in the histiocytes. These histiocytes are typically found in the bone marrow, and they can also be occasionally seen in extranodal tissues, the lungs, lymph nodes, skin, stomach, eyes, and kidneys.
C3 glomerulopathies are very rare and characterized by complement dysregulation, resulting in C3 deposits in renal tissue with no or minimal Ig deposits. The magnitude of C3 staining should be at least 2 orders greater than Ig staining. Usually, acquired autoantibodies, such as M-protein, activate C3 or C5 convertase, prolonging their normally short half-lives. Clinically, presentations manifest as mild hematuria and proteinuria to florid glomerulonephritis. Laboratory analysis shows significantly low serum C3 levels.[47]
Proliferative glomerulonephritis with monoclonal immunoglobulin deposits presents with a combination of nephrotic syndrome, kidney dysfunction, and hematuria.[46] Biopsy results show Ig deposits, usually IgG, but rarely IgA or IgM. If the complement is activated, staining for C3 and C1q can be positive. Pathology is confined to the glomerulus.[10] Light microscopy reveals membranoproliferative GN or endocapillary proliferative GN with membranous features. Immunofluorescence shows glomerular deposits staining positive for a single light chain and single heavy chain subtype. Electron microscopy in such patients shows granular, nonorganized deposits.
Fibrillary glomerulonephritis is primarily associated with polyclonal protein deposition but can also be associated with monoclonal protein (M-protein) deposits in the glomeruli. The underlying processes are most likely carcinoma, autoimmune disorders, and dysproteinemias. The disease is characterized by fibril structures resembling amyloidosis. However, these fibrils do not create the amyloid form and do not react with Congo red. Most cases show a membranoproliferative glomerulonephritis (MPGN) pattern under light microscope and IgG4, IgG1, and polyclonal LC positivity in immunofluorescence. The fibrils are non-branching and randomly oriented, similar to the amyloid fibrils, but negative for Congo-red.[48]
Immunotactoid glomerulopathy is characterized by focal monoclonal deposits forming a membranoproliferative or diffuse proliferative pattern on histology. The deposits are located in microtubules of the glomerulus and arranged in parallel arrays with positive C3 staining but negative Congo-red staining.[10]
Cryoglobulinemia type I is also associated with M-protein precipitation. Type I cryoglobulinemia is characterized by precipitation of the M-protein at temperatures lower than 37 °C that redissolve when the solution is reheated. Characteristic findings are endocapillary proliferation with a membranoproliferative pattern.[10]
History and Physical
The initial symptoms of multiple myeloma are often subtle and can include malaise, fatigue, weight loss, and bone pain. Similarly, CKD presents in a nonspecific manner as well. Thus, providers should keep plasma cell dyscrasia in the list of differentials for patients with nonspecific presenting complaints. Patients sometimes present with a fulminant syndrome of severe AKI requiring dialysis or symptomatic severe hypercalcemia and dehydration. Anemia is a characteristic feature of multiple myeloma and is present in 75% of cases; therefore, paraprotein disease should be considered in patients with kidney dysfunction and anemia.
Patients with amyloidosis or MIDD can have systemic features, such as gastrointestinal bleeding, heart failure, elevated alkaline phosphatase, cardiac arrhythmias, and periorbital purpura.[58] In such patients, blood pressure measurement can help as patients with amyloid may have hypotension with or without orthostasis as a result of coexistent myocardial and autonomic nervous system involvement. In contrast, those with MIDD and kidney dysfunction typically have hypertension.
Initial symptoms may be vague, including loss of appetite and weight, bone pain, or symptoms related to renal failure. Laboratory workup may reveal abnormal kidney function or worsening CKD, hypercalcemia, and anemia. Patients with light chain cast nephropathy usually have acute AKI or worsening CKD and proteinuria.
The proteinuria mainly involves monoclonal immunoglobulins known as Bence Jones proteins or free light chains (FLCs) in the urine. Patients with AL and MIDD can have systemic symptoms that include purpura, gastrointestinal bleeding, and heart involvement (resulting in arrhythmias or heart failure symptoms). Cardiac involvement is more common in AL. Typically, hypertension is seen in patients with cast nephropathy and MIDD due to renal failure.[59][60][61]
Evaluation
In the past, the diagnosis of myeloma kidney relied upon serum and urine protein electrophoresis with immunofixation, urinalysis, and kidney biopsy. However, with the automated immunoassay being used to quantify serum FLCs, the diagnostic protocol has changed, and there is a decreased need for kidney biopsy.[13]
The International Myeloma Working Group recommends 24-hour urine protein electrophoresis and a serum FLC assay to evaluate for cast nephropathy. In general, nephrotoxic agents, volume status, acid-base status, urinalysis with microscopic examination, and serum calcium should be reviewed.
Of note, serum electrophoresis (SPEP) often cannot detect levels of M-protein <500 mg/dL, especially if the M-protein is composed of free light chains, as these have a shorter half-life than intact immunoglobulins. One analysis found that SPEP did not detect M-protein abnormalities in over 50% of AL amyloidosis cases. Serum-free light chain assays (sFLC) use antibodies against antigens exposed to sFLC but not intact immunoglobulins and are more sensitive than SPEP. International guidelines recommend using sFLC, SPEP, and serum immunofixation instead of urinary tests, as low-level M-protein may not be detected in urine until the proximal tubular reabsorption capacity is exceeded, and 24-hour urine collections may not be accurate.[10]
The sFLC assay quantitates the concentration of circulating unbound kappa and lambda FLCs. The normal serum free kappa to lambda ratio is 0.26 to 1.65 in patients without kidney impairment. Patients with kidney impairment have high sFLC, which can be as high as 3.1 in patients with severe kidney impairment. Elevated FLCs and an abnormal kappa to lambda ratio indicate a monoclonal plasma cell disorder. The sFLC assay is more sensitive than the urine protein electrophoresis for detecting FLCs. It helps in diagnosing new cases and relapses of the disease. Light chain cast nephropathy should be strongly suspected in any patient presenting with unexplained kidney injury over fewer than 6 months and an elevated FLC level ≥1500 mg/L.[62][63]
In patients with levels of FLCs >500 mg/L, urinary albumin excretion may distinguish between other types of monoclonal gammopathies of renal significance, avoiding the need for kidney biopsy. In glomerular diseases, one expects albumin to be the predominant urine protein; however, in cast nephropathy, albumin is typically <10% of the urinary protein. Quantifying urinary light chains is also helpful as amounts <1 g/day point to causes other than cast nephropathy. One recent study observed that almost one-third of patients with multiple myeloma who underwent kidney biopsy had non-myeloma–related kidney disease.[63][64]
Cast nephropathy typically presents with proteinuria without albuminuria, as the glomerular basement membrane (GBM) remains intact. At the same time, MIDD and light chain amyloid present with significant proteinuria and albuminuria due to the involvement of the GBM.
Although there are concerns regarding the safety of kidney biopsy in patients with multiple myeloma due to presumed coagulation abnormalities, several studies indicate the procedure is generally safe, having similar rates of adverse events as encountered in the general population. Though kidney biopsy is the diagnostic test to confirm the association between a monoclonal protein and kidney disease, it can be deferred as follows:
- A presumptive diagnosis of light chain cast nephropathy can be made when multiple myeloma presents with AKI or subacute kidney injury with an sFLC concentration ≥1500 mg/L along with the predominance of monoclonal light chains in the urine by urine protein electrophoresis and immunofixation.
- A presumptive diagnosis of renal amyloidosis can be made in patients with albuminuria or nephrotic syndrome with an established diagnosis of immunoglobulin light chain AL based on a biopsy of non-kidney tissue.
- A presumptive diagnosis of light chain proximal tubulopathy can be made in patients with multiple myeloma or monoclonal gammopathy when they present with symptoms consistent with Fanconi syndrome (aminoaciduria, glycosuria in non-diabetics, hypophosphatemia, hypokalemia, hypouricemia, proteinuria).
Treatment / Management
The initial treatment of patients with myeloma-associated kidney diseases should focus on assessing the degree of renal impairment and correcting hemodynamics, volume status, and electrolyte disturbances. In addition, the formation of casts and paraprotein concentration needs to be minimized as early as possible. Most patients have some degree of renal injury, which improves with myeloma treatment. The parameters in myeloma-associated kidney disease that should be considered for correction include the following:
- Nephrotoxic agents should be discontinued, including non-steroidal anti-inflammatory agents (NSAIDs), ACE inhibitors, ARBs, and intravenous contrast.
- Patients need to be adequately hydrated. A target urine output should be approximately 100 to 150 mL/hour (about 3 L/day). It can be achieved with intravenous or oral fluid therapy unless contraindicated, such as in heart failure. Volume repletion helps avoid light chain concentration and precipitation within the tubular lumen.
- Loop diuretics can be used cautiously in patients with hypervolemia, but they should be avoided as much as possible, as they can precipitate the cast formation.
- Depending on the severity of renal impairment and the symptoms, hemodialysis may be needed to correct acid-base balance, electrolyte disturbances, volume overload, and uremic symptoms.[2][65][66] Along with extended dialysis sessions, using the dialysis cartridge to help remove the light chains has improved renal recovery.[67][68]
- Bortezomib-based anti-myeloma chemotherapy with high-dose dexamethasone should be started as early as possible to reduce the concentration of FLCs. Plasmapheresis or plasma exchange and high cut-off hemodialysis are also used to enhance the removal of toxic FLCs. (B2)
The management indicators mentioned above will be expanded on in the following sections.
Chemotherapy
About 80% of patients may recover renal function by 3 weeks if there is a reduction in the sFLC by at least 60%. This can be achieved by early diagnosis and prompt initiation of treatment. During treatment, labs must be monitored carefully for any evidence of tumor lysis syndrome characterized by hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia. The commonly used treatment regimens for multiple myeloma involve the following:
- Cyclophosphamide, bortezomib, and dexamethasone (CyBorD)
- Lenalidomide, dexamethasone (Rd)
- Lenalidomide, bortezomib, dexamethasone (RVD)
- Lenalidomide, thalidomide, dexamethasone (VTD)
The most commonly used agent is bortezomib, a proteasome inhibitor, which has a rapid onset of action and is the most studied chemotherapeutic for monoclonal gammopathies.[69] Patients with multiple myeloma associated with light chain cast nephropathy should receive chemotherapy, such as CyBorD, as quickly as possible to suppress light chain production.[70] A triplet regimen appears to be suitable for young and healthy patients, especially those with severe AKI. In older patients with comorbidities, the doublet bortezomib-dexamethasone regime is the recommended first-line treatment.[71] Bortezomib does not need renal dose adjustment, even in advanced stages of kidney failure.[72] However, the dosing of lenalidomide needs to be adjusted based on creatinine clearance.(A1)
The decision for treatment of non-multiple myeloma conditions is less clear-cut and also less well-studied due to low occurrence. The treatment of amyloidosis usually follows that of multiple myeloma due to significant morbidity and mortality. The recommendation is high-dose dexamethasone with melphalan or bortezomib-based regimens and autologous stem cell transplants in eligible patients. Given the significant complications of MGRS, similar treatment may be applicable.[7]
Extracorporeal Removal of Light Chains
The use of plasma exchange or plasmapheresis can decrease the concentration of the paraproteins. The molecular weight of the FLC is between 25 and 50 kDa. Evidence favoring the use of plasmapheresis is limited in cast nephropathy due to a large volume of distribution of light chains, resulting in a rapid rebound of light chains after the treatment.[73] (B3)
High-cutoff hemodialysis (HCO-HD) can also be used as another method of extracorporeal removal of FLCs based on their molecular weight. This technique uses a large-pore membrane hemofilter (10 nm) for repeated dialysis sessions over several weeks to remove FLCs. An in vitro study used mathematic modeling of light-chain production and metabolism and revealed that an HCO-HD membrane could remove 90% of FLCs over 3 weeks.[74] One retrospective study evaluated HCO-HD in conjunction with chemotherapy and found 63% of patients achieved dialysis independence. Albumin is lost obligatorily with HCO-HD and requires replacement.[68] One randomized controlled trial compared patients with myeloma cast nephropathy treated with bortezomib and dexamethasone, then treated with intensive dialysis and either a high-cutoff dialyzer or conventional dialyzer. The number of dialysis-independent patients was greater in the high-cutoff group, but the difference did not rise to clinical significance (possibly due to low study numbers). A key association with dialysis independence was achieving a sFLC <500 mg/dL after the first chemotherapy, which is considered the cut-off for cast formation.[51] Additional studies are required in this area.(A1)
Hypercalcemia
Use of bisphosphonates to reduce the risk of skeletal events and hypercalcemia. The most commonly used agents are pamidronate and zoledronic acid—caution in the setting of renal failure. Pamidronic acid has the potential adverse effect of focal segmental glomerulosclerosis (FSGS). In the background of reduced GFR, denosumab is preferred over bisphosphonates.
Nephrotoxic Agents
NSAIDs, ACE inhibitors, and ARBs should be discontinued. Loop diuretics and radiocontrast agents should be avoided, if possible, to prevent further kidney injury. However, novel low-osmolality contrast agents are rarely associated with developing severe AKI from light chain cast nephropathy.[51] Guidelines recommend that the risk of CIN increases when the estimated glomerular filtration rate (eGFR) falls below 45 ml/min per 1.73 m². (A1)
Transplantation
Hematopoietic stem cell transplant (HSCT) is an important and potentially curative management for patients with multiple myeloma. Although in the past, patients with significant renal dysfunction were excluded from consideration for an HSCT, several series have reported that HSCT is safe and effective in patients with kidney disease.[75] Patients younger than 70 years with an ejection fraction >45% and without active infection should be considered for HSCT.[10](B3)
The data on kidney transplantation in patients with multiple myeloma-associated kidney impairment is limited. It is an option for carefully selected patients who have had successful HSCT and have attained a hematologic stringent complete response. Also, many patients may develop acute T-cell–mediated rejection due to a commonly used chemotherapeutic agent, lenalidomide.[76] A kidney transplant can be considered if myeloma is in remission for at least 3 to 5 years. Kidney transplants can also be associated with myeloma recurrence due to immunosuppressive agents and Ig-mediated graft rejection.
Renal Replacement Therapy
Patients with ESRD can be started on renal replacement therapies, such as hemodialysis or peritoneal dialysis. As noted above, various studies have evaluated the use of high-cutoff HD for paraprotein removal.[77][78].
MGRS with IgM Monoclonal Protein
MGRS with IgM is very rare, so it is unclear what the best treatment options are. Due to their large size, IgM proteins form large multimers and are more likely to lead to hyperviscosity than other immunoglobulins. If the bone marrow clone is CD20+, rituximab-based therapy is considered first-line treatment. It can be combined with dexamethasone plus cyclophosphamide or bendamustine.[10][79] A decrease in the nephrotoxic M-protein is key to renal recovery; therefore, hematology parameters should be measured for response rates through sFLC assays or even repeat bone marrow biopsies in cases where the M-protein is difficult to measure. Renal recovery usually lags behind hematologic response (in 1 study, up to a year), so serum creatinine and urine protein may not accurately indicate treatment response.[10]
Differential Diagnosis
Patients with multiple myeloma can have 1 of the various underlying reasons for impaired kidney function. The following conditions should be kept in mind when considering the diagnosis of kidney impairment in patients with myeloma: hypercalcemia causing volume depletion, hyperviscosity syndrome, tumor lysis syndrome, and polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes syndrome (POEMS).
Prognosis
Patients with myeloma presenting with significant kidney dysfunction tend to have worse outcomes compared to those with normal renal function despite aggressive treatment.[80] Response to chemotherapy is the main predictor of survival outcomes; chemo-responsive patients have an average survival of 3 years. Recent cohort studies conducted on patients with myeloma kidney requiring dialysis with no recovery of renal function have shown a 50% survival at less than 1 year. This improves to 50% at 3 years for patients who can discontinue dialysis. Temporal trends from 2001 to 2010 in the US Renal Data System revealed that the incidence of ESRD from multiple myeloma might be declining.[81]
Patients with AKI secondary to volume depletion and due to hypercalcemia have good recovery as opposed to those with dense cast formation and tubular damage.[82] In 1 study, a higher number of casts in the cortical region was independently linked to a lower follow-up eGFR and a greater risk of remaining on dialysis.[83]
These favorable trends are attributable to increasingly effective chemotherapeutic options, such as thalidomide, lenalidomide, and bortezomib. The improvement in kidney function has been reported to be between 50% and 80% in patients with newly diagnosed myeloma managed with bortezomib.[84]
Complications
Providers treating patients with myeloma kidney should be aware of diseease complications, which include the following:
- Acute kidney injury
- Chronic kidney disease
- Hypercalcemia
- Hyperviscosity syndrome [85]
- ESRD
- Skeletal events, including fractures
- Peripheral neuropathy
Deterrence and Patient Education
- Kidney failure is a common complication of multiple myeloma. When initially diagnosed, about 20% to 50% of patients with multiple myeloma will have some degree of kidney failure.
- It can affect different kidney areas, including the glomerulus, tubules, and interstitium.
- Serum-free light chains, serum electrophoresis, urine electrophoresis, and immunofixation should be performed.
- Initial treatment should be focused on assessing the degree of renal impairment and correcting the hemodynamics, volume status, and electrolyte disturbances.
- Patients should be educated about the disease. It should be emphasized that compliance with treatment will lead to better outcomes.
Pearls and Other Issues
- Patients with light chain amyloidosis and monoclonal immunodeposition disease often have systemic involvement, including the heart and liver. Skin involvement is common with cryoglobulinemia.[10]
- Fanconi symptom is usually caused by renal crystal deposition in the proximal tubules.[7]
- Patients with MGRS have a small B-cell clones and a low level of circulating paraprotein. Therefore, serum electrophoresis may not be sufficient. More detailed investigations may be required to detect monoclonal protein, like immunofixation and serum FLC assays, especially if clinical suspicion exists.
- Fibrillary glomerulonephritis, immunotactoid glomerulonephritis, type 1 cryoglobulinemia, and crystalline light chain proximal nephropathy often require electron microscopy for differentiation.
Enhancing Healthcare Team Outcomes
Patients with monoclonal gammopathy are at high risk of renal impairment. Early identification and management of patients with monoclonal gammopathy are imperative in reducing morbidity and mortality. The care of patients with monoclonal gammopathy and renal involvement necessitates a collaborative approach among healthcare professionals to ensure patient-centered care and improve overall outcomes. Nephrologists, oncologists, emergency medicine physicians, critical care physicians, advanced practitioners, nurses, pharmacists, and other health professionals involved in the care of these patients should possess the essential clinical skills and knowledge to diagnose and manage these issues accurately. This includes expertise in recognizing the varied clinical presentations and understanding the nuances of diagnostic techniques such as SPEP, UPEP, sFLC assays, and immunofixation. Multidisciplinary teams have been shown to improve early detection and improved renal outcomes. Patient and caregiver education about common progression, adherence to treatment, and concerning signs and symptoms is crucial.
A strategic approach is equally crucial, involving evidence-based strategies to optimize treatment plans and minimize adverse effects. Ethical considerations must guide decision-making, ensuring informed consent and respecting patient autonomy in treatment choices. Each healthcare professional must be aware of their responsibilities and contribute their unique expertise to the patient's care plan, fostering a multidisciplinary approach. Effective interprofessional communication is paramount, allowing seamless information exchange and collaborative decision-making among the team members. Care coordination plays a pivotal role in ensuring that the patient's journey from diagnosis to treatment and follow-up is well-managed, minimizing errors and enhancing patient safety. Given novel chemotherapeutic agents and newer treatments, such as high-cutoff dialysis, updated literature reviews and and consultation with experts are recommended. By embracing these principles of skill, strategy, ethics, responsibilities, interprofessional communication, and care coordination, healthcare professionals can deliver patient-centered care, ultimately improving patient outcomes and enhancing team performance in the management of monoclonal gammopathy and renal involvement.
Media
(Click Image to Enlarge)
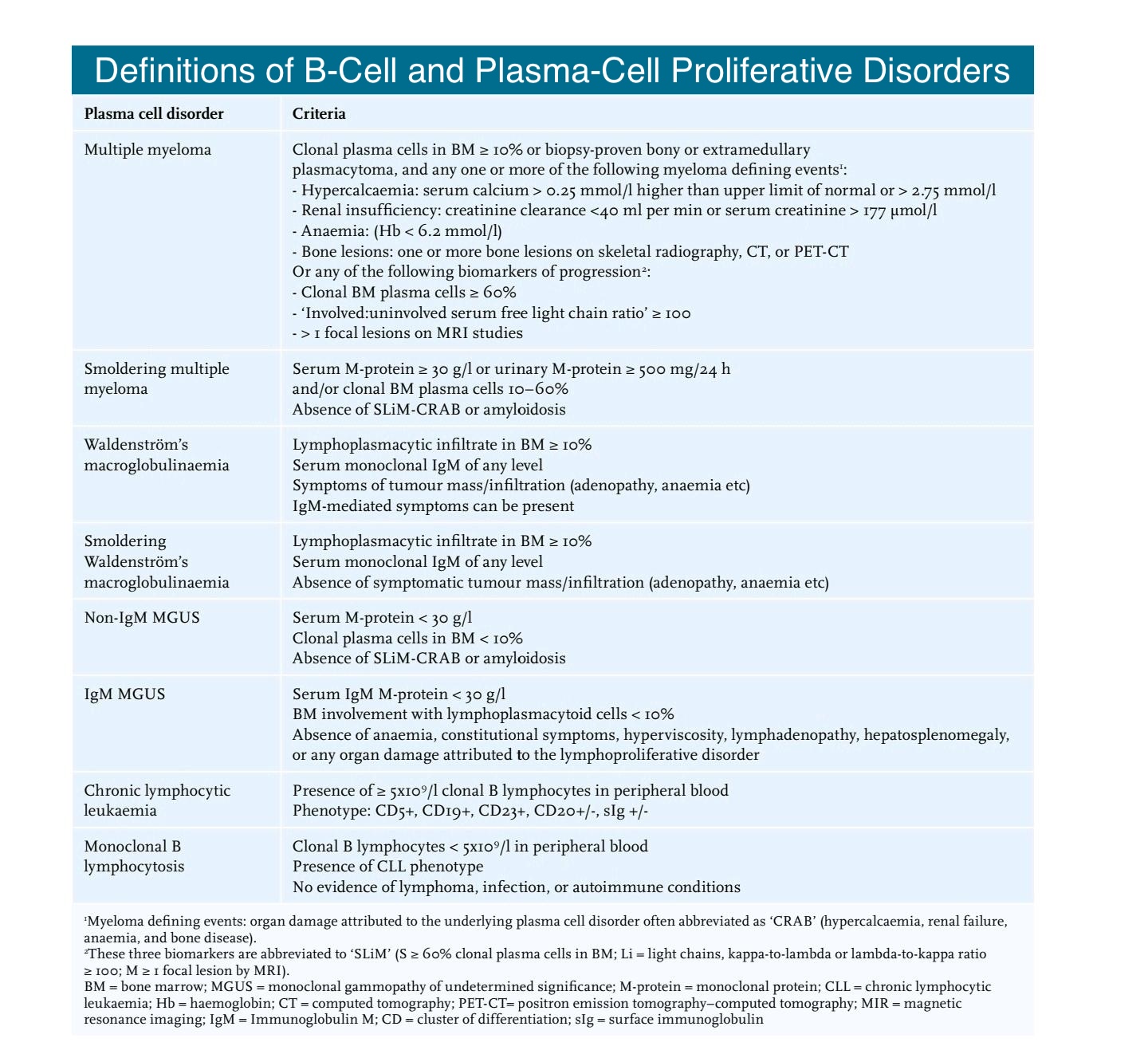
B-cell Plasma Definitions Amaador K, Peeters H, Minnema MC, et al. Monoclonal gammopathy of renal significance (MGRS) histopathologic classification, diagnostic workup, and therapeutic options. Neth J Med. 2019;77(7):243-254. PMID: 31582582.
References
Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, De Zeeuw D, Hostetter TH, Lameire N, Eknoyan G. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney international. 2005 Jun:67(6):2089-100 [PubMed PMID: 15882252]
Gödecke V, Schmidt JJ, Bräsen JH, Koenecke C, Haller H. [Diagnosis and treatment of kidney involvement in plasma cell diseases : Renal involvement in multiple myeloma and monoclonal gammopathies]. Der Internist. 2019 Jan:60(1):10-22. doi: 10.1007/s00108-018-0538-7. Epub [PubMed PMID: 30635666]
Boudhabhay I, Titah C, Talbot A, Harel S, Verine J, Touchard G, Kaaki S, Gabison E, Vasseur V, Mauget-Faÿsse M, Sené T. Multiple myeloma with crystal-storing histiocytosis, crystalline podocytopathy, and light chain proximal tubulopathy, revealed by retinal abnormalities: A case report. Medicine. 2018 Dec:97(52):e13638. doi: 10.1097/MD.0000000000013638. Epub [PubMed PMID: 30593133]
Level 3 (low-level) evidenceKorbet SM, Schwartz MM. Multiple myeloma. Journal of the American Society of Nephrology : JASN. 2006 Sep:17(9):2533-45 [PubMed PMID: 16885408]
Knudsen LM, Hjorth M, Hippe E. Renal failure in multiple myeloma: reversibility and impact on the prognosis. Nordic Myeloma Study Group. European journal of haematology. 2000 Sep:65(3):175-81 [PubMed PMID: 11007053]
Level 2 (mid-level) evidenceKyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A, Fonseca R, Rajkumar SV, Offord JR, Larson DR, Plevak ME, Therneau TM, Greipp PR. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clinic proceedings. 2003 Jan:78(1):21-33 [PubMed PMID: 12528874]
Level 2 (mid-level) evidenceMehtat Ünlü Ş, Özsan H, Sarıoğlu S. The Scope of Kidney Affection in Monoclonal Gammopathies at All Levels of Clinical Significance. Turkish journal of haematology : official journal of Turkish Society of Haematology. 2017 Dec 1:34(4):282-288. doi: 10.4274/tjh.2017.0197. Epub 2017 Aug 23 [PubMed PMID: 28832010]
Merlini G, Wechalekar AD, Palladini G. Systemic light chain amyloidosis: an update for treating physicians. Blood. 2013 Jun 27:121(26):5124-30. doi: 10.1182/blood-2013-01-453001. Epub 2013 May 13 [PubMed PMID: 23670179]
Rosenbaum C, Jasielec J, Laubach J, Paba Prada C, Richardson P, Jakubowiak AJ. Evolving strategies in the initial treatment of multiple myeloma. Seminars in oncology. 2013 Oct:40(5):592-601. doi: 10.1053/j.seminoncol.2013.08.002. Epub [PubMed PMID: 24135404]
Amaador K, Peeters H, Minnema MC, Nguyen TQ, Dendooven A, Vos JMI, Croockewit AJ, van de Donk NWCJ, Jacobs JFM, Wetzels JFM, Sprangers B, Abrahams AC. Monoclonal gammopathy of renal significance (MGRS) histopathologic classification, diagnostic workup, and therapeutic options. The Netherlands journal of medicine. 2019 Sep:77(7):243-254 [PubMed PMID: 31582582]
Jia L, Zhang L, Shao C, Song E, Sun W, Li M, Gao Y. An attempt to understand kidney's protein handling function by comparing plasma and urine proteomes. PloS one. 2009:4(4):e5146. doi: 10.1371/journal.pone.0005146. Epub 2009 Apr 20 [PubMed PMID: 19381340]
Khamlichi AA, Rocca A, Touchard G, Aucouturier P, Preud'homme JL, Cogné M. Role of light chain variable region in myeloma with light chain deposition disease: evidence from an experimental model. Blood. 1995 Nov 15:86(10):3655-9 [PubMed PMID: 7579330]
Level 3 (low-level) evidenceHutchison CA, Batuman V, Behrens J, Bridoux F, Sirac C, Dispenzieri A, Herrera GA, Lachmann H, Sanders PW, International Kidney and Monoclonal Gammopathy Research Group. The pathogenesis and diagnosis of acute kidney injury in multiple myeloma. Nature reviews. Nephrology. 2011 Nov 1:8(1):43-51. doi: 10.1038/nrneph.2011.168. Epub 2011 Nov 1 [PubMed PMID: 22045243]
Woodruff R, Sweet B. Multiple myeloma with massive Bence Jones proteinuria and preservation of renal function. Australian and New Zealand journal of medicine. 1977 Feb:7(1):60-2 [PubMed PMID: 266896]
Level 3 (low-level) evidenceSiegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA: a cancer journal for clinicians. 2023 Jan:73(1):17-48. doi: 10.3322/caac.21763. Epub [PubMed PMID: 36633525]
Kyle RA, Therneau TM, Rajkumar SV, Larson DR, Plevak MF, Melton LJ 3rd. Incidence of multiple myeloma in Olmsted County, Minnesota: Trend over 6 decades. Cancer. 2004 Dec 1:101(11):2667-74 [PubMed PMID: 15481060]
Level 2 (mid-level) evidenceVachon CM, Kyle RA, Therneau TM, Foreman BJ, Larson DR, Colby CL, Phelps TK, Dispenzieri A, Kumar SK, Katzmann JA, Rajkumar SV. Increased risk of monoclonal gammopathy in first-degree relatives of patients with multiple myeloma or monoclonal gammopathy of undetermined significance. Blood. 2009 Jul 23:114(4):785-90. doi: 10.1182/blood-2008-12-192575. Epub 2009 Jan 29 [PubMed PMID: 19179466]
Kyle RA. Multiple myeloma: review of 869 cases. Mayo Clinic proceedings. 1975 Jan:50(1):29-40 [PubMed PMID: 1110582]
Level 3 (low-level) evidenceKnudsen LM, Hippe E, Hjorth M, Holmberg E, Westin J. Renal function in newly diagnosed multiple myeloma--a demographic study of 1353 patients. The Nordic Myeloma Study Group. European journal of haematology. 1994 Oct:53(4):207-12 [PubMed PMID: 7957804]
Eleutherakis-Papaiakovou V, Bamias A, Gika D, Simeonidis A, Pouli A, Anagnostopoulos A, Michali E, Economopoulos T, Zervas K, Dimopoulos MA, Greek Myeloma Study Group. Renal failure in multiple myeloma: incidence, correlations, and prognostic significance. Leukemia & lymphoma. 2007 Feb:48(2):337-41 [PubMed PMID: 17325894]
Arellano J, Hernandez RK, Wade SW, Chen K, Pirolli M, Quach D, Quigley J, Liede A, Shahinian VB. Prevalence of renal impairment and use of nephrotoxic agents among patients with bone metastases from solid tumors in the United States. Cancer medicine. 2015 May:4(5):713-20. doi: 10.1002/cam4.403. Epub 2015 Feb 8 [PubMed PMID: 25663171]
Tsakiris DJ, Stel VS, Finne P, Fraser E, Heaf J, de Meester J, Schmaldienst S, Dekker F, Verrina E, Jager KJ. Incidence and outcome of patients starting renal replacement therapy for end-stage renal disease due to multiple myeloma or light-chain deposit disease: an ERA-EDTA Registry study. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2010 Apr:25(4):1200-6. doi: 10.1093/ndt/gfp679. Epub 2009 Dec 27 [PubMed PMID: 20037169]
Menè P, Stoppacciaro A, Lai S, Festuccia F. Light Chain Cast Nephropathy in Multiple Myeloma: Prevalence, Impact and Management Challenges. International journal of nephrology and renovascular disease. 2022:15():173-183. doi: 10.2147/IJNRD.S280179. Epub 2022 May 13 [PubMed PMID: 35592304]
Sanders PW. Pathogenesis and treatment of myeloma kidney. The Journal of laboratory and clinical medicine. 1994 Oct:124(4):484-8 [PubMed PMID: 7930873]
Sengul S, Zwizinski C, Batuman V. Role of MAPK pathways in light chain-induced cytokine production in human proximal tubule cells. American journal of physiology. Renal physiology. 2003 Jun:284(6):F1245-54 [PubMed PMID: 12582006]
Dimopoulos MA, Kastritis E, Rosinol L, Bladé J, Ludwig H. Pathogenesis and treatment of renal failure in multiple myeloma. Leukemia. 2008 Aug:22(8):1485-93. doi: 10.1038/leu.2008.131. Epub 2008 Jun 5 [PubMed PMID: 18528426]
Herrera GA, Sanders PW. Paraproteinemic renal diseases that involve the tubulo-interstitium. Contributions to nephrology. 2007:153():105-15 [PubMed PMID: 17075226]
Sanders PW, Booker BB. Pathobiology of cast nephropathy from human Bence Jones proteins. The Journal of clinical investigation. 1992 Feb:89(2):630-9 [PubMed PMID: 1737851]
Level 3 (low-level) evidenceHuang ZQ, Sanders PW. Localization of a single binding site for immunoglobulin light chains on human Tamm-Horsfall glycoprotein. The Journal of clinical investigation. 1997 Feb 15:99(4):732-6 [PubMed PMID: 9045877]
Salahuddin AZ, Alam MR, Hossain RM, Feroz S, Zannat H, Mondal MC, Roy AS, Robbani MG, Uddin MB, Kadir MS. Renal Involvement as a Presenting Feature of Multiple Myeloma. Mymensingh medical journal : MMJ. 2019 Jul:28(3):527-535 [PubMed PMID: 31391422]
Leung N, Rajkumar SV. Multiple myeloma with acute light chain cast nephropathy. Blood cancer journal. 2023 Mar 29:13(1):46. doi: 10.1038/s41408-023-00806-w. Epub 2023 Mar 29 [PubMed PMID: 36990996]
Said SM, Sethi S, Valeri AM, Leung N, Cornell LD, Fidler ME, Herrera Hernandez L, Vrana JA, Theis JD, Quint PS, Dogan A, Nasr SH. Renal amyloidosis: origin and clinicopathologic correlations of 474 recent cases. Clinical journal of the American Society of Nephrology : CJASN. 2013 Sep:8(9):1515-23. doi: 10.2215/CJN.10491012. Epub 2013 May 23 [PubMed PMID: 23704299]
Level 3 (low-level) evidenceRyšavá R. AL amyloidosis: advances in diagnostics and treatment. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2019 Sep 1:34(9):1460-1466. doi: 10.1093/ndt/gfy291. Epub [PubMed PMID: 30299492]
Level 3 (low-level) evidenceVela-Ojeda J, García-Ruiz Esparza MA, Padilla-González Y, Sánchez-Cortes E, García-Chávez J, Montiel-Cervantes L, Reyes-Maldonado E, Majluf-Cruz A, Mayani H. Multiple myeloma-associated amyloidosis is an independent high-risk prognostic factor. Annals of hematology. 2009 Jan:88(1):59-66. doi: 10.1007/s00277-008-0554-0. Epub 2008 Jul 22 [PubMed PMID: 18648809]
Bustamante JG, Zaidi SRH. Amyloidosis. StatPearls. 2024 Jan:(): [PubMed PMID: 29261990]
Nasr SH, Valeri AM, Cornell LD, Fidler ME, Sethi S, D'Agati VD, Leung N. Renal monoclonal immunoglobulin deposition disease: a report of 64 patients from a single institution. Clinical journal of the American Society of Nephrology : CJASN. 2012 Feb:7(2):231-9. doi: 10.2215/CJN.08640811. Epub 2011 Dec 8 [PubMed PMID: 22156754]
Level 2 (mid-level) evidenceAngel-Korman A, Stern L, Angel Y, Sarosiek S, Menn-Josephy H, Francis J, Ghai S, Sloan JM, Sanchorawala V, Havasi A. The Role of Kidney Transplantation in Monoclonal Ig Deposition Disease. Kidney international reports. 2020 Apr:5(4):485-493. doi: 10.1016/j.ekir.2020.01.011. Epub 2020 Mar 9 [PubMed PMID: 32274452]
Leboulleux M, Lelongt B, Mougenot B, Touchard G, Makdassi R, Rocca A, Noel LH, Ronco PM, Aucouturier P. Protease resistance and binding of Ig light chains in myeloma-associated tubulopathies. Kidney international. 1995 Jul:48(1):72-9 [PubMed PMID: 7564094]
Stokes MB, Valeri AM, Herlitz L, Khan AM, Siegel DS, Markowitz GS, D'Agati VD. Light Chain Proximal Tubulopathy: Clinical and Pathologic Characteristics in the Modern Treatment Era. Journal of the American Society of Nephrology : JASN. 2016 May:27(5):1555-65. doi: 10.1681/ASN.2015020185. Epub 2015 Sep 15 [PubMed PMID: 26374607]
Vignon M, Javaugue V, Alexander MP, El-Karoui K, Karras A, Roos-Weil D, Royer B, Asli B, Knebelmann B, Touchard G, Jaccard A, Arnulf B, Bridoux F, Leung N, Fermand JP. Current anti-myeloma therapies in renal manifestations of monoclonal light chain-associated Fanconi syndrome: a retrospective series of 49 patients. Leukemia. 2017 Jan:31(1):123-129. doi: 10.1038/leu.2016.195. Epub 2016 Jul 20 [PubMed PMID: 27435002]
Level 2 (mid-level) evidenceLuciani A, Sirac C, Terryn S, Javaugue V, Prange JA, Bender S, Bonaud A, Cogné M, Aucouturier P, Ronco P, Bridoux F, Devuyst O. Impaired Lysosomal Function Underlies Monoclonal Light Chain-Associated Renal Fanconi Syndrome. Journal of the American Society of Nephrology : JASN. 2016 Jul:27(7):2049-61. doi: 10.1681/ASN.2015050581. Epub 2015 Nov 27 [PubMed PMID: 26614382]
Daidola G, Guarena C, Brustia M, Leonardi G, Vigotti FN, Marciello A, Bianco S, Chiarinotti D, Saltarelli M, Besso L, Biancone L. [Efficacy of SUPRA HFR in the treatment of acute renal damage during multiple myeloma]. Giornale italiano di nefrologia : organo ufficiale della Societa italiana di nefrologia. 2018 Dec:35(6):. pii: 2018-vol6. Epub [PubMed PMID: 30550040]
Favà A, Fulladosa X, Montero N, Draibe J, Torras J, Gomà M, Cruzado JM. Treatment of multiple myeloma with renal involvement: the nephrologist's view. Clinical kidney journal. 2018 Dec:11(6):777-785. doi: 10.1093/ckj/sfy065. Epub 2018 Aug 1 [PubMed PMID: 30524711]
Burwick N, Adams SV, Todd-Stenberg JA, Burrows NR, Pavkov ME, O'Hare AM. Association of Monoclonal Gammopathy with Progression to ESKD among US Veterans. Clinical journal of the American Society of Nephrology : CJASN. 2018 Dec 7:13(12):1810-1815. doi: 10.2215/CJN.06210518. Epub 2018 Nov 15 [PubMed PMID: 30442867]
Bridoux F, Javaugue V, Nasr SH, Leung N. Proliferative glomerulonephritis with monoclonal immunoglobulin deposits: a nephrologist perspective. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2021 Jan 25:36(2):208-215. doi: 10.1093/ndt/gfz176. Epub [PubMed PMID: 33494099]
Level 3 (low-level) evidenceNasr SH, Satoskar A, Markowitz GS, Valeri AM, Appel GB, Stokes MB, Nadasdy T, D'Agati VD. Proliferative glomerulonephritis with monoclonal IgG deposits. Journal of the American Society of Nephrology : JASN. 2009 Sep:20(9):2055-64. doi: 10.1681/ASN.2009010110. Epub 2009 May 21 [PubMed PMID: 19470674]
Level 2 (mid-level) evidenceSmith RJH, Appel GB, Blom AM, Cook HT, D'Agati VD, Fakhouri F, Fremeaux-Bacchi V, Józsi M, Kavanagh D, Lambris JD, Noris M, Pickering MC, Remuzzi G, de Córdoba SR, Sethi S, Van der Vlag J, Zipfel PF, Nester CM. C3 glomerulopathy - understanding a rare complement-driven renal disease. Nature reviews. Nephrology. 2019 Mar:15(3):129-143. doi: 10.1038/s41581-018-0107-2. Epub [PubMed PMID: 30692664]
Level 3 (low-level) evidenceNasr SH, Valeri AM, Cornell LD, Fidler ME, Sethi S, Leung N, Fervenza FC. Fibrillary glomerulonephritis: a report of 66 cases from a single institution. Clinical journal of the American Society of Nephrology : CJASN. 2011 Apr:6(4):775-84. doi: 10.2215/CJN.08300910. Epub 2011 Mar 24 [PubMed PMID: 21441134]
Level 3 (low-level) evidenceSmolens P, Barnes JL, Kreisberg R. Hypercalcemia can potentiate the nephrotoxicity of Bence Jones proteins. The Journal of laboratory and clinical medicine. 1987 Oct:110(4):460-5 [PubMed PMID: 3655525]
Level 3 (low-level) evidenceMcCarthy CS, Becker JA. Multiple myeloma and contrast media. Radiology. 1992 May:183(2):519-21 [PubMed PMID: 1561361]
Bridoux F, Carron PL, Pegourie B, Alamartine E, Augeul-Meunier K, Karras A, Joly B, Peraldi MN, Arnulf B, Vigneau C, Lamy T, Wynckel A, Kolb B, Royer B, Rabot N, Benboubker L, Combe C, Jaccard A, Moulin B, Knebelmann B, Chevret S, Fermand JP, MYRE Study Group. Effect of High-Cutoff Hemodialysis vs Conventional Hemodialysis on Hemodialysis Independence Among Patients With Myeloma Cast Nephropathy: A Randomized Clinical Trial. JAMA. 2017 Dec 5:318(21):2099-2110. doi: 10.1001/jama.2017.17924. Epub [PubMed PMID: 29209721]
Level 1 (high-level) evidenceYachoui R. Early onset acute tubular necrosis following single infusion of zoledronate. Clinical cases in mineral and bone metabolism : the official journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases. 2016 May-Aug:13(2):154-156 [PubMed PMID: 27920815]
Level 3 (low-level) evidencede Roij van Zuijdewijn C, van Dorp W, Florquin S, Roelofs J, Verburgh K. Bisphosphonate nephropathy: A case series and review of the literature. British journal of clinical pharmacology. 2021 Sep:87(9):3485-3491. doi: 10.1111/bcp.14780. Epub 2021 Mar 4 [PubMed PMID: 33595131]
Level 2 (mid-level) evidenceHussain A, Almenfi HF, Almehdewi AM, Hamza MS, Bhat MS, Vijayashankar NP. Laboratory Features of Newly Diagnosed Multiple Myeloma Patients. Cureus. 2019 May 22:11(5):e4716. doi: 10.7759/cureus.4716. Epub 2019 May 22 [PubMed PMID: 31355076]
Leung N, Behrens J. Current approach to diagnosis and management of acute renal failure in myeloma patients. Advances in chronic kidney disease. 2012 Sep:19(5):297-302. doi: 10.1053/j.ackd.2012.06.001. Epub [PubMed PMID: 22920640]
Level 3 (low-level) evidenceCampo E, Jaffe ES, Cook JR, Quintanilla-Martinez L, Swerdlow SH, Anderson KC, Brousset P, Cerroni L, de Leval L, Dirnhofer S, Dogan A, Feldman AL, Fend F, Friedberg JW, Gaulard P, Ghia P, Horwitz SM, King RL, Salles G, San-Miguel J, Seymour JF, Treon SP, Vose JM, Zucca E, Advani R, Ansell S, Au WY, Barrionuevo C, Bergsagel L, Chan WC, Cohen JI, d'Amore F, Davies A, Falini B, Ghobrial IM, Goodlad JR, Gribben JG, Hsi ED, Kahl BS, Kim WS, Kumar S, LaCasce AS, Laurent C, Lenz G, Leonard JP, Link MP, Lopez-Guillermo A, Mateos MV, Macintyre E, Melnick AM, Morschhauser F, Nakamura S, Narbaitz M, Pavlovsky A, Pileri SA, Piris M, Pro B, Rajkumar V, Rosen ST, Sander B, Sehn L, Shipp MA, Smith SM, Staudt LM, Thieblemont C, Tousseyn T, Wilson WH, Yoshino T, Zinzani PL, Dreyling M, Scott DW, Winter JN, Zelenetz AD. The International Consensus Classification of Mature Lymphoid Neoplasms: a report from the Clinical Advisory Committee. Blood. 2022 Sep 15:140(11):1229-1253. doi: 10.1182/blood.2022015851. Epub [PubMed PMID: 35653592]
Level 3 (low-level) evidenceAlaggio R, Amador C, Anagnostopoulos I, Attygalle AD, Araujo IBO, Berti E, Bhagat G, Borges AM, Boyer D, Calaminici M, Chadburn A, Chan JKC, Cheuk W, Chng WJ, Choi JK, Chuang SS, Coupland SE, Czader M, Dave SS, de Jong D, Du MQ, Elenitoba-Johnson KS, Ferry J, Geyer J, Gratzinger D, Guitart J, Gujral S, Harris M, Harrison CJ, Hartmann S, Hochhaus A, Jansen PM, Karube K, Kempf W, Khoury J, Kimura H, Klapper W, Kovach AE, Kumar S, Lazar AJ, Lazzi S, Leoncini L, Leung N, Leventaki V, Li XQ, Lim MS, Liu WP, Louissaint A Jr, Marcogliese A, Medeiros LJ, Michal M, Miranda RN, Mitteldorf C, Montes-Moreno S, Morice W, Nardi V, Naresh KN, Natkunam Y, Ng SB, Oschlies I, Ott G, Parrens M, Pulitzer M, Rajkumar SV, Rawstron AC, Rech K, Rosenwald A, Said J, Sarkozy C, Sayed S, Saygin C, Schuh A, Sewell W, Siebert R, Sohani AR, Tooze R, Traverse-Glehen A, Vega F, Vergier B, Wechalekar AD, Wood B, Xerri L, Xiao W. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. 2022 Jul:36(7):1720-1748. doi: 10.1038/s41375-022-01620-2. Epub 2022 Jun 22 [PubMed PMID: 35732829]
Pozzi C, D'Amico M, Fogazzi GB, Curioni S, Ferrario F, Pasquali S, Quattrocchio G, Rollino C, Segagni S, Locatelli F. Light chain deposition disease with renal involvement: clinical characteristics and prognostic factors. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2003 Dec:42(6):1154-63 [PubMed PMID: 14655186]
Level 2 (mid-level) evidenceKitchlu A, McArthur E, Amir E, Booth CM, Sutradhar R, Majeed H, Nash DM, Silver SA, Garg AX, Chan CT, Kim SJ, Wald R. Acute Kidney Injury in Patients Receiving Systemic Treatment for Cancer: A Population-Based Cohort Study. Journal of the National Cancer Institute. 2019 Jul 1:111(7):727-736. doi: 10.1093/jnci/djy167. Epub [PubMed PMID: 30423160]
Takano J, Mine S, Mochizuki M, Tanaka N, Hagiwara S. Late-stage myeloma invades kidney without significant effect on renal function: findings from 53 autopsies in a single institute. International journal of hematology. 2019 Feb:109(2):147-153. doi: 10.1007/s12185-018-2546-8. Epub 2018 Oct 16 [PubMed PMID: 30327925]
Huskey JL, Heilman RL, Khamash H, Fonseca R. Kidney Transplant in the Era of Modern Therapy for Multiple Myeloma. Transplantation. 2018 Dec:102(12):1994-2001. doi: 10.1097/TP.0000000000002449. Epub [PubMed PMID: 30211830]
Leung N, Gertz MA, Zeldenrust SR, Rajkumar SV, Dispenzieri A, Fervenza FC, Kumar S, Lacy MQ, Lust JA, Greipp PR, Witzig TE, Hayman SR, Russell SJ, Kyle RA, Winters JL. Improvement of cast nephropathy with plasma exchange depends on the diagnosis and on reduction of serum free light chains. Kidney international. 2008 Jun:73(11):1282-8. doi: 10.1038/ki.2008.108. Epub 2008 Apr 2 [PubMed PMID: 18385667]
Level 2 (mid-level) evidenceLeung N, Gertz M, Kyle RA, Fervenza FC, Irazabal MV, Eirin A, Kumar S, Cha SS, Rajkumar SV, Lacy MQ, Zeldenrust SR, Buadi FK, Hayman SR, Nasr SH, Sethi S, Ramirez-Alvarado M, Witzig TE, Herrmann SM, Dispenzieri A. Urinary albumin excretion patterns of patients with cast nephropathy and other monoclonal gammopathy-related kidney diseases. Clinical journal of the American Society of Nephrology : CJASN. 2012 Dec:7(12):1964-8. doi: 10.2215/CJN.11161111. Epub 2012 Sep 27 [PubMed PMID: 23024162]
Nasr SH, Valeri AM, Sethi S, Fidler ME, Cornell LD, Gertz MA, Lacy M, Dispenzieri A, Rajkumar SV, Kyle RA, Leung N. Clinicopathologic correlations in multiple myeloma: a case series of 190 patients with kidney biopsies. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2012 Jun:59(6):786-94. doi: 10.1053/j.ajkd.2011.12.028. Epub 2012 Mar 13 [PubMed PMID: 22417785]
Level 2 (mid-level) evidenceRenal Impairment of Multiple Myeloma Collaborative Study Group. [Expert consensus for the diagnosis and treatment of patients with renal impairment of multiple myeloma]. Zhonghua nei ke za zhi. 2017 Nov 1:56(11):871-875. doi: 10.3760/cma.j.issn.0578-1426.2017.11.022. Epub [PubMed PMID: 29136724]
Level 3 (low-level) evidenceChinese Hematology Association, Chinese Society of Hematology, Chinese Myeloma Committee-Chinese Hematology Association. [The guidelines for the diagnosis and management of multiple myeloma in China (2017 revision)]. Zhonghua nei ke za zhi. 2017 Nov 1:56(11):866-870. doi: 10.3760/cma.j.issn.0578-1426.2017.11.021. Epub [PubMed PMID: 29136723]
Hutchison CA, Cockwell P, Stringer S, Bradwell A, Cook M, Gertz MA, Dispenzieri A, Winters JL, Kumar S, Rajkumar SV, Kyle RA, Leung N. Early reduction of serum-free light chains associates with renal recovery in myeloma kidney. Journal of the American Society of Nephrology : JASN. 2011 Jun:22(6):1129-36. doi: 10.1681/ASN.2010080857. Epub 2011 Apr 21 [PubMed PMID: 21511832]
Level 2 (mid-level) evidenceHutchison CA, Heyne N, Airia P, Schindler R, Zickler D, Cook M, Cockwell P, Grima D. Immunoglobulin free light chain levels and recovery from myeloma kidney on treatment with chemotherapy and high cut-off haemodialysis. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2012 Oct:27(10):3823-8. doi: 10.1093/ndt/gfr773. Epub 2012 Jan 23 [PubMed PMID: 22273664]
Dimopoulos MA, Roussou M, Gkotzamanidou M, Nikitas N, Psimenou E, Mparmparoussi D, Matsouka C, Spyropoulou-Vlachou M, Terpos E, Kastritis E. The role of novel agents on the reversibility of renal impairment in newly diagnosed symptomatic patients with multiple myeloma. Leukemia. 2013 Feb:27(2):423-9. doi: 10.1038/leu.2012.182. Epub 2012 Jul 5 [PubMed PMID: 22763386]
Sonneveld P, Schmidt-Wolf IG, van der Holt B, El Jarari L, Bertsch U, Salwender H, Zweegman S, Vellenga E, Broyl A, Blau IW, Weisel KC, Wittebol S, Bos GM, Stevens-Kroef M, Scheid C, Pfreundschuh M, Hose D, Jauch A, van der Velde H, Raymakers R, Schaafsma MR, Kersten MJ, van Marwijk-Kooy M, Duehrsen U, Lindemann W, Wijermans PW, Lokhorst HM, Goldschmidt HM. Bortezomib induction and maintenance treatment in patients with newly diagnosed multiple myeloma: results of the randomized phase III HOVON-65/ GMMG-HD4 trial. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2012 Aug 20:30(24):2946-55. doi: 10.1200/JCO.2011.39.6820. Epub 2012 Jul 16 [PubMed PMID: 22802322]
Level 1 (high-level) evidenceBridoux F, Arnulf B, Karlin L, Blin N, Rabot N, Macro M, Audard V, Belhadj K, Pegourie B, Gobert P, Cornec Le Gall E, Joly B, Karras A, Jaccard A, Augeul-Meunier K, Manier S, Royer B, Caillot D, Tiab M, Delbes S, Suarez F, Vigneau C, Caillard S, Arakelyan-Laboure N, Roos-Weil D, Chevret S, Fermand JP, MYRE study group. Randomized Trial Comparing Double Versus Triple Bortezomib-Based Regimen in Patients With Multiple Myeloma and Acute Kidney Injury Due to Cast Nephropathy. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2020 Aug 10:38(23):2647-2657. doi: 10.1200/JCO.20.00298. Epub 2020 Jun 23 [PubMed PMID: 32574117]
Level 1 (high-level) evidenceDimopoulos MA, Roussou M, Gavriatopoulou M, Psimenou E, Eleutherakis-Papaiakovou E, Migkou M, Matsouka C, Mparmparousi D, Gika D, Kafantari E, Ziogas D, Fotiou D, Panagiotidis I, Terpos E, Kastritis E. Bortezomib-based triplets are associated with a high probability of dialysis independence and rapid renal recovery in newly diagnosed myeloma patients with severe renal failure or those requiring dialysis. American journal of hematology. 2016 May:91(5):499-502. doi: 10.1002/ajh.24335. Epub 2016 Apr 4 [PubMed PMID: 26890495]
Cserti C, Haspel R, Stowell C, Dzik W. Light-chain removal by plasmapheresis in myeloma-associated renal failure. Transfusion. 2007 Mar:47(3):511-4 [PubMed PMID: 17319833]
Level 3 (low-level) evidenceHutchison CA, Cockwell P, Reid S, Chandler K, Mead GP, Harrison J, Hattersley J, Evans ND, Chappell MJ, Cook M, Goehl H, Storr M, Bradwell AR. Efficient removal of immunoglobulin free light chains by hemodialysis for multiple myeloma: in vitro and in vivo studies. Journal of the American Society of Nephrology : JASN. 2007 Mar:18(3):886-95 [PubMed PMID: 17229909]
Parikh GC, Amjad AI, Saliba RM, Kazmi SM, Khan ZU, Lahoti A, Hosing C, Mendoza F, Qureshi SR, Weber DM, Wang M, Popat U, Alousi AM, Champlin RE, Giralt SA, Qazilbash MH. Autologous hematopoietic stem cell transplantation may reverse renal failure in patients with multiple myeloma. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation. 2009 Jul:15(7):812-6. doi: 10.1016/j.bbmt.2009.03.021. Epub [PubMed PMID: 19539212]
Level 3 (low-level) evidenceLum EL, Huang E, Bunnapradist S, Pham T, Danovitch G. Acute Kidney Allograft Rejection Precipitated by Lenalidomide Treatment for Multiple Myeloma. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2017 May:69(5):701-704. doi: 10.1053/j.ajkd.2016.11.024. Epub 2017 Feb 9 [PubMed PMID: 28189378]
Oortgiesen BE, Azad R, Hemmelder MH, Kibbelaar RE, Veeger NJGM, de Vries JC, van Roon EN, Hoogendoorn M. The impact of the introduction of bortezomib on dialysis independence in multiple myeloma patients with renal impairment: a nationwide Dutch population-based study. Haematologica. 2018 Jul:103(7):e311-e314. doi: 10.3324/haematol.2017.184754. Epub 2018 Mar 15 [PubMed PMID: 29545339]
Dimopoulos MA, Roussou M, Gavriatopoulou M, Fotiou D, Ziogas DC, Migkou M, Panagiotidis I, Eleutherakis-Papaiakovou E, Kanellias N, Psimenou E, Marinaki S, Bacharaki D, Mparmparoussi D, Matsouka C, Giannouli S, Terpos E, Kastritis E. Outcomes of newly diagnosed myeloma patients requiring dialysis: renal recovery, importance of rapid response and survival benefit. Blood cancer journal. 2017 Jun 16:7(6):e571. doi: 10.1038/bcj.2017.49. Epub 2017 Jun 16 [PubMed PMID: 28622304]
Girard LP, Soekojo CY, Ooi M, Chng WJ, de Mel S. Immunoglobulin M Monoclonal Gammopathies of Clinical Significance. Frontiers in oncology. 2022:12():905484. doi: 10.3389/fonc.2022.905484. Epub 2022 Jun 9 [PubMed PMID: 35756635]
Chow CC, Mo KL, Chan CK, Lo HK, Wong KS, Chan JC. Renal impairment in patients with multiple myeloma. Hong Kong medical journal = Xianggang yi xue za zhi. 2003 Apr:9(2):78-82 [PubMed PMID: 12668816]
Level 2 (mid-level) evidenceReule S, Sexton DJ, Solid CA, Chen SC, Foley RN. ESRD due to Multiple Myeloma in the United States, 2001-2010. Journal of the American Society of Nephrology : JASN. 2016 May:27(5):1487-94. doi: 10.1681/ASN.2014090876. Epub 2015 Oct 29 [PubMed PMID: 26516209]
Alexanian R, Barlogie B, Dixon D. Renal failure in multiple myeloma. Pathogenesis and prognostic implications. Archives of internal medicine. 1990 Aug:150(8):1693-5 [PubMed PMID: 2383164]
Ecotière L, Thierry A, Debiais-Delpech C, Chevret S, Javaugue V, Desport E, Belmouaz S, Quellard N, Kaaki S, Michel Goujon J, Fermand JP, Touchard G, Bridoux F. Prognostic value of kidney biopsy in myeloma cast nephropathy: a retrospective study of 70 patients. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2016 May:31(5):850. doi: 10.1093/ndt/gfw056. Epub 2016 Mar 10 [PubMed PMID: 26968198]
Level 2 (mid-level) evidenceUchida M, Kamata K, Okubo M. Renal dysfunction in multiple myeloma. Internal medicine (Tokyo, Japan). 1995 May:34(5):364-70 [PubMed PMID: 7647403]
Level 2 (mid-level) evidenceKopp WL, Beirne GJ, Burns RO. Hyperviscosity syndrome in multiple myeloma. The American journal of medicine. 1967 Jul:43(1):141-6 [PubMed PMID: 4951414]
Level 3 (low-level) evidence