Introduction
The treatment of rectal trauma has undergone a significant evolution over the past 80 years. Most of these changes have paralleled the history of wartime conflict. During World War II, Sir William H. Ogilvie, who was the Consultant Surgeon to the East African Force in 1941, mandated that all colorectal wounds be managed by exteriorization.[1][2][3] This remained dogma in post - world war civilian surgery. During the Vietnam conflict, pre-sacral drainage and distal rectal washout were popularized, completing the four D's dogma (debridement, diversion, drainage, and distal rectal washout.)
In 1979 Stone and Fabian published the first randomized prospective trial comparing primary repair and diversion; this marked the evolution of the management of colorectal injuries. Over the next two decades, multiple studies reinforced that primary repair or resection and anastomosis was the standard of care for most colorectal injuries, and extraperitoneal rectal injuries should have management with selective fecal diversion.
In 1994 a study by Stewart et al. looked retrospectively at patients with destructive wounds of the colon. They found a 14% leak rate with primary anastomosis. With sub-analysis, patients with underlying chronic illness and requiring greater than four units of packed red blood cells within 24 hours had a leak rate of 42%, and a third of the leaks died.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The majority of rectal injuries are secondary to penetrating trauma, excluding iatrogenic, sex-related, and foreign body injuries. Gunshot wounds compose 85 to 90% and stab wounds approximately 5%. Approximately 5 to 10% are secondary to blunt trauma of which 1 to 2% are associated with pelvic fractures, most specifically anterior-posterior compression.[4][5][6][7]
Epidemiology
The incidence of rectal trauma in civilian trauma centers is 1 to 3%, and in recent military conflict, up to 5%. The military rectal wounds involve much higher velocity weaponry, blast injuries, fragmentations, and burns.[8]
Pathophysiology
The rectum is approximately 15cm long. It has an intraperitoneal portion, which includes the upper two-thirds anteriorly and the upper one third laterally. The lower third of the rectum is extraperitoneal. The blood supply is from the superior hemorrhoidal branches from the inferior mesenteric artery, the middle hemorrhoidal branch of the internal iliac artery, and the inferior hemorrhoidal branch of the internal pudendal arteries.
Decision making for management of rectal injuries has as its basis intraperitoneal and extra-peritoneal zones and the Rectum Injury Scale of the American Association for the Surgery of Trauma (image attached below).[9]
History and Physical
In the trauma patient, a systemic approach of the entire patient must be conducted, without exception, as outlined by the Advanced Trauma Life Support (ATLS) Program. An initial assessment of the patient is of utmost importance before focusing on the specific anatomic regions of obvious traumatic injury. The concept of this initial assessment, as outlined by the ATLS, includes a systematic evaluation including a primary survey, resuscitation, and detailed secondary survey with continuous re-evaluation through all steps.
The primary survey is designed to identify immediate life-threatening injuries quickly. Therefore, the universal approach has been established by the ATLS to follow the following in specific order: airway maintenance, breathing (ventilation), circulation (including hemorrhage control), disability (neurologic status), and exposure. Airway assessment and management have the highest priority of any injured patient irrespective of mechanism or wound location.[10] This cannot be overemphasized, to first secure or ensure a patent airway, before proceeding methodically, in appropriate order through the ATLS protocol.
During the primary survey, complete exposure of the patient is essential, as is to roll the patient potentially to both sides, as to not overlook penetrating injuries that may not be easily identifiable when lying in a supine position. The assessment includes an examination of the perineum, buttocks, and lower gluteal, anal, or groin folds (as is vital to examine the patients back, flanks, and axilla).
Recognition of rectal injuries requires a high level of suspicion in those evaluating any patient with a penetrating wound. This suspicion should increase with any identification of penetrating wounds to the lower abdomen, pelvis, perineum, buttocks, or thighs. Penetrating wounds should be counted and marked (one approach is a simple paper clip gets taped adjacent to the penetration site) to help physicians hypothesize missile projection. If the count is an odd number of penetrating wounds, the physician should have heightened suspicion that a foreign body may remain in the victim.
As with all penetrating wounds via knife, spear, or other large objects, these should not get removed until the patient is in a controlled environment, i.e., the operating room, no matter the location of the foreign body.
In all patients who are hemodynamically stable, alert, and oriented, obtaining a detailed history of the events surrounding their injury is essential. Questions pertinent to ask include proximity of projectile when fired, and caliber of the weapon if known. With all patients, it is crucial to attempt to obtain previous past medical, past surgical, and social histories as well as current patient medications and known drug allergies.
Evaluation
In the diagnostic assessment of a trauma patient, bedside ultrasonography in the form of the focused assessment with sonography for trauma (FAST) examination is considered standard of care. This diagnostic modality allows the operator to perform evaluations simultaneously during the primary of the initial assessment, as outlined above. Of the four views, the suprapubic location with visualization of the pelvic cul de sac requires inspection with a concern of penetrating rectal trauma. The presence of fluid in this window may indicate intra-abdominal hemorrhage, hollow viscus injury, hemoperitoneum, or ascites. A threshold of at least 200mL of fluid is necessary for the detection of fluid within the intra-abdominal cavity. Most recently, a FAST exam is noted to have a sensitivity of 69.8% and a specificity of 92.1%.[11] Positive findings in a stable patient can be evaluated further with CT. In contrast, positive findings in an unstable patient necessitate the surgeon to take the patient to the operating room for emergent abdominal exploration.
Prio practice was that all patients where there was a concern of penetrating rectal injury should undergo a digital rectal exam during the secondary trauma survey; this, however, has raised controversy and recently been called into question. Digital rectal examination is, however, not supported due to low sensitivity, approximately 51% of this test being inadequate to effectively rule out injury, coupled with significant risk for enlargening rectal perforation with a blind examination.[12][13][14][15] The physician, however, may attempt to directly visualize rectal injury with a higher yield modality, such as intraoperative examination with proctosigmoidoscopy. A senior-level physician who is familiar with proctosigmoidoscopy should perform this exam. If the location of the injury is not identifiable, blood seen on rigid proctosigmoidoscopy has been determined to have a sensitivity as high as 90% for the diagnosis of rectal injury.[16]
Computer tomography (CT) with IV contrast is the most useful adjunct for evaluation in the stable trauma patient to help identify missile trajectory, in addition to evaluation and/or determination of other concomitant injuries. If encountering hematuria during Foley catheter insertion, CT cystography may as well be useful to rule out associated bladder injury.[17][18]
Treatment / Management
The evidence-based management of rectal trauma is formulated based on the patient’s physiology and anatomy. Physiologically the patient is either hemodynamically stable or unstable with massive blood loss, acidosis, hypothermia, and coagulopathy. These patients would go straight to the operating room and have a damage control operation performed. This scenario is not uncommon for rectal trauma since the etiology is 85% gunshot wounds and blunt injuries are usually secondary to open-book pelvic fractures.
For the hemodynamically stable patient, the rectal injury is repaired based on the anatomy of the wound.[19] The rectum is partially intraperitoneal (anterior and lateral surfaces of the upper two-thirds, and partly extraperitoneal (posterior surface, and circumferential lower one-third). The management of intra-peritoneal wounds is the same as colon injuries. Primary repair with or without proximal diversion. The patient should also receive broad-spectrum antibiotics covering gram-negative and anaerobes for 24 hours. If the injury is nondestructive (less than 50% of the circumference of the intraperitoneal rectum), it can undergo repair. If the wound is destructive (greater than 50% circumferential involvement), the rectum requires resection to viable, healthy tissue and re-anastomosed.
Over the last several decades, there have been multiple studies showing that fecal diversion is not necessary, except in the setting of various transfusion requirements or hypotension. In 1979 Stone and Fabian performed a randomized prospective trial comparing primary repair of colon injuries versus colostomy creation and found equivalent infection (48% vs. 57% p>0.05) and mortality rates (1.5% vs. 1.4% p>50). This historical study revolutionized the management of colorectal trauma. In 2001, the American Association for the Surgery of Trauma conducted a prospective multicenter study on penetrating colon injuries, comparing diversion or primary repair. This study demonstrated lower mortality in the primary repair arm (0% vs. 1.3%).[9] A 2009 Cochrane review examined six randomized trials on colon injuries comparing primary repair versus fecal diversion from 1975 to 2002. [20] This also revealed a significantly lower rate of wound complication and infection with primary repair.(B2)
When considering diversion, one must take into account all of the complications of ostomies. There is a 35 to 55% complication incidence from forming an ostomy itself. The readmission rate is as high as 17% secondary to multiple potential complications, including parastomal hernias, stenosis, retraction, and metabolic imbalance.[21][22][23][24][25] With the reversal of the ostomy, there is a 5 to 25% complication rate, with a local wound infection rate of 3 to 20%.[21][23](A1)
In 2006, Gonzalez did a trial of 14 patients with nondestructive rectal trauma without fecal diversion and had no complications or mortality.[26] If one compares nondestructive rectal injuries in the non-trauma world, such as draining pelvic abscess of the rectum, excising rectal tumor trans-anally, or draining supra levator abscess via the rectum, none of these procedures require a fecal diversion.[27][28](B2)
For destructive extraperitoneal rectal trauma (greater than 50% circumferential involvement), associated pelvic fractures, or concomitant vascular injuries that can compromise the blood supply to the rectum causing anastomotic failure; fecal diversion would be a safe alternative. With regards to presacral drainage and distal washout, these procedures were established during the Vietnam Conflict and published in 1971 by Lavenson and Cohen. Over the past several decades, there have been numerous studies demonstrating no benefit in presacral drainage or distal rectal washout. For extraperitoneal rectal injuries, there is controversy over fecal diversion, presacral drainage, and distal rectal washout. The Eastern Association of the Surgery of Trauma (EAST) recently published guidelines on fecal diversion for extraperitoneal rectal trauma despite finding the quality of evidence to be weak, and conditionally recommended proximal diversion.[20] The Eastern Association of the Surgery of Trauma practice management guidelines on nondestructive penetrating extraperitoneal rectal injuries also conditionally recommended not performing rectal washout or pre-sacral drainage.[20]
The exception to this is wartime related injuries, where there is severe presacral destruction with large soft tissue injury or those associated with pelvic fractures. The patient with severe presacral destruction and large soft tissue injuries associated with pelvic fractures are much more commonly seen in war-related injuries.[29] It is in these patients where proximal diversion is indicated, with the use of pre-sacral drainage not clearly defined, and overall not well supported.
Blunt trauma accounts for 1 to 2% of rectal trauma and is usually secondary to an anterior-posterior compression mechanism causing an open book pelvic fracture.[6][7] These injuries should always have fecal diversion. (B2)
Concomitant bladder injury with rectal trauma does not increase the rate of abdominal complication nor mortality. Fecal diversion does not change the outcome of concomitant traumatic bladder injuries.[30]
Differential Diagnosis
Suspicion for rectal injury should increase with any identification of penetrating wound to the lower abdomen, pelvis, perineum, buttocks, or thighs. With the identification of trauma to this region, the differential diagnosis must include intra-peritoneal vs. extraperitoneal rectal injury, vascular injury, bladder injury. Nearly any major vasculature or viscera may be injured and subsequently must be excluded with the identification of a penetrating injury.
Prognosis
The overall prognosis for patients who sustain rectal trauma is again multifactorial, including but not limited to patient’s age, comorbidities, hemodynamics, concomitant injuries, and, as discussed, the location of injury (intraperitoneal compared to extraperitoneal). Despite advances in trauma guidelines, mortality rates en total remain between 3 and 10% with additional morbidity of 18 to 21%.[31]
Brown et al. performed a retrospective review from 2004 to 2015, of all patients sustaining a traumatic rectal injury at 22 participating level 1 trauma centers. They demonstrated patients with intraperitoneal rectal injuries that underwent proximal diversion sustained more abdominal complications thereafter than those that did not (22% vs. 10% p=0.003). Further independent risk factors for intra-abdominal complications in patients with intraperitoneal injury included a high-grade injury (defined as AAST grade greater than II) or if the mechanism of injury was of penetrating in nature. Regardless of proximal diversion, there was no difference in overall mortality (3% vs. 2% p=0.66), excluding patients that died within 48 hours of hospital arrival.[32]
Prognosis is similar concerning extraperitoneal injury. The same study showed no difference in mortality in the extraperitoneal rectal injury population, with proximal diversion, found to be (2% vs. 1% p=0.55), again excluding those that died within 48 hours of arrival. After multivariate analysis, independent risk factors for complications with extraperitoneal injuries were those that received distal rectal washout (OR 3.4 p=0.008) and presacral drain placement (OR 2.6 p=0.02).[32]
Although only selectively indicated for destructive extraperitoneal rectal injuries, proximal diversion and creation of an ostomy are important to note for prognosis, as this holds 25 to 55% complications incidence in and of itself.[21][22][23]
Complications
In most studies related to bowel injury, similar factors predispose to the relative risk for infectious morbidity and primary repair or anastomotic failure. These relative risks include fecal contamination, extensive blood loss, and hemodynamic instability or shock state. Further severe concern complications from direct rectal injury include wound infection, abdominal and or pelvic/retroperitoneal abscess, fistulous tract formation, fascial dehiscence, bacteremia, and necrotizing fasciitis.[19] Non-life-threatening conditions with lifestyle implications include not only possible ostomy maintenance but as well as fecal incontinence.
Despite increasing literature against and need to increase selectivity, proximal diversion, and ostomy creation in multi-institute studies examining rectal trauma are as high as 76%. Ostomy complications include parastomal hernias, stenosis, retraction, and metabolic imbalance. With the reversal of an ostomy, there is a risk for local wound infections between 3 to 20%.[21][22][23]
Deterrence and Patient Education
Some authors recommend manual disimpaction/evacuation of stool from the rectum to assist with early healing. In a similar nature, patients must maintain a high fiber diet and start stool softeners early during recovery to assist in bowel recovery.
Enhancing Healthcare Team Outcomes
Effective interprofessional teamwork is imperative in the trauma setting, an uncertain and complicated scenario, of resuscitating critically injured patients. From initial evaluation by EMS, to all those involved in the trauma bay, to post-operative an interprofessional care, including but not limited to surgeons, trauma nursing staff, operative staff, anesthesia, pharmacists, physical and occupational therapists, care management, consultants and nutritionists, there is a broad span of participants that contribute to overall patient outcome.
The presence or absence of a trauma team leader (TTL) at a Level I trauma center, demonstrated that TTL involvement during resuscitations correlated with improved adherence to trauma protocols, and increased efficiency (compared to no TTL involvement) to diagnostic imaging.[33]
Efforts to further improve teamwork in trauma include simulation-based interprofessional team training with non-technical skills (NTS) focus. Again to further strength non-procedural, intangibles of teamwork. The various specialties will coordinate with the nursing staff irrespective of the procedural management of the case. Nursing will assist in surgery, prepare the patient, provide counsel and reassurance to the patient, and administer medications and provide postoperative care, reporting any concerns to the clinical staff. The creation, staffing, and maintenance of effective trauma teams require training strategies such as interprofessional simulation that target team training interaction. Specifically, training needs to focus on developing non-technical skills for resuscitation, and management of wounds and a stoma. There is ample evidence showing that interprofessional teamwork leads to better outcomes in most trauma patients.[34][35] [Level 5]
Media
(Click Image to Enlarge)
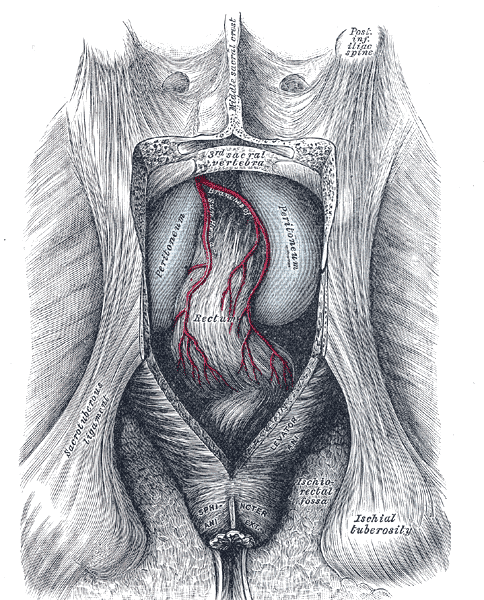
The Large Intestine, The posterior aspect of the rectum exposed by removing the lower part of the sacrum and the coccyx, Ischial tuberosity, sacrotuberous ligament
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
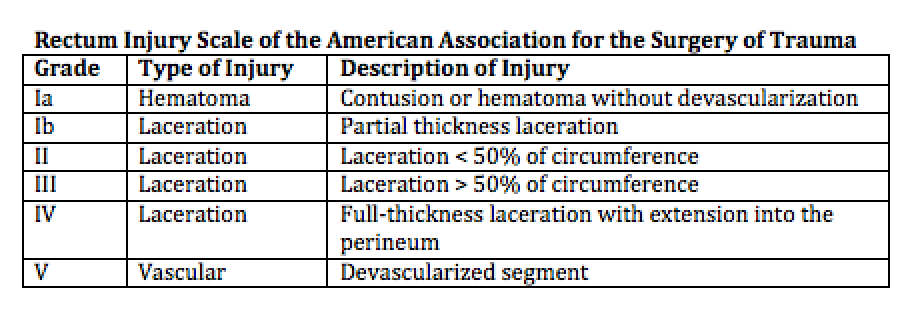
Rectum Injury Scale Contributed by the American Association of the Surgery of Trauma
(Click Image to Enlarge)
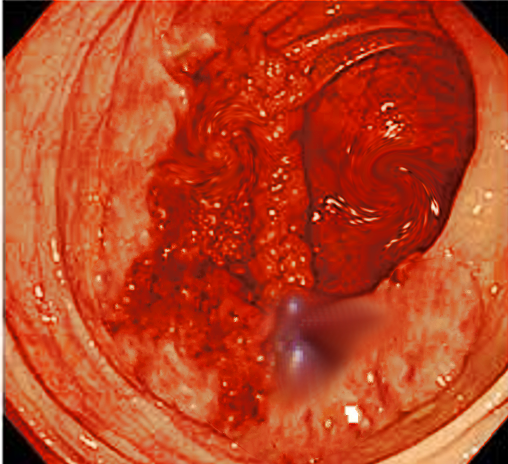
Rectal trauma (gunshot) Image courtesy S Bhimji MD
References
OGILVIE WH. Surgical advances during the war. Journal of the Royal Army Medical Corps. 1945 Dec:85():259-65 [PubMed PMID: 21011547]
Level 3 (low-level) evidenceOgilvie WH. Surgical Lessons of War applied to Civil Practice. British medical journal. 1945 May 5:1(4400):619-23 [PubMed PMID: 20786044]
OGILVIE WH. Abdominal wounds in the Western Desert. Bulletin of the U.S. Army Medical Department. United States. Army. Medical Department. 1946 Oct:6(4):435-45 [PubMed PMID: 20275008]
Steele SR, Maykel JA, Johnson EK. Traumatic injury of the colon and rectum: the evidence vs dogma. Diseases of the colon and rectum. 2011 Sep:54(9):1184-201. doi: 10.1007/DCR.0b013e3182188a60. Epub [PubMed PMID: 21825901]
Demetriades D, Karaiskakis M, Toutouzas K, Alo K, Velmahos G, Chan L. Pelvic fractures: epidemiology and predictors of associated abdominal injuries and outcomes. Journal of the American College of Surgeons. 2002 Jul:195(1):1-10 [PubMed PMID: 12113532]
Aihara R, Blansfield JS, Millham FH, LaMorte WW, Hirsch EF. Fracture locations influence the likelihood of rectal and lower urinary tract injuries in patients sustaining pelvic fractures. The Journal of trauma. 2002 Feb:52(2):205-8; discussion 208-9 [PubMed PMID: 11834976]
Level 2 (mid-level) evidenceGiannoudis PV, Grotz MR, Tzioupis C, Dinopoulos H, Wells GE, Bouamra O, Lecky F. Prevalence of pelvic fractures, associated injuries, and mortality: the United Kingdom perspective. The Journal of trauma. 2007 Oct:63(4):875-83 [PubMed PMID: 18090020]
Level 3 (low-level) evidenceHudolin T, Hudolin I. The role of primary repair for colonic injuries in wartime. The British journal of surgery. 2005 May:92(5):643-7 [PubMed PMID: 15800953]
Demetriades D, Murray JA, Chan L, Ordoñez C, Bowley D, Nagy KK, Cornwell EE 3rd, Velmahos GC, Muñoz N, Hatzitheofilou C, Schwab CW, Rodriguez A, Cornejo C, Davis KA, Namias N, Wisner DH, Ivatury RR, Moore EE, Acosta JA, Maull KI, Thomason MH, Spain DA, Committee on Multicenter Clinical Trials. American Association for the Surgery of Trauma. Penetrating colon injuries requiring resection: diversion or primary anastomosis? An AAST prospective multicenter study. The Journal of trauma. 2001 May:50(5):765-75 [PubMed PMID: 11371831]
Level 2 (mid-level) evidenceSchipper IB, Schep N. [ATLS - a pioneer in trauma education; history and effects]. Nederlands tijdschrift voor geneeskunde. 2017:161():D1569 [PubMed PMID: 28466801]
Engles S, Saini NS, Rathore S. Emergency Focused Assessment with Sonography in Blunt Trauma Abdomen. International journal of applied & basic medical research. 2019 Oct-Dec:9(4):193-196. doi: 10.4103/ijabmr.IJABMR_273_19. Epub 2019 Oct 11 [PubMed PMID: 31681541]
Ball CG, Jafri SM, Kirkpatrick AW, Rajani RR, Rozycki GS, Feliciano DV, Wyrzykowski AD. Traumatic urethral injuries: does the digital rectal examination really help us? Injury. 2009 Sep:40(9):984-6. doi: 10.1016/j.injury.2009.03.003. Epub 2009 Jun 16 [PubMed PMID: 19535063]
Level 2 (mid-level) evidenceEsposito TJ, Ingraham A, Luchette FA, Sears BW, Santaniello JM, Davis KA, Poulakidas SJ, Gamelli RL. Reasons to omit digital rectal exam in trauma patients: no fingers, no rectum, no useful additional information. The Journal of trauma. 2005 Dec:59(6):1314-9 [PubMed PMID: 16394903]
Shlamovitz GZ, Mower WR, Bergman J, Crisp J, DeVore HK, Hardy D, Sargent M, Shroff SD, Snyder E, Morgan MT. Poor test characteristics for the digital rectal examination in trauma patients. Annals of emergency medicine. 2007 Jul:50(1):25-33, 33.e1 [PubMed PMID: 17391807]
Level 2 (mid-level) evidencePorter JM, Ursic CM. Digital rectal examination for trauma: does every patient need one? The American surgeon. 2001 May:67(5):438-41 [PubMed PMID: 11379644]
Hargraves MB, Magnotti LJ, Fischer PE, Schroeppel TJ, Zarzaur BL, Fabian TC, Croce MA. Injury location dictates utility of digital rectal examination and rigid sigmoidoscopy in the evaluation of penetrating rectal trauma. The American surgeon. 2009 Nov:75(11):1069-72 [PubMed PMID: 19927507]
Shanmuganathan K, Mirvis SE, Chiu WC, Killeen KL, Scalea TM. Triple-contrast helical CT in penetrating torso trauma: a prospective study to determine peritoneal violation and the need for laparotomy. AJR. American journal of roentgenology. 2001 Dec:177(6):1247-56 [PubMed PMID: 11717058]
Shanmuganathan K, Mirvis SE, Chiu WC, Killeen KL, Hogan GJ, Scalea TM. Penetrating torso trauma: triple-contrast helical CT in peritoneal violation and organ injury--a prospective study in 200 patients. Radiology. 2004 Jun:231(3):775-84 [PubMed PMID: 15105455]
Weinberg JA, Fabian TC, Magnotti LJ, Minard G, Bee TK, Edwards N, Claridge JA, Croce MA. Penetrating rectal trauma: management by anatomic distinction improves outcome. The Journal of trauma. 2006 Mar:60(3):508-13; discussion 513-14 [PubMed PMID: 16531847]
Bosarge PL, Como JJ, Fox N, Falck-Ytter Y, Haut ER, Dorion HA, Patel NJ, Rushing A, Raff LA, McDonald AA, Robinson BR, McGwin G Jr, Gonzalez RP. Management of penetrating extraperitoneal rectal injuries: An Eastern Association for the Surgery of Trauma practice management guideline. The journal of trauma and acute care surgery. 2016 Mar:80(3):546-51. doi: 10.1097/TA.0000000000000953. Epub [PubMed PMID: 26713970]
Hendren S, Hammond K, Glasgow SC, Perry WB, Buie WD, Steele SR, Rafferty J. Clinical practice guidelines for ostomy surgery. Diseases of the colon and rectum. 2015 Apr:58(4):375-87. doi: 10.1097/DCR.0000000000000347. Epub [PubMed PMID: 25751793]
Level 1 (high-level) evidenceRobertson JP, Puckett J, Vather R, Jaung R, Bissett I. Early closure of temporary loop ileostomies: a systematic review. Ostomy/wound management. 2015 May:61(5):50-7 [PubMed PMID: 25965092]
Level 1 (high-level) evidenceChow A, Tilney HS, Paraskeva P, Jeyarajah S, Zacharakis E, Purkayastha S. The morbidity surrounding reversal of defunctioning ileostomies: a systematic review of 48 studies including 6,107 cases. International journal of colorectal disease. 2009 Jun:24(6):711-23. doi: 10.1007/s00384-009-0660-z. Epub 2009 Feb 17 [PubMed PMID: 19221766]
Level 1 (high-level) evidenceKrouse RS, Grant M, Wendel CS, Mohler MJ, Rawl SM, Baldwin CM, Coons SJ, McCorkle R, Ko CY, Schmidt CM. A mixed-methods evaluation of health-related quality of life for male veterans with and without intestinal stomas. Diseases of the colon and rectum. 2007 Dec:50(12):2054-66 [PubMed PMID: 17701071]
Level 2 (mid-level) evidenceClemens MS, Heafner TA, Watson JD, Aden JK 3rd, Rasmussen TE, Glasgow SC. Quality of Life in United States Veterans With Combat-Related Ostomies From Iraq and Afghanistan. Military medicine. 2016 Nov:181(11):e1569-e1574 [PubMed PMID: 27849491]
Level 2 (mid-level) evidenceGonzalez RP, Phelan H 3rd, Hassan M, Ellis CN, Rodning CB. Is fecal diversion necessary for nondestructive penetrating extraperitoneal rectal injuries? The Journal of trauma. 2006 Oct:61(4):815-9 [PubMed PMID: 17033545]
Level 2 (mid-level) evidenceKeller DS, Tahilramani RN, Flores-Gonzalez JR, Mahmood A, Haas EM. Transanal Minimally Invasive Surgery: Review of Indications and Outcomes from 75 Consecutive Patients. Journal of the American College of Surgeons. 2016 May:222(5):814-22. doi: 10.1016/j.jamcollsurg.2016.02.003. Epub 2016 Feb 13 [PubMed PMID: 27016903]
Althumairi AA, Gearhart SL. Local excision for early rectal cancer: transanal endoscopic microsurgery and beyond. Journal of gastrointestinal oncology. 2015 Jun:6(3):296-306. doi: 10.3978/j.issn.2078-6891.2015.022. Epub [PubMed PMID: 26029457]
Cleary RK, Pomerantz RA, Lampman RM. Colon and rectal injuries. Diseases of the colon and rectum. 2006 Aug:49(8):1203-22 [PubMed PMID: 16858663]
Osterberg EC, Veith J, Brown CVR, Sharpe JP, Musonza T, Holcomb JB, Bui E, Bruns B, Hopper HA, Truitt M, Burlew CC, Schellenberg M, Sava J, Van Horn J, AAST Contemporary Management of Rectal Injuries Study Group. Concomitant bladder and rectal injuries: Results from the American Association for the Surgery of Trauma Multicenter Rectal Injury Study Group. The journal of trauma and acute care surgery. 2020 Feb:88(2):286-291. doi: 10.1097/TA.0000000000002451. Epub [PubMed PMID: 31343599]
Clemens MS, Peace KM, Yi F. Rectal Trauma: Evidence-Based Practices. Clinics in colon and rectal surgery. 2018 Jan:31(1):17-23. doi: 10.1055/s-0037-1602182. Epub 2017 Dec 19 [PubMed PMID: 29379403]
Brown CVR, Teixeira PG, Furay E, Sharpe JP, Musonza T, Holcomb J, Bui E, Bruns B, Hopper HA, Truitt MS, Burlew CC, Schellenberg M, Sava J, VanHorn J, Eastridge PB, Cross AM, Vasak R, Vercruysse G, Curtis EE, Haan J, Coimbra R, Bohan P, Gale S, Bendix PG, AAST Contemporary Management of Rectal Injuries Study Group. Contemporary management of rectal injuries at Level I trauma centers: The results of an American Association for the Surgery of Trauma multi-institutional study. The journal of trauma and acute care surgery. 2018 Feb:84(2):225-233. doi: 10.1097/TA.0000000000001739. Epub [PubMed PMID: 29140953]
Tsang B, McKee J, Engels PT, Paton-Gay D, Widder SL. Compliance to advanced trauma life support protocols in adult trauma patients in the acute setting. World journal of emergency surgery : WJES. 2013 Oct 2:8(1):39. doi: 10.1186/1749-7922-8-39. Epub 2013 Oct 2 [PubMed PMID: 24088362]
Murphy M, McCloughen A, Curtis K. The impact of simulated multidisciplinary Trauma Team Training on team performance: A qualitative study. Australasian emergency care. 2019 Mar:22(1):1-7. doi: 10.1016/j.auec.2018.11.003. Epub 2018 Dec 10 [PubMed PMID: 30998866]
Level 2 (mid-level) evidenceSarani B, Paspulati RM, Hambley J, Efron D, Martinez J, Perez A, Bowles-Cintron R, Yi F, Hill S, Meyer D, Maykel J, Attalla S, Kochman M, Steele S. A multidisciplinary approach to diagnosis and management of bowel obstruction. Current problems in surgery. 2018 Oct:55(10):394-438. doi: 10.1067/j.cpsurg.2018.09.001. Epub 2018 Sep 22 [PubMed PMID: 30526888]