Introduction
The fossa ovalis is a depressed structure, of varying shapes, located in the inferior aspect of the right interatrial septum.[1] A remnant of an interatrial opening, the foramen ovale, which has a significant role in fetal circulation, the fossa ovalis forms by the fusion of the septum primum and septum secundum.[2] This article will describe the structure, function, embryology, vascular supply, physiologic variants, surgical considerations, and clinical significance of the fossa ovalis.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The fossa ovalis is a depressed structure located in the lower portion of the right atrial side of the interatrial septum.[2][3] Although the fossa ovalis appears two-dimensional, it is, in fact, a three-dimensional structure - consisting of the septum primum, septum secundum, and the annulus or limbus fossa ovalis which raises around the perimeter of the fossa ovalis.[4] Important neighboring structures are as follows: below and rightward of the fossa ovalis lies the inferior vena cava opening; the location of the coronary sinus is anterior to the fossa ovalis; along the same horizontal plane of the fossa ovalis is the His bundle. [2][5] The fossa ovalis forms part of the atrial septum which appears expansive from the right atrial view. However, the true and false atrial septa are clinically important features that need to be distinguished. [6][3] The true interatrial septum contains the fossa ovalis and comprises only 20% of the entire septum. It is the only area through which the interatrial septum may be traversed without the risk of cardiac perforation.[6] In the normal heart, the fossa ovalis serves to prevent blood flow, i.e., shunting of blood, across the interatrial septum.[7]
Embryology
During fetal life, ostia within the juxtaposed septa (septum primum and septum secundum) form a one-way flap valve, the foramen ovale, that allows shunting of blood from the right atrium to the left atrium.[4] The septum primum which is on the left atrial side forms the floor of the fossa ovalis, whereas the septum secundum derived from an infolding of the roof of the atrium forms the limbus of the fossa ovalis.[2][4] Physiologic increase in the left heart pressure at the time of birth allows the septum primum to create a tight seal with the septum secundum, creating the fossa ovalis.[8] This fusion of the septum primum with the septum secundum and subsequent formation of the fossa ovalis occurs in 75% of cases, failure of which leads to a patent foramen ovale. Also, the fossa ovalis undergo thinning in utero.[7]
Blood Supply and Lymphatics
The interatrial septum (IAS) receives vascular supply by anastomoses between the left and right branches of the anterior and posterior atrial branches of the right and left coronary arteries; termed Kugel’s artery or arteria anastomotica auricularis magna.[9][10] The fossa ovalis together with the middle part of the IAS receives the least vascular supply, additionally, the number and density of these vessels’ networks decrease with age, whereas the anteroinferior portion of the septum receives the densest vascular network.[11]
Nerves
The right atrium has an angiotensinergic innervation and is a source of angiotensin II. The peripheral fibers are mainly non-catecholaminergic afferents and vagal efferents with a small amount being sympathetic. [12]
Muscles
The pectinate muscles or musculi pectinati compose the walls of the atria. They are parallel ridges in the walls of the right atrium. The crista terminalis is a smooth muscular ridge in the superior portion of the right atrium. It divides the musculi pectinati and the right atrial appendage from the smooth surface of the right atrium.[13]
Physiologic Variants
The fossa ovalis may assume various shapes and dimensions.[2][3] It most commonly assumes an oval shape but may be circular or even elliptical. The dimensions of the fossa ovalis vary among populations as well as by the measuring tools employed but may correlate with the patient's weight of the heart, age, and body weight.[2][6] Significant variations of the fossa ovalis exist, with recesses, slits, aneurysms, and fibrous strands found in certain specimens.[2]
Surgical Considerations
The (limbus) fossa ovalis represents the most direct anatomical landmark for atrial septal puncture for various procedures and may be located using the His bundle electrogram locating method.[5]The following are significant procedures that require the location of the fossa ovalis for transseptal puncture[6]
- Patent foramen ovale and atrial septal defect repair
- Right heart catheterization
- Percutaneous balloon valvuloplasty
- Radiofrequency catheter ablation
- Pulmonary vein isolation
- Left atrial appendage closure
- Catheter-based mitral valve repair
- Hemodynamic assessment of the mitral valve
- Paravalvular leak closure
- Alternative access to the left ventricle in the presence of a prosthetic aortic valve
Intracardiac echocardiography (ICE) and fluoroscopy are useful for identifying the fossa ovalis, a critical landmark for electrophysiological procedures.[14]
Clinical Significance
The fossa ovalis may be a frequent site of cardiac pathology. Known pathologies involving the fossa ovalis include:
- Premature closure of the foramen ovale & Patent foramen ovale (PFO)
- Atrial septal defect (ASD)
- Rheumatic heart disease
- Amyloidosis
- Tumors: Prichard’s structures, myxomas, lipomatous hypertrophy of the cardiac interatrial septum
- Fossa ovalis membrane aneurysm (FOMA)
- Cardiac arrhythmias
Patent foramen ovale and atrial septal defect represent functionally similar pathologies; however, they differ in their etiology as well as clinical severity. ASDs are the result of the failure to form either of the interatrial septa (septum primum, septum secundum) or sinus venosus, whereas PFOs result when, in approximately 25% of the population, there is a failure of closure of the foramen ovale created by the septa.[8] Both diseases are characterized clinically by the presence of migraines, paradoxical emboli and strokes, and decompression sickness.[1][8] The size of a patent foramen ovale largely correlates with its clinical severity; larger lesions correlate with more severe illness and a higher risk of paradoxical emboli.[15]
Atrial septal defects may occur in isolation or as part of a syndrome. Several genes have been implicated in the development of atrial septal defects. NKX2.5 gene is known to produce secundum type defects, TBX5 gene mutations result in Holt-Oram syndrome which features ASD.[2] Atrial septal defects may undergo spontaneous closure depending on their initial size at the time of diagnosis, found to be the best predictor of the progression of such defects. Holes in the fossa ovalis measuring less than 8mm and/or containing aneurysms may diminish in size or resolve spontaneously.[16][17] However, failure of closure usually leads to enlargement of the defect and the need for surgical closure.[16][18]
The structure and dimensions of the fossa ovalis are altered in the course of rheumatic heart disease.[19] Rheumatic heart disease is characterized by extensive scarring of valves and other structures within the heart.[20] The fossa ovalis may assume a more horizontal orientation in addition to a larger surface area; hemodynamic alterations are also prominent in this setting.[19]
Amyloidosis, characterized by diffuse thickening of heart valves, does not spare the interatrial septum. Thickening of the interatrial septum is 100% specific for amyloidosis [21]
The fossa ovalis is a frequent site of atrial myxomas. Atrial myxomas are true neoplasms, appearing as pedunculated friable masses attached to the interatrial septum.[22] These masses present with a wide range of symptoms ranging from dyspnea to hemiplegia.[22][23]
Prichard's structures are also benign structures derived from mature endothelial cells, they are more frequently found in individuals beyond 60 years of age and are unrelated to cardiac myxomas.[24] These structures may be subendothelial or located within the atrial cavity, commonly on the left side of the fossa ovalis, and may be the result of hemodynamic alterations in blood flow within the heart.[25]
Lipomatous hypertrophy is fat accumulation greater than 2cm located on the interatrial septum. The mass characteristically spares the fossa ovalis. Arrhythmias and sudden cardiac death may be accompanying complications.[26][27] Obstruction of the vena cava ostium may be present in larger lesions.[28] The occurrence of lipomatous hypertrophy of the septum has correlations with obesity, older age, female gender, steroid use.[28]
The fossa ovalis is found to be aneurysmal in some cases but is present with increased incidence in patients with stroke.[2] Fossa ovalis membrane aneurysms present as focal bulging of the interatrial septum, with displacement towards the left or right atrium.[29][30][31] FOMA carries a significant risk of fibrosis and thrombus formation within its wall with related complications, as well as the formation of an ASD from a preexisting PFO leading to increased intracardiac shunting. It is often the result of elevated intracardiac pressures arising from secondary cardiac pathologies, most commonly ischemic heart disease, aortic and mitral valvular diseases.[29] Transesophageal echocardiography represents the best method of visualizing fossa ovalis membrane aneurysms in patients suspected of cardiogenic emboli, although the emboli may arise from a different source.[32][33]
Electrophysiological studies may reveal increased automaticity in the region of the limbus fossa ovalis. Such automaticity may manifest as reversible focal atrial tachycardia and chaotic atrial rhythm and is responsive to focal radiofrequency ablation of the limbus with the restoration of cardiac function.[34][35]
Other Issues
Most patients with cryptogenic stroke have a patent foramen ovale which serves as a channel for paradoxical emboli leading to a greater incidence of cerebrovascular accidents.[3] Proper screening for patent foramen ovale requires transthoracic agitated saline contrast echocardiography during a cough or in conjunction with Valsalva maneuver.[36][37] Interatrial shunting is confirmed by the presence of more than five bubbles in the left atrial chamber within three cardiac cycles.[37] Closure of patent foramen ovale requires a detailed echocardiographic workup for anatomical variations, as this is crucial in deciding the most appropriate closure device, to prevent residual shunts.[3][2]
Media
(Click Image to Enlarge)

Patent Foramen Ovale. Most adult patients with patent foramen ovale are asymptomatic. In some adults, patent foramen ovale may result in an interatrial, right-to-left shunting of deoxygenated blood and the potential for shunting venous thromboembolism to the arterial circulation.
Contributed by O Chaigasame, MD
(Click Image to Enlarge)
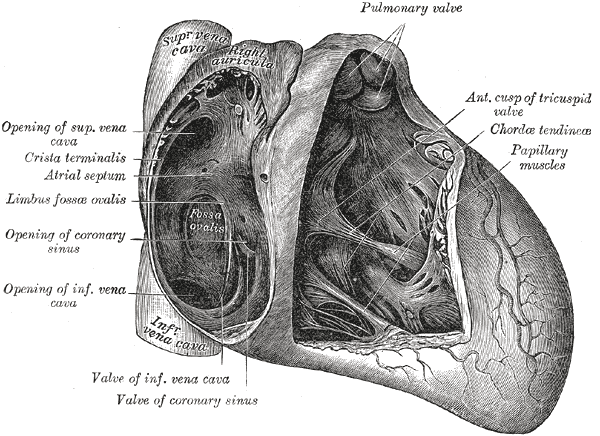
The fossa ovalis depicted on imaging and anatomically. Contributed from the Wikimedia User: Bartleby From Henry Gray "Gray's Anatomy (Public Domain)
(Click Image to Enlarge)
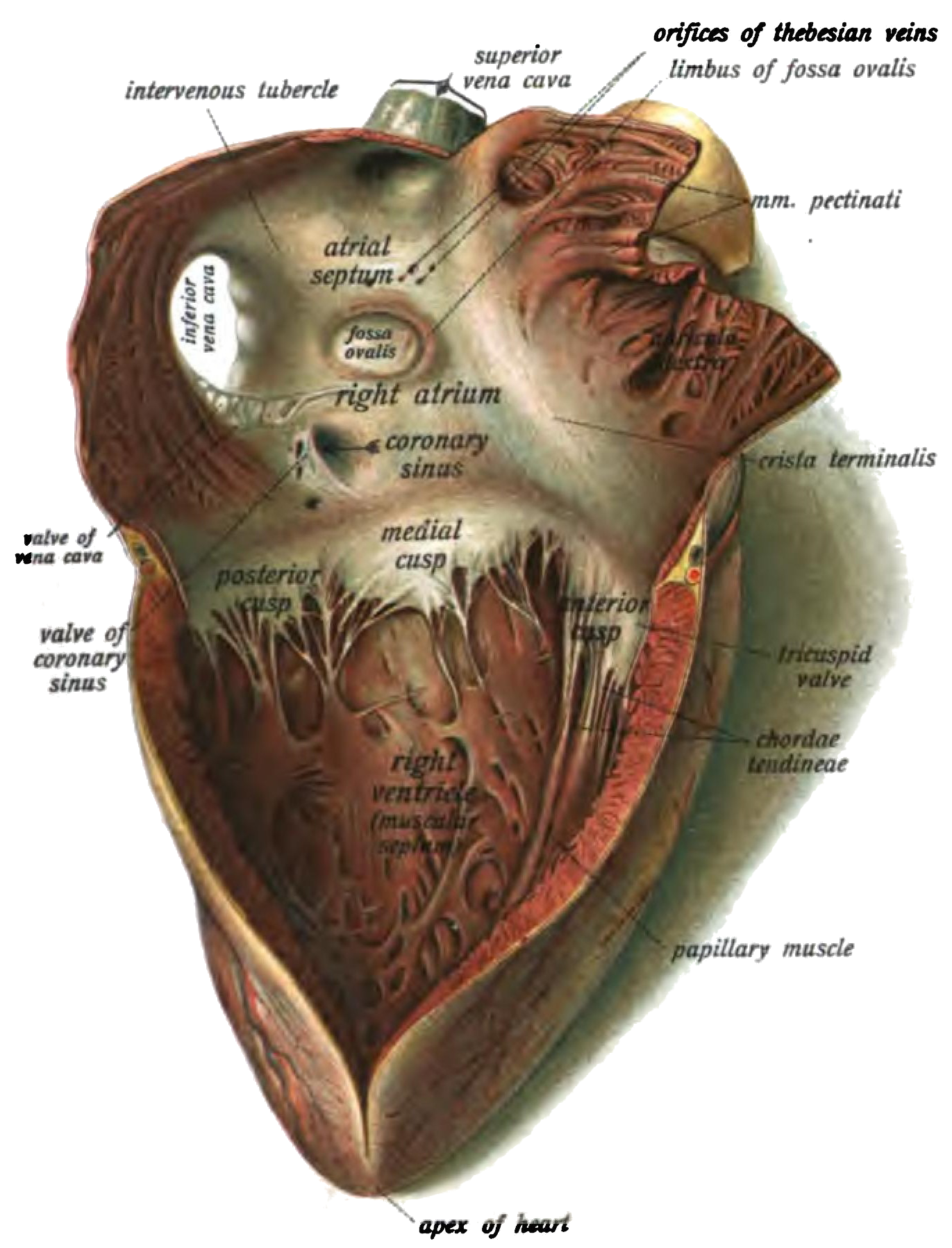
The anatomy and location of the fossa ovalis in reference to other structures of the heart. Contributed by Wikimedia User: Dr. Johannes Sobotta, (Public Domain )
(Click Image to Enlarge)
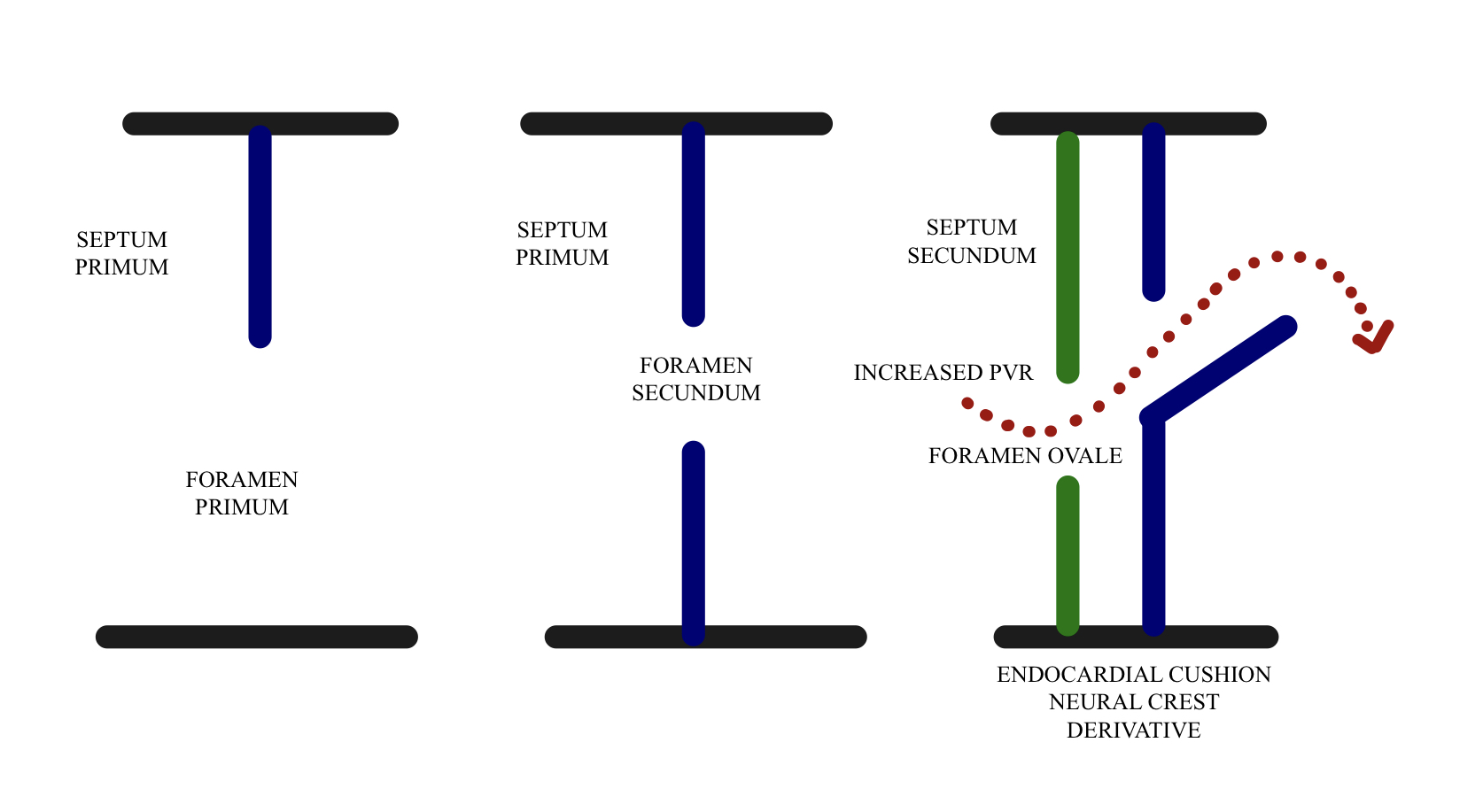
The failure of the foramen ovale to close at birth resulting in a PFO. Contributed by Piyush Sharma, MDc
(Click Image to Enlarge)
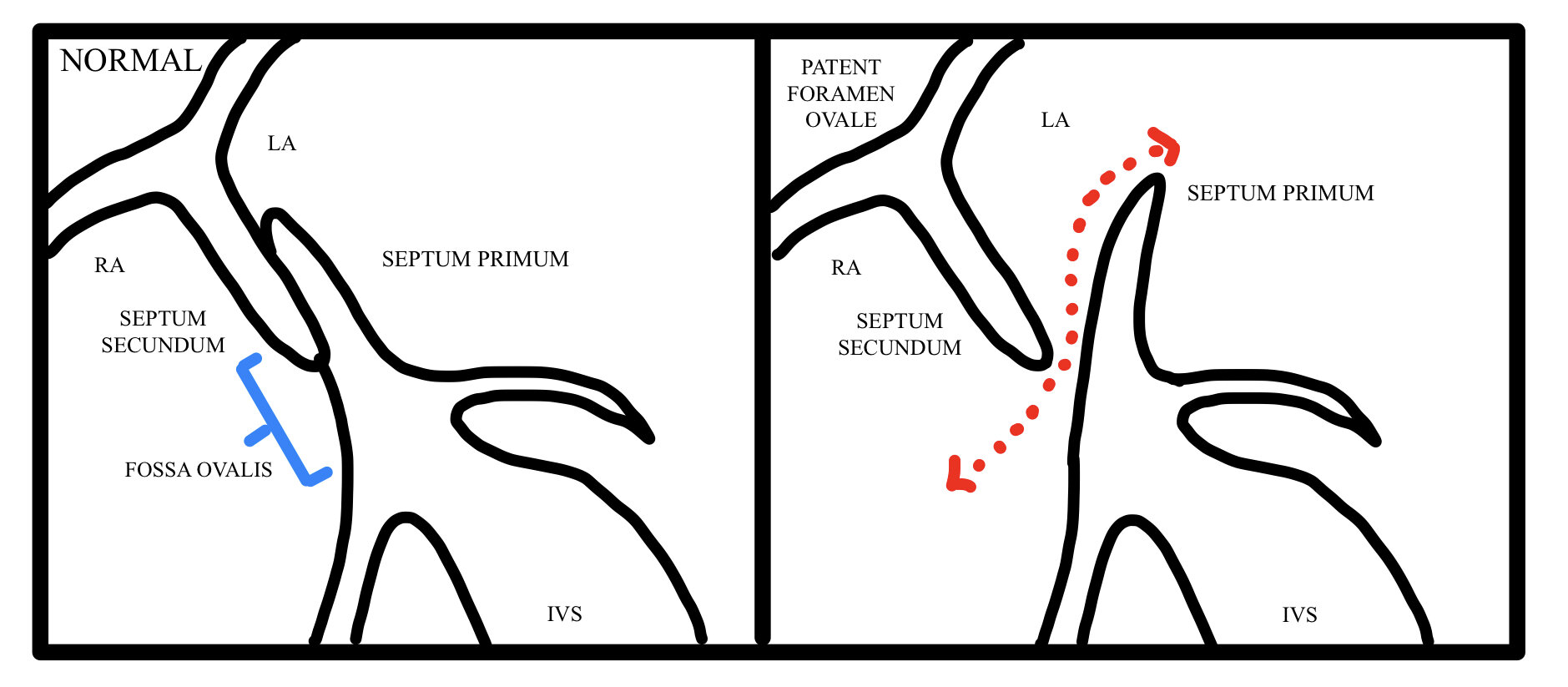
Patent foramen ovale Contributed by Piyush Sharma
References
Malik SB, Kwan D, Shah AB, Hsu JY. The right atrium: gateway to the heart--anatomic and pathologic imaging findings. Radiographics : a review publication of the Radiological Society of North America, Inc. 2015 Jan-Feb:35(1):14-31. doi: 10.1148/rg.351130010. Epub [PubMed PMID: 25590385]
Joshi SD, Chawre HK, Joshi SS. Morphological study of fossa ovalis and its clinical relevance. Indian heart journal. 2016 Mar-Apr:68(2):147-52. doi: 10.1016/j.ihj.2015.08.001. Epub 2016 Jan 18 [PubMed PMID: 27133322]
Rana BS, Shapiro LM, McCarthy KP, Ho SY. Three-dimensional imaging of the atrial septum and patent foramen ovale anatomy: defining the morphological phenotypes of patent foramen ovale. European journal of echocardiography : the journal of the Working Group on Echocardiography of the European Society of Cardiology. 2010 Dec:11(10):i19-25. doi: 10.1093/ejechocard/jeq122. Epub [PubMed PMID: 21078835]
Barik R. The three-dimensional fossa ovalis. Indian heart journal. 2016 Mar-Apr:68(2):211-2. doi: 10.1016/j.ihj.2016.02.004. Epub 2016 Feb 18 [PubMed PMID: 27133343]
Shen J. [An application of His bundle electrogram to locate fossa ovalis during percutaneous transseptal balloon valvuloplasty]. Zhonghua xin xue guan bing za zhi. 1991 Jun:19(3):153-4, 197 [PubMed PMID: 1914856]
Klimek-Piotrowska W, Hołda MK, Koziej M, Piątek K, Hołda J. Anatomy of the true interatrial septum for transseptal access to the left atrium. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2016 May:205():60-4. doi: 10.1016/j.aanat.2016.01.009. Epub 2016 Feb 12 [PubMed PMID: 26879344]
Terpenning S, White CS. Imaging pitfalls, normal anatomy, and anatomical variants that can simulate disease on cardiac imaging as demonstrated on multidetector computed tomography. Acta radiologica short reports. 2015 Jan:4(1):2047981614562443. doi: 10.1177/2047981614562443. Epub 2015 Jan 9 [PubMed PMID: 25610617]
Level 3 (low-level) evidenceKanaganayagam GS, Malik IS. Modern management of a patent foramen ovale. JRSM cardiovascular disease. 2012 Oct 31:1(7):. doi: 10.1258/cvd.2012.012017. Epub 2012 Oct 31 [PubMed PMID: 24175077]
Krupa U. Arterial vascularization of the interatrial septum in the human heart in relation to the type of coronary ramification. Folia morphologica. 1995:54(1):51-9 [PubMed PMID: 8537068]
Level 1 (high-level) evidenceBoppana VS, Castaño A, Avula UMR, Yamazaki M, Kalifa J. Atrial Coronary Arteries: Anatomy And Atrial Perfusion Territories. Journal of atrial fibrillation. 2011 Sep-Nov:4(3):375. doi: 10.4022/jafib.375. Epub 2011 Sep 30 [PubMed PMID: 28496703]
Sokolov VV, Brezhnev FF, Kharlamov EV. [Sources of the vascularization of the human interatrial septum of the heart with different variants of the atrial blood supply]. Arkhiv anatomii, gistologii i embriologii. 1986 Jul:91(7):29-34 [PubMed PMID: 3753224]
Bohlender JM, Nussberger J, Tevaearai H, Imboden H. Angiotensinergic Innervation of the Human Right Atrium: Implications for Cardiac Reflexes. American journal of hypertension. 2018 Jan 12:31(2):188-196. doi: 10.1093/ajh/hpx163. Epub [PubMed PMID: 28985343]
Siddiqui AU, Daimi SR, Gandhi KR, Siddiqui AT, Trivedi S, Sinha MB, Rathore M. Crista terminalis, musculi pectinati, and taenia sagittalis: anatomical observations and applied significance. ISRN anatomy. 2013:2013():803853. doi: 10.5402/2013/803853. Epub 2013 Aug 13 [PubMed PMID: 25938104]
Hanaoka T, Suyama K, Taguchi A, Shimizu W, Kurita T, Aihara N, Kamakura S. Shifting of puncture site in the fossa ovalis during radiofrequency catheter ablation: intracardiac echocardiography-guided transseptal left heart catheterization. Japanese heart journal. 2003 Sep:44(5):673-80 [PubMed PMID: 14587649]
Kerut EK, Norfleet WT, Plotnick GD, Giles TD. Patent foramen ovale: a review of associated conditions and the impact of physiological size. Journal of the American College of Cardiology. 2001 Sep:38(3):613-23 [PubMed PMID: 11527606]
Demir T, Oztunç F, Eroğlu AG, Saltik L, Ahunbay G, Kutluğ S, Güzeltaş A, Altun G. Outcome for patients with isolated atrial septal defects in the oval fossa diagnosed in infancy. Cardiology in the young. 2008 Feb:18(1):75-8. doi: 10.1017/S1047951107001692. Epub 2008 Jan 8 [PubMed PMID: 18179730]
Level 2 (mid-level) evidenceAzhari N, Shihata MS, Al-Fatani A. Spontaneous closure of atrial septal defects within the oval fossa. Cardiology in the young. 2004 Apr:14(2):148-55 [PubMed PMID: 15691403]
Level 2 (mid-level) evidenceMcMahon CJ, Feltes TF, Fraley JK, Bricker JT, Grifka RG, Tortoriello TA, Blake R, Bezold LI. Natural history of growth of secundum atrial septal defects and implications for transcatheter closure. Heart (British Cardiac Society). 2002 Mar:87(3):256-9 [PubMed PMID: 11847166]
Level 2 (mid-level) evidenceChaudhari RG, Shinde SV, Deshpande JR. Morphometric analysis of fossa ovalis in rheumatic heart disease. Indian heart journal. 2005 Nov-Dec:57(6):662-5 [PubMed PMID: 16521634]
Level 2 (mid-level) evidenceRoberts WC, Ko JM. Some observations on mitral and aortic valve disease. Proceedings (Baylor University. Medical Center). 2008 Jul:21(3):282-99 [PubMed PMID: 18628928]
Munjewar C, Agrawal R, Sharma S. Cardiac amyloidosis: a report of two cases. Indian heart journal. 2014 Jul-Aug:66(4):473-6. doi: 10.1016/j.ihj.2014.05.028. Epub 2014 Jun 24 [PubMed PMID: 25173210]
Level 3 (low-level) evidenceCohen R, Singh G, Mena D, Garcia CA, Loarte P, Mirrer B. Atrial Myxoma: A Case Presentation and Review. Cardiology research. 2012 Feb:3(1):41-44. doi: 10.4021/cr145w. Epub 2012 Jan 20 [PubMed PMID: 28357024]
Level 3 (low-level) evidenceOnubogu U, West B, Orupabo-Oyan B. Atrial myxoma: a rare cause of hemiplegia in children. Cardiovascular journal of Africa. 2017 Sep/Oct 23:28(5):e1-e3. doi: 10.5830/CVJA-2016-093. Epub 2016 Dec 12 [PubMed PMID: 27942694]
Acebo E, Val-Bernal JF, Gómez-Román JJ. Prichard's structures of the fossa ovalis are not histogenetically related to cardiac myxoma. Histopathology. 2001 Nov:39(5):529-35 [PubMed PMID: 11737312]
Val-Bernal JF, Martino M, Mayorga M, Garijo MF. Prichard's structures of the fossa ovalis are age-related phenomena composed of nonreplicating endothelial cells: the cardiac equivalent of cutaneous senile angioma. APMIS : acta pathologica, microbiologica, et immunologica Scandinavica. 2007 Nov:115(11):1234-40 [PubMed PMID: 18092955]
Edla S, Elsherbiny A, Ravakhah K, Hoit B. Lipomatous Hypertrophy of the Interatrial Septum Presenting with Atrial Arrhythmias. Texas Heart Institute journal. 2015 Aug:42(4):403-4. doi: 10.14503/THIJ-14-4615. Epub 2015 Aug 1 [PubMed PMID: 26413030]
Xanthopoulos A, Giamouzis G, Alexopoulos N, Kitai T, Triposkiadis F, Skoularigis J. Lipomatous Hypertrophy of the Interatrial Septum: A Case Report and Review of the Literature. CASE (Philadelphia, Pa.). 2017 Oct:1(5):182-189. doi: 10.1016/j.case.2017.06.005. Epub 2017 Aug 23 [PubMed PMID: 30062277]
Level 3 (low-level) evidenceRibeiro RNF, Ribeiro BNF, Martins WA, Antunes LO, Marchiori E. Lipomatous hypertrophy of the interatrial septum. Radiologia brasileira. 2018 Mar-Apr:51(2):130-131. doi: 10.1590/0100-3984.2016.0165. Epub [PubMed PMID: 29743748]
Topaz O, Edwards JE, Bojack-Mackey S, Titus JL. Aneurysm of fossa ovalis in adults: a pathologic study. Cardiovascular pathology : the official journal of the Society for Cardiovascular Pathology. 2003 Jul-Aug:12(4):219-25 [PubMed PMID: 12826292]
Katayama H, Mitamura H, Mitani K, Nakagawa S, Ui S, Kimura M. [Incidence of atrial septal aneurysm: echocardiographic and pathologic analysis]. Journal of cardiology. 1990:20(2):411-21 [PubMed PMID: 2104416]
Ruiz de Larrea C, Lasarte JR, Cuadrado A, Pastor E, Galdeano JM, Cabrera A. [Aneurysm of the atrial septum associated with interatrial communication: a study of 12 cases by 2-dimensional color echocardiography]. Revista espanola de cardiologia. 1993 Jun:46(6):340-3 [PubMed PMID: 8316700]
Level 3 (low-level) evidenceMügge A, Daniel WG, Angermann C, Spes C, Khandheria BK, Kronzon I, Freedberg RS, Keren A, Denning K, Engberding R. Atrial septal aneurysm in adult patients. A multicenter study using transthoracic and transesophageal echocardiography. Circulation. 1995 Jun 1:91(11):2785-92 [PubMed PMID: 7758185]
Level 2 (mid-level) evidenceIlercil A, Meisner JS, Vijayaraman P, Gentilucci M, Metveyeva P, Hla A, Strom JA, Chang CJ, Shirani J. Clinical significance of fossa ovalis membrane aneurysm in adults with cardioembolic cerebral ischemia. The American journal of cardiology. 1997 Jul 1:80(1):96-8 [PubMed PMID: 9205032]
Di Pino A, Caruso E, Gitto P. The limbus of the fossa ovalis: an unusual location for incessant focal atrial tachycardia in children. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2016 Aug:18(8):1251. doi: 10.1093/europace/euw047. Epub [PubMed PMID: 27496952]
Bevilacqua LM, Rhee EK, Epstein MR, Triedman JK. Focal ablation of chaotic atrial rhythm in an infant with cardiomyopathy. Journal of cardiovascular electrophysiology. 2000 May:11(5):577-81 [PubMed PMID: 10826938]
Level 3 (low-level) evidenceCheng TO. The proper conduct of Valsalva maneuver in the detection of patent foramen ovale. Journal of the American College of Cardiology. 2005 Apr 5:45(7):1145-6 [PubMed PMID: 15808778]
Level 3 (low-level) evidenceLam YY, Yu CM, Zhang Q, Yan BP, Yip GW. Enhanced detection of patent foramen ovale by systematic transthoracic saline contrast echocardiography. International journal of cardiology. 2011 Oct 6:152(1):24-7. doi: 10.1016/j.ijcard.2010.06.018. Epub 2010 Jul 8 [PubMed PMID: 20619473]
Level 1 (high-level) evidence