Introduction
Endolymph is a physiological fluid that fills the inner ear's labyrinth and serves crucial sensory functions (see Image. The Internal Ear or Labyrinth). Vibrational waves transmitted following the displacement of this fluid from outside stimuli convey information about sound, position, and balance to central sensory neural structures. The endolymph is biochemically specialized and distinct from other central nervous system fluids, such as perilymph and cerebral spinal fluid. Given its crucial role in the sensation and transmission of balance, hearing, and position information, disorders of endolymph have profoundly disabling symptoms, typically hearing loss and vertigo attacks, which can be difficult to diagnose and treat effectively.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Endolymph, or Scarpa fluid, is a clear fluid found in the inner ear's membranous labyrinth. It is unique in composition compared to other extracellular fluids in the body due to its high potassium ion concentration (140 mEq/L) and low sodium ion concentration (15 mEq/L).[1] Many tissues play critical roles in producing and maintaining the ionic composition of endolymph, including the Reissner membrane, stria vascularis, and dark cells of the vestibular organs. Endolymph is separated from surrounding perilymph by the Reissner membrane, which forms a barrier between the 2 fluids.[2] The Reissner membrane allows for selective ion transport and endolymph production from perilymph.[3] Another important tissue involved in endolymph production is the stria vascularis, which is found lining the lateral wall of the cochlear duct. The cells in this tissue help maintain endolymph's high membrane potential and potassium ion concentration.[4] Dark cells in the cristae ampullaris of the semicircular canals use the sodium/potassium ATPase pump to pump potassium into the endolymphatic fluid actively.[5] The ion concentration created and maintained by these various tissues results in endolymph having a high positive potential relative to perilymph. The potential gradient between the 2 fluids allows for increased sensitivity to sound waves, resulting in depolarization and nerve transmission to the brain for interpretation. Many tissues play a role in the regulation and reabsorption of endolymph; however, these processes are not entirely understood.[6] Endolymph serves several important sensory functions based on its interaction with cells in the vestibular apparatus or the cochlear duct. See Image. Endolymph.
Vestibular Apparatus
The vestibular apparatus comprises the utricle, saccule, and 3 semicircular ducts. The acceleration of endolymph within regions of the vestibular apparatus allows for our perception of balance and equilibrium.[7] This occurs through head movement that causes endolymph to move specialized hair cells. Hair cells are arranged in rows and contain "tip-links" that connect them and either depolarize or hyperpolarize afferent nerve fibers based on their direction of movement.[8] Depolarization of hair cells results in an influx of potassium ions from endolymph, leading to calcium channel opening and, subsequently, neurotransmission along nerve fibers. These nerve fibers carry information from different regions of the vestibular apparatus that each plays a unique role in our perception of balance and equilibrium. The saccule and utricle are bones connected to the semicircular ducts that each contain a macula responsible for the perception of linear movement based on endolymph stimulation of hair cells. Likewise, rotational movement is sensed by the semicircular ducts aligned in the lateral, superior, and posterior planes. The ipsilateral semicircular ducts are functionally coupled with the contralateral semicircular ducts to provide feedback on the spatial orientation of the head and equilibrium from endolymph movement via the vestibulocochlear nerve. This relays to the visual system to create the vestibulocochlear reflex, allowing one to keep their eyes fixed on an object while the head moves horizontally.
Cochlear Duct
Endolymph in the cochlear duct plays a very important role in the perception of sound. This occurs when pressure waves travel down the external acoustic meatus and strike the tympanic membrane, causing it to vibrate. These vibrations are transferred to the ossicular chain, consisting of the malleus, incus, and stapes, to the oval window opening to the bony labyrinth vestibule. The stapes footplate transfers these pressure waves to the perilymph and, ultimately, the endolymph. Vibrations in the endolymph stimulate regional hair cells in the organ of Corti based on the vibration frequency, creating a tonotopic map along the cochlea. Based on the region of hair cells stimulated by vibration in the endolymph, nerve impulses are sent to the brain via the cochlear portion of the vestibulocochlear nerve. The brain then interprets these impulses as individual frequencies of sound.[9][10]
Embryology
The inner ear is formed embryologically from ectodermal tissue. The first relevant structure is the preplacodal region, which is an anterior rim of ectodermal tissue along the neural plate. This leads to the formation of the otic placode, which subsequently invaginates to form the otic pit. The otic pit fully invaginates into a closed-off cystic structure known as the otic vesicle, forming the inner ear within the petrous temporal bone.[11] See Image. The Organs of Hearing.
Blood Supply and Lymphatics
The arterial supply to the vestibulocochlear system originates from the posterior circulation of the brain, specifically the basilar artery. The basilar artery forms from the confluence of the bilateral vertebral arteries at the level of the base of the pons. It gives rise to the anterior inferior cerebellar artery, which gives off the internal auditory artery, the labyrinthine artery.[12] The internal auditory artery accompanies the vestibulocochlear nerve through the internal auditory canal. It gives rise to the common cochlear and anterior vestibular arteries to supply the inner ear through a complex network of anastomoses.[13] Furthermore, the subarcuate artery is a second branch from the anterior inferior cerebellar artery, which supplies the vestibule and semicircular canals [12]. The venous drainage of the vestibulocochlear system involves 2 main veins. One of these veins drains the central part of the sensorial areas (maculae plus cristae) and then becomes the vein of the cochlear aqueduct. The other vein drains the peripheral part of the sensorial areas and the simple endolymphatic walls and becomes the vein of the vestibular aqueduct. The latter vein has a close relationship with the endolymphatic sac.[14]
Nerves
Endolymphatic fluid waves generated by mechanical vibrations transmit nerve impulses along the vestibulocochlear nerve, conveying crucial incoming sensory information from the outside world to central neural structures.[10]
Surgical Considerations
Surgery to decompress the endolymphatic sinus or transect the vestibular nerve has been used as a last-resort treatment in patients with refractory Meniere disease.[15]
Clinical Significance
Endolymphatic hydrops
Expansion of the endolymph volume in the endolymphatic space results in the pathological anatomical finding of endolymphatic hydrops.[16] Endolymphatic hydrops can be observed microscopically as an enlargement of the endolymphatic space and distention of the Reissner membrane.[17] It is worth noting that endolymphatic hydrops occur in the presence of volume expansion with a negligible change in pressure in both the endolymph and perilymph. This is due to the high compliance of the endolymphatic boundaries that can accommodate volume increase without an associated substantial pressure increase. The pathophysiology of endolymphatic hydrops was once hypothesized to be a result of impaired flow and reabsorption of endolymph through the endolymphatic sac; however, recent evidence suggests that the volume expansion is the result of ion transport and osmotic gradient dysregulation. This failure of homeostasis is now thought to be associated with hormonal dysregulation of aquaporins that play a role in fluid equilibrium across endolymphatic boundaries.[18]
Endolymphatic hydrops can be diagnosed on MR imaging with specialized sequences termed FLAIR (fluid-attenuated inversion recovery) and REAL-IR (inversion recovery with real reconstruction). These sequences rely on gadolinium contrast infusion either intravenously or into the tympanic space. Because the contrast diffuses into the perilymph but does not diffuse into the endolymph, it is possible to distinguish between these 2 spaces and ascertain if there is a pathological expansion of the latter.[19]
This condition affects the function of the inner ear and is intimately related to the diagnosis of Meniere disease, although the relationship is not always straightforward. Other inner ear disorders may present with endolymphatic hydrops, and studies of patients with clinical signs of Meniere disease have identified a subset that does not have radiological endolymphatic hydrops.[20] Recent experimental evidence has suggested that endolymphatic hydrops alone may not be sufficient to cause Meniere disease alone but that adding other cofactors, including vascular risk factors, may convert this anatomical change into the symptomatic syndrome observed in MD.[21]
Meniere Disease
Meniere disease is a complex disorder of the inner ear with an estimated prevalence of 0.27%, typically affecting people in their 4th and 5th decades of life and with significant deleterious effects on mental health and general quality of life.[22][23] Studies from different parts of the world have demonstrated a sex difference skew toward women to different degrees, most pronounced in a study from Finland, showing a ratio of 4.3 to 1.[24] Furthermore, it is suspected that there may be a genetic component to the disease, although this has not been elucidated with a plausible gene candidate to date.[25] It most commonly affects a unilateral ear but can progress to bilaterally involvement in around 35% of cases.[26] Clinically, Meniere disease presents as a combination of tinnitus, intermittent hearing loss, attacks of vertigo that may last for hours, and the sensation of fullness in the ear.[27] The timeline of symptom onset and progression does not always correlate with the degree of endolymphatic sac distention from endolymphatic hydrops, and a multifactorial interaction likely dictates the onset and progression of the disease.
The diagnosis of Meniere disease can be made using a range of inner ear tests and imaging as well as close observation of the symptomatology experienced by the patient. Typical gold standard testing involves audiometry to assess hearing loss, vestibular evoked myogenic potential (VEMP) testing to assess saccule ad utricle function, caloric testing to assess the vestibulo-ocular reflex, and electrocochleography to record the response to the sound of the middle ear.[28][29][28][30] Furthermore, MR imaging with FLAIR and REAL-IR sequences can aid the diagnosis of endolymphatic hydrops. However, this is not required by current international consensus guidelines. These guidelines suggest that ‘definite’ Meniere disease is defined as the presence of 2 or more spontaneous attacks of vertigo, each with a duration between 20 minutes and 12 hours, alongside fluctuating aural symptoms (defined as heating loss, fullness, and tinnitus), plus audiometric evidence of sensorineural hearing loss in the low- to the midfrequency range.[31]
Treatment of Meniere disease focuses on symptomatic management, principally the recurrent attacks of vertigo, which are acutely disabling. The best current evidence supports using centrally acting anti-histamines with anticholinergic effects.[27] Management of relevant risk factors, including vasculopathy and migraine, may be of benefit.[32] Finally, surgical management options for endolymphatic hydrops are available. The endolymphatic sac decompression by removing part of the petrous bone to allow expansion and placement of a shunt has been used and evaluated in clinical trials but has not been shown to confer any significant lasting benefit.[33] Furthermore, the ablation of inner ear structures such as hair cells, the vestibular nerve, or the labyrinth has been reported with good efficacy, with the rationale that this prevents the ongoing sensation of vertiginous symptoms.[34]
Media
(Click Image to Enlarge)
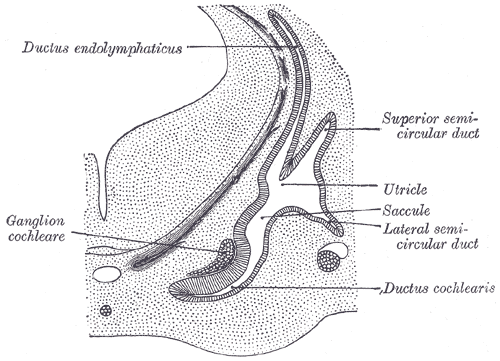
The Organs of Hearing. Transverse section through the head of fetal sheep; in the region of the labyrinth, ductus endolymphaticus, superior semicircular duct, utricle, saccule, lateral semicircular duct, ductus cochlearis, and ganglion cochleare.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
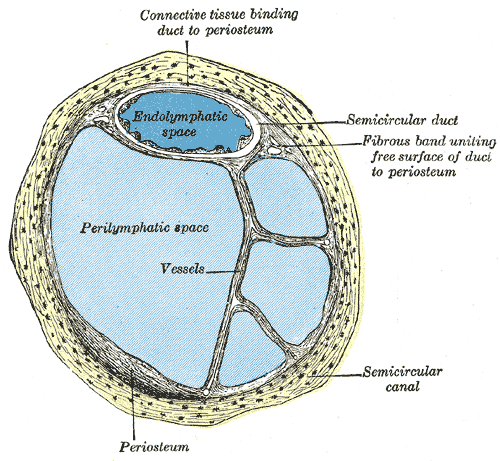
Internal Ear or Labyrinth, Transverse Section. The image is a transverse section of a human semicircular canal and duct, endolymphatic space, perilymphatic space, and a fibrous band uniting the free surface of the duct to the periosteum.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
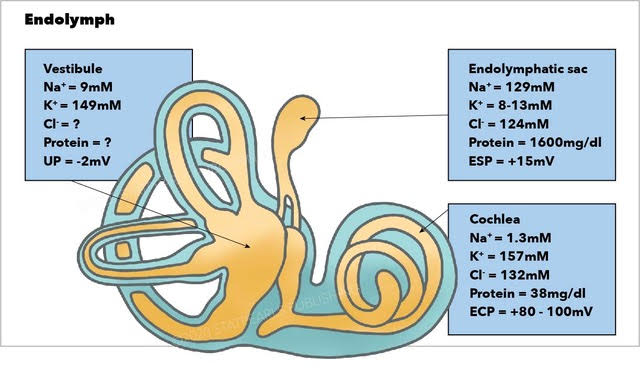
Endolymph. The image depicts the endolymph, vestibule, endolymphatic sac, and cochlea.
Illustration by E Gregory
References
Couloigner V, Teixeira M, Sterkers O, Rask-Andersen H, Ferrary E. [The endolymphatic sac: its roles in the inner ear]. Medecine sciences : M/S. 2004 Mar:20(3):304-10 [PubMed PMID: 15067575]
Shibata T, Matsumoto S, Agishi T, Nagano T. Visualization of Reissner membrane and the spiral ganglion in human fetal cochlea by micro-computed tomography. American journal of otolaryngology. 2009 Mar-Apr:30(2):112-20. doi: 10.1016/j.amjoto.2008.07.012. Epub [PubMed PMID: 19239953]
Köppl C, Wilms V, Russell IJ, Nothwang HG. Evolution of Endolymph Secretion and Endolymphatic Potential Generation in the Vertebrate Inner Ear. Brain, behavior and evolution. 2018:92(1-2):1-31. doi: 10.1159/000494050. Epub 2018 Nov 9 [PubMed PMID: 30415265]
Yu W, Zong S, Du P, Zhou P, Li H, Wang E, Xiao H. Role of the Stria Vascularis in the Pathogenesis of Sensorineural Hearing Loss: A Narrative Review. Frontiers in neuroscience. 2021:15():774585. doi: 10.3389/fnins.2021.774585. Epub 2021 Nov 19 [PubMed PMID: 34867173]
Level 3 (low-level) evidenceCoppens AG, Salmon I, Heizmann CW, Poncelet L. Dark-cell areas in the dog vestibular endorgans: an immunohistochemical study. Histology and histopathology. 2004 Oct:19(4):1227-35. doi: 10.14670/HH-19.1227. Epub [PubMed PMID: 15375766]
Level 3 (low-level) evidenceKurbel S, Borzan V, Golem H, Dinjar K. Cochlear potential difference between endolymph fluid and the hair cell's interior: a retold interpretation based on the Goldman equation. Medicinski glasnik : official publication of the Medical Association of Zenica-Doboj Canton, Bosnia and Herzegovina. 2017 Feb 1:14(1):8-15. doi: 10.17392/868-16. Epub [PubMed PMID: 28165435]
Angelaki DE,Cullen KE, Vestibular system: the many facets of a multimodal sense. Annual review of neuroscience. 2008 [PubMed PMID: 18338968]
Level 3 (low-level) evidenceMcPherson DR. Sensory Hair Cells: An Introduction to Structure and Physiology. Integrative and comparative biology. 2018 Aug 1:58(2):282-300. doi: 10.1093/icb/icy064. Epub [PubMed PMID: 29917041]
Level 2 (mid-level) evidenceKniep R, Zahn D, Wulfes J, Walther LE. The sense of balance in humans: Structural features of otoconia and their response to linear acceleration. PloS one. 2017:12(4):e0175769. doi: 10.1371/journal.pone.0175769. Epub 2017 Apr 13 [PubMed PMID: 28406968]
Iversen MM, Rabbitt RD. Wave Mechanics of the Vestibular Semicircular Canals. Biophysical journal. 2017 Sep 5:113(5):1133-1149. doi: 10.1016/j.bpj.2017.08.001. Epub [PubMed PMID: 28877495]
Whitfield TT. Development of the inner ear. Current opinion in genetics & development. 2015 Jun:32():112-8. doi: 10.1016/j.gde.2015.02.006. Epub 2015 Mar 19 [PubMed PMID: 25796080]
Level 3 (low-level) evidenceSalgado-Lopez L, Leonel LCP, Aydin SO, Peris-Celda M. Surgical Anatomy of the Labyrinthine and Subarcuate Arteries and Clinical Implications. World neurosurgery. 2020 Sep:141():e880-e887. doi: 10.1016/j.wneu.2020.06.083. Epub 2020 Jun 19 [PubMed PMID: 32565373]
Sugita M, Masutani H, Moriguchi M, Matsunaga K, Nakai Y. Distribution of arteries from brain stem to inner ear around the internal auditory canal. Acta oto-laryngologica. Supplementum. 1991:486():45-52 [PubMed PMID: 1842877]
Level 3 (low-level) evidenceHansen JM, Qvortrup K, Friis M. Vestibular tributaries to the vein of the vestibular aqueduct. Acta oto-laryngologica. 2011 Jan:131(1):9-13. doi: 10.3109/00016489.2010.511260. Epub 2010 Oct 19 [PubMed PMID: 20958133]
Level 3 (low-level) evidenceTassinari M, Mandrioli D, Gaggioli N, Roberti di Sarsina P. Ménière's disease treatment: a patient-centered systematic review. Audiology & neuro-otology. 2015:20(3):153-65. doi: 10.1159/000375393. Epub 2015 Mar 31 [PubMed PMID: 25832807]
Level 1 (high-level) evidenceSalt AN,Plontke SK, Endolymphatic hydrops: pathophysiology and experimental models. Otolaryngologic clinics of North America. 2010 Oct [PubMed PMID: 20713237]
Level 3 (low-level) evidenceMinor LB, Schessel DA, Carey JP. Ménière's disease. Current opinion in neurology. 2004 Feb:17(1):9-16 [PubMed PMID: 15090872]
Level 3 (low-level) evidenceShulman A, Goldstein B. Brain and inner-ear fluid homeostasis, cochleovestibular-type tinnitus, and secondary endolymphatic hydrops. The international tinnitus journal. 2006:12(1):75-81 [PubMed PMID: 17147045]
Level 3 (low-level) evidenceDomínguez P,Manrique-Huarte R,Suárez-Vega V,López-Laguna N,Guajardo C,Pérez-Fernández N, Endolymphatic Hydrops in Fluctuating Hearing Loss and Recurrent Vertigo. Frontiers in surgery. 2021 [PubMed PMID: 34136529]
Baráth K, Schuknecht B, Naldi AM, Schrepfer T, Bockisch CJ, Hegemann SC. Detection and grading of endolymphatic hydrops in Menière disease using MR imaging. AJNR. American journal of neuroradiology. 2014 Jul:35(7):1387-92. doi: 10.3174/ajnr.A3856. Epub 2014 Feb 13 [PubMed PMID: 24524921]
Foster CA, Breeze RE. Endolymphatic hydrops in Ménière's disease: cause, consequence, or epiphenomenon? Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2013 Sep:34(7):1210-4. doi: 10.1097/MAO.0b013e31829e83df. Epub [PubMed PMID: 23921917]
Level 1 (high-level) evidenceTyrrell JS, Whinney DJ, Ukoumunne OC, Fleming LE, Osborne NJ. Prevalence, associated factors, and comorbid conditions for Ménière's disease. Ear and hearing. 2014 Jul-Aug:35(4):e162-9. doi: 10.1097/AUD.0000000000000041. Epub [PubMed PMID: 24732693]
Level 2 (mid-level) evidenceTyrrell J, White MP, Barrett G, Ronan N, Phoenix C, Whinney DJ, Osborne NJ. Mental Health and Subjective Well-being of Individuals With Ménière's: Cross-sectional Analysis in the UK Biobank. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2015 Jun:36(5):854-61. doi: 10.1097/MAO.0000000000000732. Epub [PubMed PMID: 25730447]
Level 2 (mid-level) evidenceHavia M, Kentala E, Pyykkö I. Prevalence of Menière's disease in general population of Southern Finland. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2005 Nov:133(5):762-8 [PubMed PMID: 16274806]
Level 2 (mid-level) evidenceHietikko E, Kotimäki J, Okuloff A, Sorri M, Männikkö M. A replication study on proposed candidate genes in Ménière's disease, and a review of the current status of genetic studies. International journal of audiology. 2012 Nov:51(11):841-5. doi: 10.3109/14992027.2012.705900. Epub 2012 Aug 30 [PubMed PMID: 22934933]
Level 2 (mid-level) evidenceHuppert D, Strupp M, Brandt T. Long-term course of Menière's disease revisited. Acta oto-laryngologica. 2010 Jun:130(6):644-51. doi: 10.3109/00016480903382808. Epub [PubMed PMID: 20001444]
Level 2 (mid-level) evidenceNakashima T, Pyykkö I, Arroll MA, Casselbrant ML, Foster CA, Manzoor NF, Megerian CA, Naganawa S, Young YH. Meniere's disease. Nature reviews. Disease primers. 2016 May 12:2():16028. doi: 10.1038/nrdp.2016.28. Epub 2016 May 12 [PubMed PMID: 27170253]
Gonçalves DU, Felipe L, Lima TM. Interpretation and use of caloric testing. Brazilian journal of otorhinolaryngology. 2008 May-Jun:74(3):440-6 [PubMed PMID: 18661020]
Level 1 (high-level) evidenceFife TD, Satya-Murti S, Burkard RF, Carey JP. Vestibular evoked myogenic potential testing: Payment policy review for clinicians and payers. Neurology. Clinical practice. 2018 Apr:8(2):129-134. doi: 10.1212/CPJ.0000000000000430. Epub [PubMed PMID: 29708189]
Gibson WP. The Clinical Uses of Electrocochleography. Frontiers in neuroscience. 2017:11():274. doi: 10.3389/fnins.2017.00274. Epub 2017 May 19 [PubMed PMID: 28634435]
Basura GJ, Adams ME, Monfared A, Schwartz SR, Antonelli PJ, Burkard R, Bush ML, Bykowski J, Colandrea M, Derebery J, Kelly EA, Kerber KA, Koopman CF, Kuch AA, Marcolini E, McKinnon BJ, Ruckenstein MJ, Valenzuela CV, Vosooney A, Walsh SA, Nnacheta LC, Dhepyasuwan N, Buchanan EM. Clinical Practice Guideline: Ménière's Disease. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2020 Apr:162(2_suppl):S1-S55. doi: 10.1177/0194599820909438. Epub [PubMed PMID: 32267799]
Level 1 (high-level) evidenceMonzani D, Barillari MR, Alicandri Ciufelli M, Aggazzotti Cavazza E, Neri V, Presutti L, Genovese E. Effect of a fixed combination of nimodipine and betahistine versus betahistine as monotherapy in the long-term treatment of Ménière's disease: a 10-year experience. Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale. 2012 Dec:32(6):393-403 [PubMed PMID: 23349559]
Level 2 (mid-level) evidencePullens B, Verschuur HP, van Benthem PP. Surgery for Ménière's disease. The Cochrane database of systematic reviews. 2013 Feb 28:2013(2):CD005395. doi: 10.1002/14651858.CD005395.pub3. Epub 2013 Feb 28 [PubMed PMID: 23450562]
Level 1 (high-level) evidenceGreenberg SL, Nedzelski JM. Medical and noninvasive therapy for Meniere's disease. Otolaryngologic clinics of North America. 2010 Oct:43(5):1081-90. doi: 10.1016/j.otc.2010.05.005. Epub [PubMed PMID: 20713246]