Introduction
The orbital cavity drains via a system of venous blood vessels referred to collectively as the ophthalmic veins. The primary ophthalmic veins are the superior ophthalmic vein (SOV) and inferior ophthalmic vein (IOV). Accessory veins include the medial ophthalmic vein and middle ophthalmic vein, which occur in approximately 40% and 1% to 20% of the population, respectively.[1][2][3][4] The ophthalmic veins anastomose with the facial venous system and drain into the cavernous sinus and intracranial veins (Figure 1).[4][5]
Of the ophthalmic veins, the SOV is the largest caliber with the greatest diameter. It originates in the anterior medial orbit from the junction of the supraorbital, supratrochlear, and angular (a branch of the facial vein) veins medial to the superior rectus muscle insertion and posterior to the trochlea. The SOV then travels posteriorly in a diagonal manner (from medial to lateral) coursing inferior to the superior rectus muscle and superior to the optic nerve and ciliary nerves. Once it reaches the lateral edge of the superior rectus muscle posteriorly, the SOV traverses the superior orbital fissure outside of the annulus of Zinn and drains into the cavernous sinus.[4][5]
The IOV originates as a venous plexus between the globe and the inferior rectus muscle near the anteromedial portion of the orbital floor. The IOV often splits into two branches: one exits the orbit via the inferior orbital fissure to drain into the pterygoid venous plexus while the other exits via the superior orbital fissure to empty into either the SOV or the cavernous sinus directly. The cavernous sinus, a component of the dural venous sinus pathway, drains via the superior and inferior petrosal sinuses and the sigmoid sinus into the internal jugular vein.[4][5]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The function of the ophthalmic veins is to drain blood from the eye and orbit, in addition to periocular adnexal tissues and parts of the mid-face, including the glabella and nasal bridge. The tributaries of the SOV include the following: the lacrimal vein, central retinal vein, superior vortex veins, anterior ethmoidal vein, several muscular veins, medial ophthalmic vein, and sometimes the IOV. The tributaries of the IOV include the following: veins from the inferior oblique, inferior rectus, eyelids, and lacrimal sac, and the inferior vortex veins. Blood collected from these tributary vessels then usually drains into the internal jugular vein via the cavernous sinus; however, alternate venous drainage pathways exist in a subset of the population, such as the pterygoid plexus, which drains into either the internal or external jugular vein. The jugular veins deliver blood into the right atrium of the heart by way of the superior vena cava.[4][6]
Embryology
Eye development involves a complex interplay of numerous molecular signals beginning in the third week of embryogenesis.[7] During the seventh week of gestation, the middle dural plexus stem and the anterior portion of the embryonic primary head sinus form the pro-otic sinus, the future cavernous sinus.[8] The primitive maxillary vein drains the optic vesicle into the pro-otic sinus. The SOV develops from the primitive maxillary vein at the ninth week of gestation. It originates from the mesoderm layer and differentiates into the venous vasculature through various molecules, including vascular endothelial growth factor and transforming growth factor β. The embryonic primary head sinus drains the entire head region, including the orbital contents, through the primitive maxillary vein into the anterior cardinal vein, which develops into the internal jugular vein.[9][10]
Blood Supply and Lymphatics
The lymphatic drainage of the periocular adnexa is primarily via the facial lymph nodes (infraorbital, buccinator, and malar groups). The lateral tissue drains into the superficial parotid group of lymph nodes (i.e., preauricular nodes), while the medial tissue drains into the submandibular nodes. This lymph further drains into the deep cervical lymph nodes along the internal jugular vein.
The infraorbital group of lymph nodes is in the infraorbital region, near the medial canthus, tear trough, or nasolabial fold. These lymph nodes collect lymph from the skin and subcutaneous tissues of the medial portion of the eyelids and the medial canthus. The buccinator group of lymph nodes, overlying the buccinator muscle, drains the lower eyelid. The malar group of lymph nodes is often superficial to the malar eminence and drains the eyelids, medial and lateral canthi, and conjunctiva (Figure 2).[11][12]
The post-septal orbit was once thought to be devoid of robust lymphatic drainage. By double staining with 5’-nucleotidase and alkaline phosphatase and using conjunctival lymphatics as a control, Gausas et al. demonstrated the first evidence of numerous lymphatic capillaries in the lacrimal gland and the outer and middle layers of dura mater encapsulating the human optic nerve.[13] Structures in the orbital apex revealed moderate positive staining but did not meet the established morphological criteria of lymphatics. They found no lymphatic vessels within the orbital fat or extraocular muscles.
Nerves
The SOV passes through the superior orbital fissure accompanied by the oculomotor nerve (cranial nerve III), trochlear nerve (cranial nerve IV), ophthalmic division of the trigeminal nerve (cranial nerve V1; including the lacrimal, frontal, and nasociliary branches), abducens nerve (cranial nerve VI), and sympathetic fibers from the cavernous plexus. The IOV has two branches – one passes through the superior orbital fissure, and the other passes through the inferior orbital fissure along with the maxillary division of the trigeminal nerve (cranial nerve V2; including the infraorbital and zygomatic branches) and branches of the pterygopalatine ganglion.[14]
Muscles
As mentioned previously, the SOV runs medial to the tendinous insertion of the superior rectus muscle. The SOV then courses diagonally to the lateral border of the superior rectus in the posterior orbit near the annulus of Zinn. The IOV runs just superior to the inferior rectus muscle.[4]
Physiologic Variants
The ophthalmic veins are less well-defined and have more variability than the arteries of the orbit. For example, the diameter of the SOV ranges from 2 to 10 millimeters. Further, the roots of origin and communicating branches vary occasionally and give rise to the medial ophthalmic vein, which is usually unilateral. The IOV shows a much more variable organization. The length of the IOV is inconsistent in the literature, and it drains through a variety of indirect and direct routes.[4]
Surgical Considerations
Carotid-Cavernous Fistula Embolization (Superior Ophthalmic Vein Approach)
Direct cannulation of the SOV is one important approach to the treatment of indirect carotid-cavernous sinus fistulas. The SOV approach may be considered to access these lesions when standard percutaneous coiling techniques are unsuccessful or anatomically challenging. The surgical technique is briefly described as follows.[15][16][17]
After obtaining informed consent, the patient is brought to the angiography suite and placed in the supine position. The upper eyelid is infiltrated with a local anesthetic, and the face is prepped and draped in the usual sterile fashion for oculoplastic surgery. A #15 blade is used to create a skin incision in the upper eyelid crease. A combination of blunt and sharp dissection is carried down through the orbicularis oculi muscle, and the orbital septum is incised with Westcott scissors or monopolar cautery. The pre-aponeurotic fat is dissected until an arterialized feeder vessel of the SOV is visualized, which can be followed to the main trunk of the SOV. The surgeon then bluntly isolates and exposes the SOV and enters the vessel wall with an angiocatheter. After confirming catheter location, standard endovascular techniques, including coiling and injection of liquid embolic agents, are used to obliterate the cavernous sinus. The SOV is then occluded by suture ligation or bipolar cautery unless the vein is too large and thick-walled, in which case, primary closure is necessary.[16][17] Lastly, the skin incision is closed with the surgeon’s choice of suture material.
In rare cases where the traditional approaches fail, including transvenous access by way of the inferior petrosal sinus and direct cannulation of the SOV as described above, percutaneous puncture of the IOV has been shown to be a safe alternative. In this approach, percutaneous access of the IOV is achieved with the aid of ultrasound guidance or advanced imaging techniques.[18][19] Other non-conventional transvenous access techniques have been described, including through the frontal vein, facial vein, pterygoid plexus, inferior petro-occipital vein, and superficial temporal vein.[19][20][21]
Clinical Significance
Important clinical considerations regarding the ophthalmic veins include the following:
- Carotid-cavernous sinus fistula (CCF): CCF is a rare disorder involving abnormal communication between the cavernous sinus and the carotid arterial system. As the arterial blood flows into the cavernous sinus, the increased pressure causes stasis of venous blood, leading to dilation of the ophthalmic veins—patients present with exophthalmos, ophthalmoplegia, and conjunctival injection. The CCF and dilated ophthalmic veins are viewable on neuroimaging of the orbits. The gold standard for diagnosis and treatment is carotid angiography, although computed tomography angiography is a minimally-invasive alternative for diagnosis only. Treatment via a transarterial approach in direct CCFs is often required to prevent vision loss from elevated intraocular pressure as a result of venous congestion. For indirect CCFs, the preferred treatment is transvenous endovascular embolization. One approach, as outlined above, is the cannulation and ligation of the SOV or IOV under direct visualization.[17][18][22]
- Ophthalmic vein varix: A varix is a rare orbital venous malformation characterized by dilation of thin-walled veins and low blood flow. The inferior ophthalmic venous plexus, in particular, includes many interconnected, narrow valveless veins. Varices are usually present at birth but manifest in young adulthood as diplopia and proptosis during maneuvers that increase venous pressure, such as Valsalva or prone positioning. Over time, there may be paradoxical enophthalmos when the globe retracts as the varix deflates. Imaging, including ultrasound, computed tomography, and magnetic resonance imaging, can be used to detect varices. For symptomatic varices, treatment options include surgical excision with the aid of clips, endovascular coiling, and percutaneous injection of N-butyl cyanoacrylate glue.[23]
- Increased intracranial pressure: Studies have shown that the diameter of the SOV on imaging correlates directly with intracranial pressure. Isolated bilateral dilation of the SOVs may be the initial sign of increased intracranial pressure, which should prompt urgent evaluation.[24]
- Graves' disease: Color doppler ultrasound has been highlighted in the literature for its use in assessing the SOV in Graves' orbitopathy. During the active phase of thyroid eye disease, there is a significant reduction or reversal in SOV blood flow due to orbital congestion and inflammation. The circulation typically returns to normal following successful treatment, which is supported by clinically and radiographically improved signs of orbital congestion.[25][26]
- Mass effect: Orbital pseudotumor is benign, idiopathic orbital inflammation with no identifiable neoplastic or infectious disorder. The mass effect from orbital edema may compress structures of the orbit, leading to occlusion or constriction of the superior ophthalmic veins, causing venous stasis.[27][28] The most common finding is unilateral dilation of the SOV seen on neuroimaging. This elevated superior ophthalmic venous pressure may increase vascular permeability and decrease venous outflow, even causing choroidal detachment in rare cases.[29]
Other Issues
The ophthalmic veins drain the orbital contents and are the link between the facial and intracranial veins. As such, dilation of the ophthalmic veins is an important clinical consideration. The differential diagnosis for dilated ophthalmic veins is broad, with most common pathologies including carotid-cavernous sinus or dural-cavernous sinus fistulas, venous thrombosis, and facial or orbital arteriovenous malformations.[30]
Media
(Click Image to Enlarge)
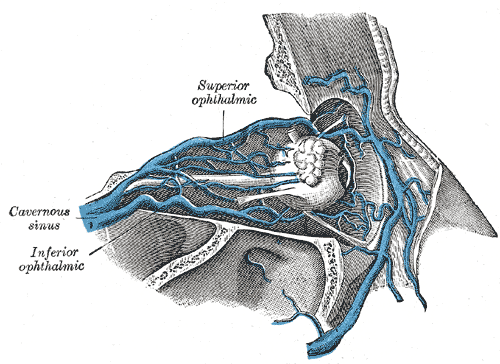
Superior Ophthalmic Vein, Inferior Ophthalmic Vein, and Cavernous Sinus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
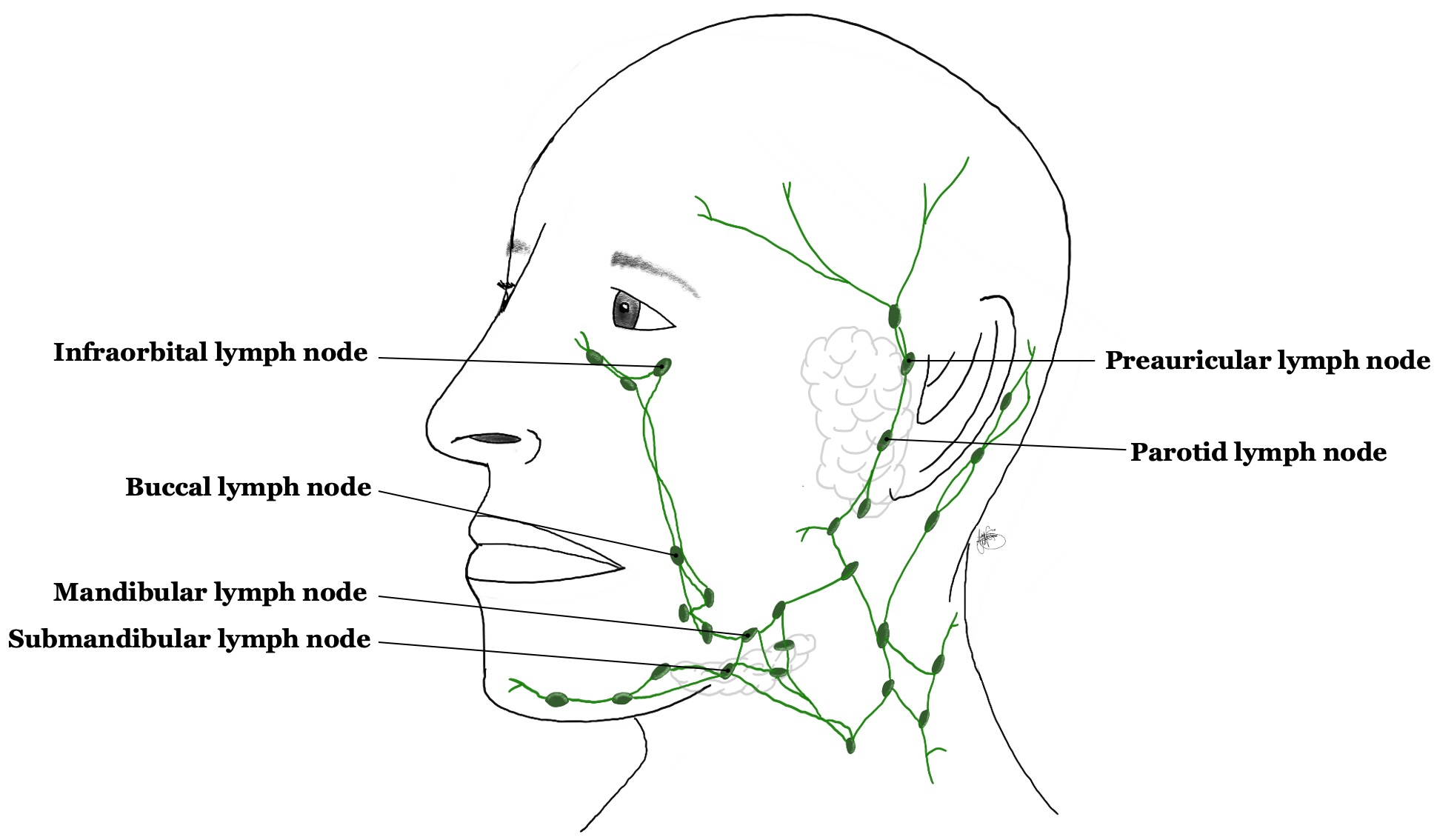
Facial lymph nodes. Lymphatic drainage of the orbit and periocular adnexa occurs by way of the infraorbital, buccinator, and malar groups. Contributed by Ajay Nair Sharma
References
Hayreh SS. Orbital vascular anatomy. Eye (London, England). 2006 Oct:20(10):1130-44 [PubMed PMID: 17019411]
Jo A, Trauzettel H. [Topographic relationships of veins in the orbit]. Verhandlungen der Anatomischen Gesellschaft. 1974:68():539-48 [PubMed PMID: 4467623]
Brismar J. Orbital phlebography. III. Topography of intraorbital veins. Acta radiologica: diagnosis. 1974 Nov:15(6):577-94 [PubMed PMID: 4463695]
Cheung N, McNab AA. Venous anatomy of the orbit. Investigative ophthalmology & visual science. 2003 Mar:44(3):988-95 [PubMed PMID: 12601019]
Bergen MP. A literature review of the vascular system in the human orbit. Acta morphologica Neerlando-Scandinavica. 1981 Dec:19(4):273-305 [PubMed PMID: 7034482]
Brismar J. Orbital phlebography. II. Anatomy of superior ophthalmic vein and its tributaries. Acta radiologica: diagnosis. 1974 Sep:15(5):481-96 [PubMed PMID: 4451136]
Azzam D, Bordoni B. Embryology, Optic Fissure. StatPearls. 2023 Jan:(): [PubMed PMID: 32119320]
Raybaud C. Normal and abnormal embryology and development of the intracranial vascular system. Neurosurgery clinics of North America. 2010 Jul:21(3):399-426. doi: 10.1016/j.nec.2010.03.011. Epub [PubMed PMID: 20561492]
Level 3 (low-level) evidenceMizutani K, Akiyama T, Yoshida K. The remnant of primary head sinus found in the case of dural arteriovenous fistula: A case report. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2016 Aug:22(4):452-6. doi: 10.1177/1591019916641903. Epub 2016 Apr 15 [PubMed PMID: 27084493]
Level 3 (low-level) evidenceTanoue S, Kiyosue H, Okahara M, Sagara Y, Hori Y, Kashiwagi J, Mori H. Para-cavernous sinus venous structures: anatomic variations and pathologic conditions evaluated on fat-suppressed 3D fast gradient-echo MR images. AJNR. American journal of neuroradiology. 2006 May:27(5):1083-9 [PubMed PMID: 16687548]
Tart RP, Mukherji SK, Avino AJ, Stringer SP, Mancuso AA. Facial lymph nodes: normal and abnormal CT appearance. Radiology. 1993 Sep:188(3):695-700 [PubMed PMID: 8351335]
Pan WR, Suami H, Taylor GI. Lymphatic drainage of the superficial tissues of the head and neck: anatomical study and clinical implications. Plastic and reconstructive surgery. 2008 May:121(5):1614-1624. doi: 10.1097/PRS.0b013e31816aa072. Epub [PubMed PMID: 18453984]
Gausas RE, Gonnering RS, Lemke BN, Dortzbach RK, Sherman DD. Identification of human orbital lymphatics. Ophthalmic plastic and reconstructive surgery. 1999 Jul:15(4):252-9 [PubMed PMID: 10432521]
Shumway CL, Motlagh M, Wade M. Anatomy, Head and Neck, Orbit Bones. StatPearls. 2023 Jan:(): [PubMed PMID: 30285385]
Shah A, Patel BC. Superior Ophthalmic Vein Cannulation for Carotid Cavernous Fistula. StatPearls. 2023 Jan:(): [PubMed PMID: 30725862]
Miller NR, Monsein LH, Debrun GM, Tamargo RJ, Nauta HJ. Treatment of carotid-cavernous sinus fistulas using a superior ophthalmic vein approach. Journal of neurosurgery. 1995 Nov:83(5):838-42 [PubMed PMID: 7472552]
Chalouhi N, Dumont AS, Tjoumakaris S, Gonzalez LF, Bilyk JR, Randazzo C, Hasan D, Dalyai RT, Rosenwasser R, Jabbour P. The superior ophthalmic vein approach for the treatment of carotid-cavernous fistulas: a novel technique using Onyx. Neurosurgical focus. 2012 May:32(5):E13. doi: 10.3171/2012.1.FOCUS123. Epub [PubMed PMID: 22537122]
Level 2 (mid-level) evidenceCecchini MM, Levitt MR, Taneja M, Hallam DK, Ghodke BV. Embolization of carotid-cavernous fistula via direct percutaneous puncture of the inferior ophthalmic vein. Journal of neuroradiology = Journal de neuroradiologie. 2012 Jul:39(3):181-5. doi: 10.1016/j.neurad.2011.05.007. Epub 2011 Jul 23 [PubMed PMID: 21783255]
Level 3 (low-level) evidenceMorton RP, Tariq F, Levitt MR, Nerva JD, Mossa-Basha M, Sekhar LN, Kim LJ, Hallam DK, Ghodke BV. Radiographic and clinical outcomes in cavernous carotid fistula with special focus on alternative transvenous access techniques. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2015 May:22(5):859-64. doi: 10.1016/j.jocn.2014.11.006. Epub 2015 Feb 11 [PubMed PMID: 25682541]
Level 2 (mid-level) evidenceMatsubara S, Kazekawa K, Aikawa H, Onizuka M, Tsutsumi M, Ikou M, Kodama T, Nii K, Nagata S, Tanaka A. Direct superficial temporal vein approach for dural carotid cavernous fistula. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2007 Mar 15:13 Suppl 1(Suppl 1):64-7 [PubMed PMID: 20566079]
Kurata A, Suzuki S, Iwamoto K, Nakahara K, Inukai M, Niki J, Satou K, Yamada M, Fujii K, Kan S, Katsuta T. A new transvenous approach to the carotid-cavernous sinus via the inferior petrooccipital vein. Journal of neurosurgery. 2012 Mar:116(3):581-7. doi: 10.3171/2011.4.JNS102155. Epub 2011 Jun 17 [PubMed PMID: 21682561]
Level 3 (low-level) evidenceZhu L, Liu B, Zhong J. Post-traumatic right carotid-cavernous fistula resulting in symptoms in the contralateral eye: a case report and literature review. BMC ophthalmology. 2018 Jul 25:18(1):183. doi: 10.1186/s12886-018-0863-6. Epub 2018 Jul 25 [PubMed PMID: 30045703]
Level 3 (low-level) evidencePappas A, Araque JM, Sarup V. Orbital Venous Varices: A Rare Bilateral Asymptomatic Presentation. Cureus. 2018 Sep 14:10(9):e3302. doi: 10.7759/cureus.3302. Epub 2018 Sep 14 [PubMed PMID: 30705795]
Lirng JF, Fuh JL, Wu ZA, Lu SR, Wang SJ. Diameter of the superior ophthalmic vein in relation to intracranial pressure. AJNR. American journal of neuroradiology. 2003 Apr:24(4):700-3 [PubMed PMID: 12695206]
Sorrentino D, Taubenslag KJ, Bodily LM, Duncan K, Stefko T, Yu JY. Superior ophthalmic vein thrombosis: A rare complication of Graves' orbitopathy. Orbit (Amsterdam, Netherlands). 2018 Jun:37(3):175-178. doi: 10.1080/01676830.2017.1383467. Epub 2017 Oct 20 [PubMed PMID: 29053044]
Monteiro ML, Moritz RB, Angotti Neto H, Benabou JE. Color Doppler imaging of the superior ophthalmic vein in patients with Graves' orbitopathy before and after treatment of congestive disease. Clinics (Sao Paulo, Brazil). 2011:66(8):1329-34 [PubMed PMID: 21915479]
Level 2 (mid-level) evidenceRonquillo Y, Zeppieri M, Patel BC. Nonspecific Orbital Inflammation. StatPearls. 2025 Jan:(): [PubMed PMID: 31869057]
Wilner HI, Gupta KL, Kelly JK. Orbital pseudotumor: association of orbital vein deformities and myositis. AJNR. American journal of neuroradiology. 1980 Jul-Aug:1(4):305-9 [PubMed PMID: 6779606]
Kwon JM, Lee SJ. Kissing Choroidal Detachment in a Patient with Idiopathic Orbital Inflammatory Syndrome. Korean journal of ophthalmology : KJO. 2019 Aug:33(4):386-388. doi: 10.3341/kjo.2018.0090. Epub [PubMed PMID: 31389216]
Adam CR, Shields CL, Gutman J, Kim HJ, Hayek B, Shore JW, Braunstein A, Levin F, Winn BJ, Vrcek I, Mancini R, Linden C, Choe C, Gonzalez M, Altschul D, Ortega-Gutierrez S, Paramasivam S, Fifi JT, Berenstein A, Durairaj V, Shinder R. Dilated Superior Ophthalmic Vein: Clinical and Radiographic Features of 113 Cases. Ophthalmic plastic and reconstructive surgery. 2018 Jan/Feb:34(1):68-73. doi: 10.1097/IOP.0000000000000872. Epub [PubMed PMID: 28141624]
Level 3 (low-level) evidence