Introduction
Ultrasound is an imaging modality that has been in clinical use for approximately 50 years. Sokolov first described the potential for using this technology to produce low-resolution images in 1939. Later understanding of the piezoelectric effect and further technological refinements have resulted in machine advancements. We have seen the machine sizes dramatically decrease; some of the earliest machines were the size of refrigerators while recently we have seen the introduction of transducers that are compatible with smartphones. Although ultrasound technology can be utilized in a variety of different settings and body locations, the focus of this article will be on transabdominal ultrasound, its definition, indications and diagnostic pearls and pitfalls.[1][2]
Transabdominal ultrasound was initially utilized in its most colloquial setting of pregnancy in the 1960s.[3][4] It is now utilized for visualization of multiple abdominal organs, both intraperitoneal and retroperitoneal. By definition, any evaluation with an ultrasound transducer overlying the abdominal wall can be considered a transabdominal ultrasound. Transabdominal ultrasound can be applied to visualize the liver, gallbladder[5], kidneys, pancreas, small and large intestine, appendix, bladder, uterus, adnexa, spleen, stomach, aorta, and IVC. In the setting of obstetrics and gynecology (OBGYN), the transabdominal approach is usually performed to evaluate for possible pelvic pathology or pregnancy in a less invasive manner. In the emergency department (ED) a transabdominal ultrasound is most commonly utilized to evaluate for intrauterine pregnancy[6], cholelithiasis, intraabdominal free fluid, abdominal aortic aneurysm, and hydronephrosis.
Emergency physicians (EPs) perform a limited point-of-care ultrasound (POCUS) in comparison to formal radiology transabdominal ultrasounds. The EP performs the former compared to the latter, and a trained sonographer performs a thorough and complete examination of the organ. ED POCUS is focused on binary questions that are rapidly evaluated at the bedside and direct patient care immediately. For example: “Is there an intrauterine pregnancy?” In most cases when an intrauterine pregnancy is identified, the examination is complete. While both EPs and sonographers perform a transabdominal ultrasound, the performance characteristics and goals vary.[7]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Sonographic anatomy, similar to gross anatomy, recognizes landmarks and scanning conventions that were originally defined by specialties like obstetrics and radiology. For example, the gallbladder is located under the liver and has great variability with its location. The sonographic cystic pedicle (SCP) is a landmark utilized to ensure correct identification of the gallbladder.[8] Originally this was called the main lobar fissure (MLF), which was thought to correlate to the main portal fissure. Cadaveric dissection later found this to be an extrahepatic structure paralleling the rim of the main lobar fissure and was re-named the SCP, which includes the cystic duct, ensheathing fat and blood vessels. Each organ of interest has its varying anatomy and ultrasound scanning convention to acquire the desired image or measurements needed to identify pathology.
Indications
Abdominal Pain
Right Upper Quadrant[9]: Evaluation for free fluid, cholelithiasis, choledocholithiasis, hepatic abscess mass, hydronephrosis
Right Lower Quadrant: Evaluation for appendicitis[10], intussusception, psoas abscess
Left Upper Quadrant: Evaluation for free fluid, splenic pathology (laceration or fracture), stomach, hydronephrosis
Left Lower Quadrant: Evaluation for diverticulitis, small bowel obstruction[11]
Epigastric: Evaluation for pancreatic mass, abdominal aortic aneurysm
Pelvic: Evaluation for free fluid, urinary retention, pregnancy, ectopic pregnancy, pelvic mass
Blunt or Penetrating Abdominal Trauma
- Evaluation of free fluid[12]
Vaginal Bleeding
- Evaluation for pregnancy, ectopic pregnancy, uterine pathology, abortion (fetal parts)
Hypotension:
- Evaluation for infectious sources listed above, vascular assessment of inferior vena cava as a surrogate marker for volume status or volume loss from hemorrhage[13], abdominal aortic aneurysm
Hematuria
- Evaluation for genitourinary mass, nephrolithiasis, hydronephrosis
Contraindications
There are no absolute contraindications to performing a transabdominal ultrasound. One should take care not to scan over a wound or incision to avoid contamination and infection. Color and pulsed Doppler should not be applied to a fetus because of the theoretical radiation risk to the fetus.[14]
Equipment
Transabdominal ultrasound should be performed with a low-frequency probe, ideally with a large convex footprint. Most common probes utilized are the curvilinear or phased array probes. Disinfectant wipes and cleaning equipment are institution specific and usually determined by the infectious disease department.
Personnel
A trained provider can perform a transabdominal ultrasound. Registered diagnostic medical sonographer (RDMS) have different requirements and certification than most primary providers performing a point-of-care ultrasound at the bedside. For example, emergency physicians are required to perform and interpret a minimum of 25 to 50 cardiac ultrasound exams upon residency graduation.
Preparation
Ensure that the probe and machine are cleaned before entering a patient room. The correct probes should be connected to the machine. The patient is ideally lying in a supine position on a stretcher with his or her abdomen exposed. Care should be taken to avoid unnecessary exposure with the use of towels tucked around the gown and undergarment edges. This will also aid in keeping unexposed areas clean from ultrasound gel.
For dominant right-hand operators, the ultrasound machine should be positioned at the patient’s anatomic right near the head of the bed, plugged in (if applicable) and turned on. The lights should be dimmed if possible. For evaluation of the gallbladder, being in a fasting state aids in the engorgement of the gallbladder and better visualization. When evaluating the uterus, informing the patient to maintain a full bladder will aid in visualization secondary to fluid in the bladder providing an acoustic window to deeper structures.
Technique or Treatment
A low-frequency convex probe is best for a transabdominal ultrasound. Alternatively, a phased array probe can be used if a convex probe is not available. The settings on the ultrasound machine should be set to the desired exam being performed, for example, abdominal, FAST, vascular. The settings on the machine optimize image quality for the scan being performed. Generally, the probe indicator is always aimed cephalad (toward the patient’s head) or to the patient’s right side. Specific scanning technique is utilized depending on the organ or pathology being evaluated. For example, when evaluating the gallbladder, the probe is placed in a sagittal plane (with the indicator cephalad) in the right upper quadrant just inferior to the costal margin. The operator then slides the probe medial and lateral along the costal margin while maintaining the sagittal plane (cephalad) evaluating for the optimal sonographic window for image acquisition. Asking the patient to take a deep breath and hold it causes the diaphragm to contract, displacing the liver and gallbladder inferior, and aiding in image acquisition. A coronal scan of the right upper quadrant is another technique that can allow for gallbladder evaluation. With the probe placed on the patient’s right in the mid-axillary line, indicator cephalad, the operator can then fan the probe anterior and posterior through the liver in an attempt to acquire an optimal window to evaluate the gallbladder. The gallbladder is then evaluated for (1) stones or sludge, (2) wall thickening (normal less than 3 mm), (3) presence of a sonographic Murphy's sign, and (4) pericholecystic fluid.[15] The presence of all four is very sensitive and specific for cholecystitis. This is an example of one specific area of transabdominal ultrasound. There are specific techniques for most abdominal organs and underlying pathologies that can be evaluated using ultrasound.
Complications
Transabdominal ultrasound, like most diagnostic ultrasound applications, is associated with little if any risk. There may be some associated discomfort when pressure is applied.
Clinical Significance
Transabdominal ultrasound is an inexpensive, safe, rapid way of assessing for multiple pathologies. It can be used to effectively rule in or out specific pathologies such as cholecystitis without the need for further imaging in many cases. This can lead to expedited diagnosis, treatment, and a reduction in ionizing radiation.
Enhancing Healthcare Team Outcomes
It is the healthcare providers responsibility to decrease the harm caused by ionizing radiation. ALARA principle supported by the US-Nuclear Regulatory Commission and the Centers for Disease Control and Prevention (CDC).[16][17]
Media
(Click Image to Enlarge)
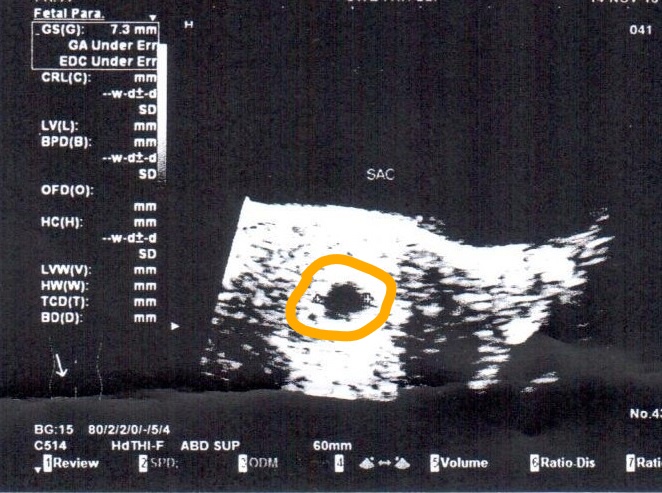
Final Transabdominal Ultrasound at 8 weeks, shows gestational sac 7.3 mm with no fetus Contributed by Tripthi M. Mathew, MD, MPH, MBA, PhD.
References
Russell TC, Crawford PF. Ultrasound in the austere environment: a review of the history, indications, and specifications. Military medicine. 2013 Jan:178(1):21-8 [PubMed PMID: 23356114]
Whitson MR, Mayo PH. Ultrasonography in the emergency department. Critical care (London, England). 2016 Aug 15:20(1):227. doi: 10.1186/s13054-016-1399-x. Epub 2016 Aug 15 [PubMed PMID: 27523885]
Benson CB,Doubilet PM, The history of imaging in obstetrics. Radiology. 2014 Nov [PubMed PMID: 25340440]
Schillinger H, Müller R, Kretzschmar M, Wode J. [Estimation of fetal weight by ultrasound (author's transl)]. Geburtshilfe und Frauenheilkunde. 1975 Nov:35(11):858-65 [PubMed PMID: 1193357]
Revzin MV, Scoutt LM, Garner JG, Moore CL. Right Upper Quadrant Pain: Ultrasound First! Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2017 Oct:36(10):1975-1985. doi: 10.1002/jum.14274. Epub 2017 Jun 6 [PubMed PMID: 28586152]
Sohoni A, Bosley J, Miss JC. Bedside ultrasonography for obstetric and gynecologic emergencies. Critical care clinics. 2014 Apr:30(2):207-26, v. doi: 10.1016/j.ccc.2013.10.002. Epub 2013 Dec 12 [PubMed PMID: 24606774]
Blanco P,Volpicelli G, Common pitfalls in point-of-care ultrasound: a practical guide for emergency and critical care physicians. Critical ultrasound journal. 2016 Dec [PubMed PMID: 27783380]
Hall MK, Mirjalili SA, Moore CL, Rizzolo LJ. The student's dilemma, liver edition: incorporating the sonographer's language into clinical anatomy education. Anatomical sciences education. 2015 May-Jun:8(3):283-8. doi: 10.1002/ase.1518. Epub 2015 Jan 8 [PubMed PMID: 25573229]
Joshi G, Crawford KA, Hanna TN, Herr KD, Dahiya N, Menias CO. US of Right Upper Quadrant Pain in the Emergency Department: Diagnosing beyond Gallbladder and Biliary Disease. Radiographics : a review publication of the Radiological Society of North America, Inc. 2018 May-Jun:38(3):766-793. doi: 10.1148/rg.2018170149. Epub [PubMed PMID: 29757718]
Matthew Fields J, Davis J, Alsup C, Bates A, Au A, Adhikari S, Farrell I. Accuracy of Point-of-care Ultrasonography for Diagnosing Acute Appendicitis: A Systematic Review and Meta-analysis. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2017 Sep:24(9):1124-1136. doi: 10.1111/acem.13212. Epub 2017 Aug 21 [PubMed PMID: 28464459]
Level 1 (high-level) evidenceTaylor MR,Lalani N, Adult small bowel obstruction. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2013 Jun [PubMed PMID: 23758299]
Level 1 (high-level) evidenceWilliams SR, Perera P, Gharahbaghian L. The FAST and E-FAST in 2013: trauma ultrasonography: overview, practical techniques, controversies, and new frontiers. Critical care clinics. 2014 Jan:30(1):119-50, vi. doi: 10.1016/j.ccc.2013.08.005. Epub [PubMed PMID: 24295843]
Level 3 (low-level) evidenceCiozda W, Kedan I, Kehl DW, Zimmer R, Khandwalla R, Kimchi A. The efficacy of sonographic measurement of inferior vena cava diameter as an estimate of central venous pressure. Cardiovascular ultrasound. 2016 Aug 20:14(1):33. doi: 10.1186/s12947-016-0076-1. Epub 2016 Aug 20 [PubMed PMID: 27542597]
Kurjak A. Are color and pulsed Doppler sonography safe in early pregnancy? Journal of perinatal medicine. 1999:27(6):423-30 [PubMed PMID: 10732300]
Woo MY, Taylor M, Loubani O, Bowra J, Atkinson P. My patient has got abdominal pain: identifying biliary problems. Ultrasound (Leeds, England). 2014 Nov:22(4):223-8. doi: 10.1177/1742271X14546181. Epub 2014 Aug 4 [PubMed PMID: 27433223]
Shah NB, Platt SL. ALARA: is there a cause for alarm? Reducing radiation risks from computed tomography scanning in children. Current opinion in pediatrics. 2008 Jun:20(3):243-7. doi: 10.1097/MOP.0b013e3282ffafd2. Epub [PubMed PMID: 18475090]
Level 3 (low-level) evidenceBello SO, Ekele BA. On the safety of diagnostic ultrasound in pregnancy: have we handled the available data correctly? Annals of African medicine. 2012 Jan-Mar:11(1):1-4. doi: 10.4103/1596-3519.91006. Epub [PubMed PMID: 22199039]