Introduction
The femoral sheath is a fascial tube encapsulating the key vascular structures passing through the retro-inguinal space, a critical transition point between the abdomen and the anterior thigh compartment. It is an important anatomical landmark for understanding the structures in the femoral triangle within which it lies and has clinical importance as the site of femoral hernias.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The inguinal ligament spans the gap between the anterior superior iliac spine and the pubic tubercle. Beneath it, the retro-inguinal space is created and is divided by the iliopectineal arch into a muscular compartment and a vascular compartment. The femoral sheath lines the vascular compartment of the retro-inguinal space, which contains the femoral artery, femoral vein, and deep inguinal lymph nodes.[2]
The femoral sheath has a conical shape and is of varying length, typically 3 to 4 cm, before it blends with the adventitia of the femoral vessels. Its anterior aspect is a continuation of the transversalis fascia, whereas the posterior aspect is formed from a continuation of the iliopsoas fascia.[3]
Anteriorly, the femoral sheath is covered by the fascia lata of the thigh, and posteriorly it is related to the underlying iliacus and pectineus muscles. The femoral sheath is bordered medially by the lacunar ligament, and on its lateral side lies the femoral nerve.
The femoral sheath is divided into three compartments by vertical septa of connective tissue that separate it into distinct functional areas:
- Lateral compartment – containing the femoral artery
- Intermediate compartment – containing the femoral vein
- Medial compartment – called the femoral canal, containing loose connective tissue and lymph nodes[4]
The function of the femoral canal (medial compartment of the femoral sheath) is to allow expansion of the femoral vein into this space following increased venous return.[5] The superior opening of the femoral canal under the inguinal ligament is termed the femoral ring. The borders of the femoral ring are:
- Anteriorly: the inguinal ligament
- Medially: the lacunar ligament
- Laterally: the septum between the femoral canal and the intermediate compartment of the femoral sheath
- Posteriorly: Pectineus muscle[3]
The ‘mouth’ of the femoral ring is covered transversely by a sheet of peritoneal fatty tissue termed the femoral septum; this area is weak and abdominal viscera can traverse through it into the femoral canal, causing a femoral hernia.[2][4]
The general function of the femoral sheath is to allow the femoral vascular structures to glide underneath the inguinal ligament during hip flexion and extension. It provides a smooth fascial layer to facilitate this.
Embryology
The femoral sheath is a fascial structure formed anteriorly by a continuation of the transversalis fascia and posteriorly by a continuation of the iliopsoas fascia. Both of these fascia layers are part of the thoracolumbar fascia, which is key to maintaining posture and the transmission of force between the scapular and pelvic girdles.[6] The embryological origin of the fascial layers of the body is intimately associated with the development of their corresponding muscular structures. Somitogenesis begins on the twentieth day of the embryo, forming somites from the segmentation of the paraxial mesoderm.[7] The dermomyotome is one of the constituent parts of the resulting somite, alongside the sclerotome. Further differentiation of the dermomyotome forms the dermis of the skin, as well as the epaxial and the hypaxial muscle compartments, the latter of which include the ventrolateral muscles of the abdominal wall.[8]
Blood Supply and Lymphatics
The femoral artery travels in the lateral compartment of the femoral sheath. It is a continuation of the external iliac artery, commencing as it passes under the inguinal ligament.[9] Distally, the femoral artery passes into the adductor canal, becoming the popliteal artery as it passes through the adductor hiatus. It gives off several important branches, none of which arise within the femoral sheath itself.
The femoral vein occupies the intermediate compartment of the femoral sheath. It is a continuation of the popliteal vein and enters the femoral sheath before becoming the external iliac vein as it passes under the inguinal ligament.
The femoral canal contains deep inguinal lymph nodes and associated lymphatic vessels.[10] The superior-most lymph node is termed the node of Cloquet.[11] These lymph nodes drain the glans clitoris in females, and the glans penis and the distal part of the spongy urethra in males.
Nerves
The femoral branch of the genitofemoral nerve (from L1-L2) is given off as it lies on psoas major. It then runs inferiorly under the inguinal ligament, accompanying the femoral artery in the lateral compartment of the femoral sheath, before piercing it anteriorly to innervate the skin over the femoral triangle.[12][13]
The femoral nerve proper (from L2-L4) travels in the muscular compartment of the retro-inguinal space, lateral to the vascular compartment lined by the femoral sheath.[14] Thus, although an important part of the femoral triangle anatomy, it does not form part of the femoral sheath.
Muscles
Behind the femoral sheath are the pectineus muscle (posteromedial) and the iliopsoas muscle (posterolateral).[2] The origin of the pectineus muscle is the pectineal line of the pubis, and its distal insertion point is the pectineal line of the femur, which is a continuation from the inferior part of the lesser trochanter. The iliopsoas muscle is a congruence of two posterior abdominal wall muscles; the iliacus, which arises from the iliac fossa, and the psoas major, which arises from the transverse processes of lumbar vertebrae L1-L5. Together, as the iliopsoas muscle, it inserts at the lesser trochanter of the femur. There is no muscular covering anteriorly over the femoral sheath; instead, it is covered by the fascia lata and cribriform fascia, subcutaneous tissue, and skin.
Surgical Considerations
The medial part of the femoral sheath, termed the femoral canal, is the site through which abdominal viscera can protrude, resulting in a femoral hernia. Femoral hernia repair can be performed with mesh (hernioplasty) or primary suture closure (herniorrhaphy). Modern practice internationally has favored mesh repair, either via an open approach or laparoscopically, in the elective setting for both male and female groin hernia repair.[15][1] However, controversy remains as to the best management for femoral hernias.[16][17][18][19] This is because they are far less common than inguinal hernias, and there is a lack of long-term outcome data from the various repair techniques.[20]
The three classic open approaches to repair of femoral hernia are the infra-inguinal (Lockwood) approach, the trans-inguinal (Lotheissen) approach, and the high (McEvedy) approach, with each offering advantages in certain situations. The Lockwood approach, for example, involves a parallel incision approximately 1cm below the inguinal ligament and is suitable for elective repair as there is little opportunity to allow for bowel resection if required in emergency surgery[21]. Contemporary surgical practice has moved towards the laparoscopic approach for elective repair of femoral hernia, however, with classic open approaches increasingly being superseded. Indeed, the laparoscopic approach is increasingly recognized also as an option for emergency repair.[22]
The two laparoscopic surgical techniques for groin hernias are the transabdominal preperitoneal (TAPP) and the totally intraperitoneal (TEP) approach.[23] In the former, the peritoneal cavity is entered, and an incision is made pre-peritoneally to enable repair of the herniated site, whereas, in TEP, the peritoneum remains intact, and repair is performed without entering the cavity[24]. Current evidence involving a meta-analysis of 15 randomized-control trials suggests the recurrence rate and long-term outcomes of the two techniques are comparable.[25]
Clinical Significance
Femoral Hernia
Femoral hernias are the least common kind of groin hernia, accounting for between 20% and 31% of groin repairs in women and only 1% of groin repairs in men.[26] There is a strong preponderance towards women, with one study identifying 88% of femoral hernias as presenting in women, and the average age of presentation is typically in the 6th to 7th decade.[27] However, they may be underdiagnosed, particularly in patients with a high body-mass index (BMI); one study reported that 37% of women undergoing endoscopic inguinal hernia repair were found to have a synchronous undiagnosed femoral hernia.[28]
The typical clinical presentation of femoral hernia is a swelling inferior to the inguinal ligament and inferior and lateral to the pubic tubercle.[1] The risk of strangulation in femoral hernia is higher than for inguinal hernia.[26] Incarcerated bowel within a strangulated femoral hernia may present with severe pain and an acute bowel obstruction requiring emergent surgical intervention, and this is associated with worse outcomes than in patients managed electively.[29][30]
Femoral Vascular Access
The femoral vein is a relatively safe option for gaining central venous access when more proximal locations are less easily accessible. Ultrasound guidance helps reduce vascular bleeding by 60% when used for femoral vein cannulation.[31][32] The femoral artery is also a commonly used site of arterial access, both for obtaining blood in emergency situations and diagnostic procedures, such as digital subtraction angiography in neurosurgery.[33][34]
Node of Cloquet
The node of Cloquet, which lies within the medial compartment of the femoral sheath (otherwise known as the femoral canal), is the junctional point between the external iliac lymph chain and the deep inguinal nodes.[35] As such, it is the sentinel node for the iliac and obturator lymphatic system. Studies investigating the predictive value of metastatic deposits in Cloquet's node for deep pelvic malignancy have shown a positive predictive value of 70% and a negative predictive value of 84%.[11] This means that the decision on whether to perform deep pelvic lymphadenectomy can potentially be made based on a sentinel node biopsy of the node of Cloquet.[11] A further study found the pathological status of Cloquet's node to be superior to the radiological diagnosis when determining the appropriate extent of lymph node dissection that should be undertaken in patients with lower limb melanoma and palpable inguinal lymphadenopathy.[36]
Media
(Click Image to Enlarge)
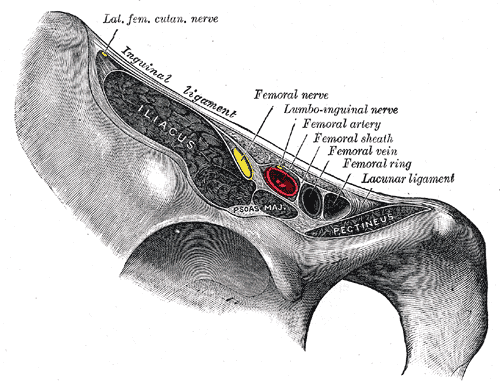
Vascular Lacuna, Femoral Nerve, Ilioinguinal nerve, Femoral sheath, Femoral artery, Femoral vein and ring
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
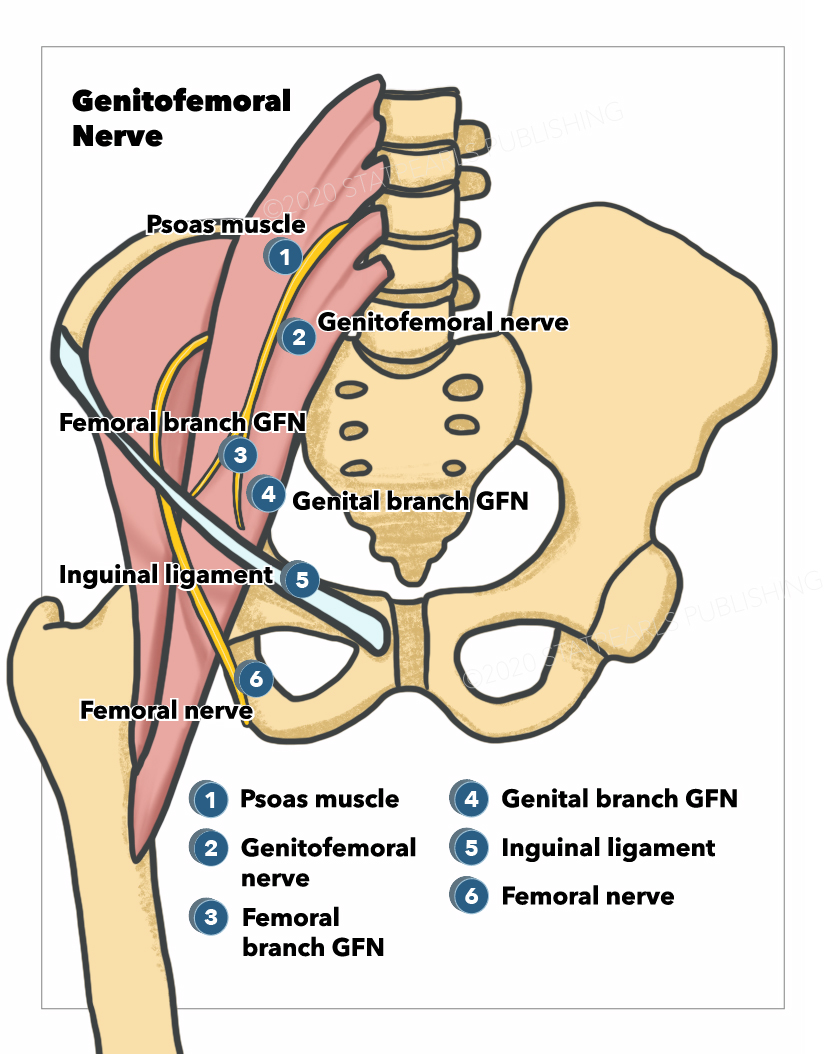
Genitofemoral Nerve. The genitofemoral nerve arises from the lumbar plexus and supplies sensation to the thigh and genitalia.
Illustration by E Gregory
(Click Image to Enlarge)
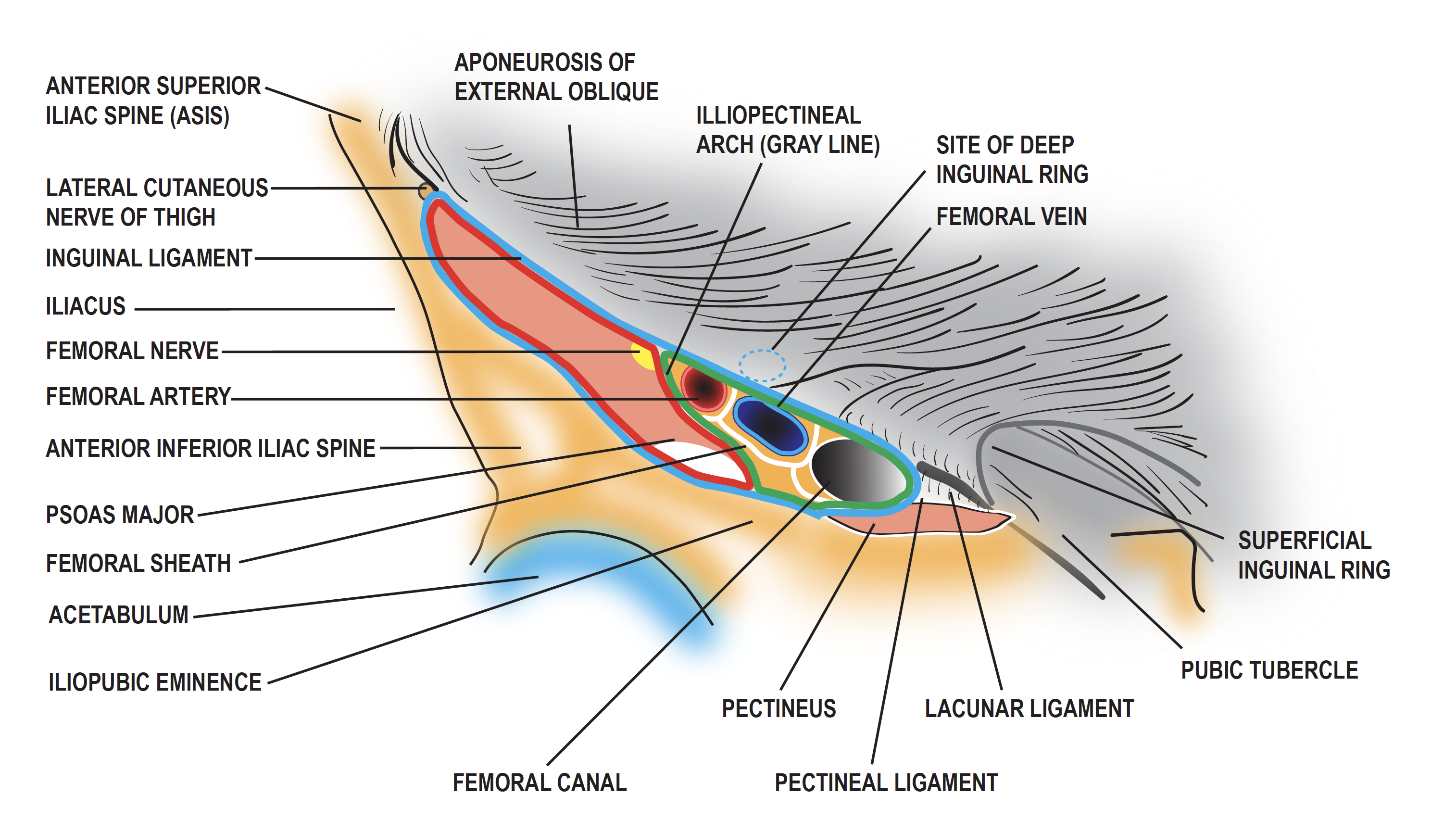
Diagram of the femoral sheath and its contents. Contributed by Penney Dellavalle
(Click Image to Enlarge)
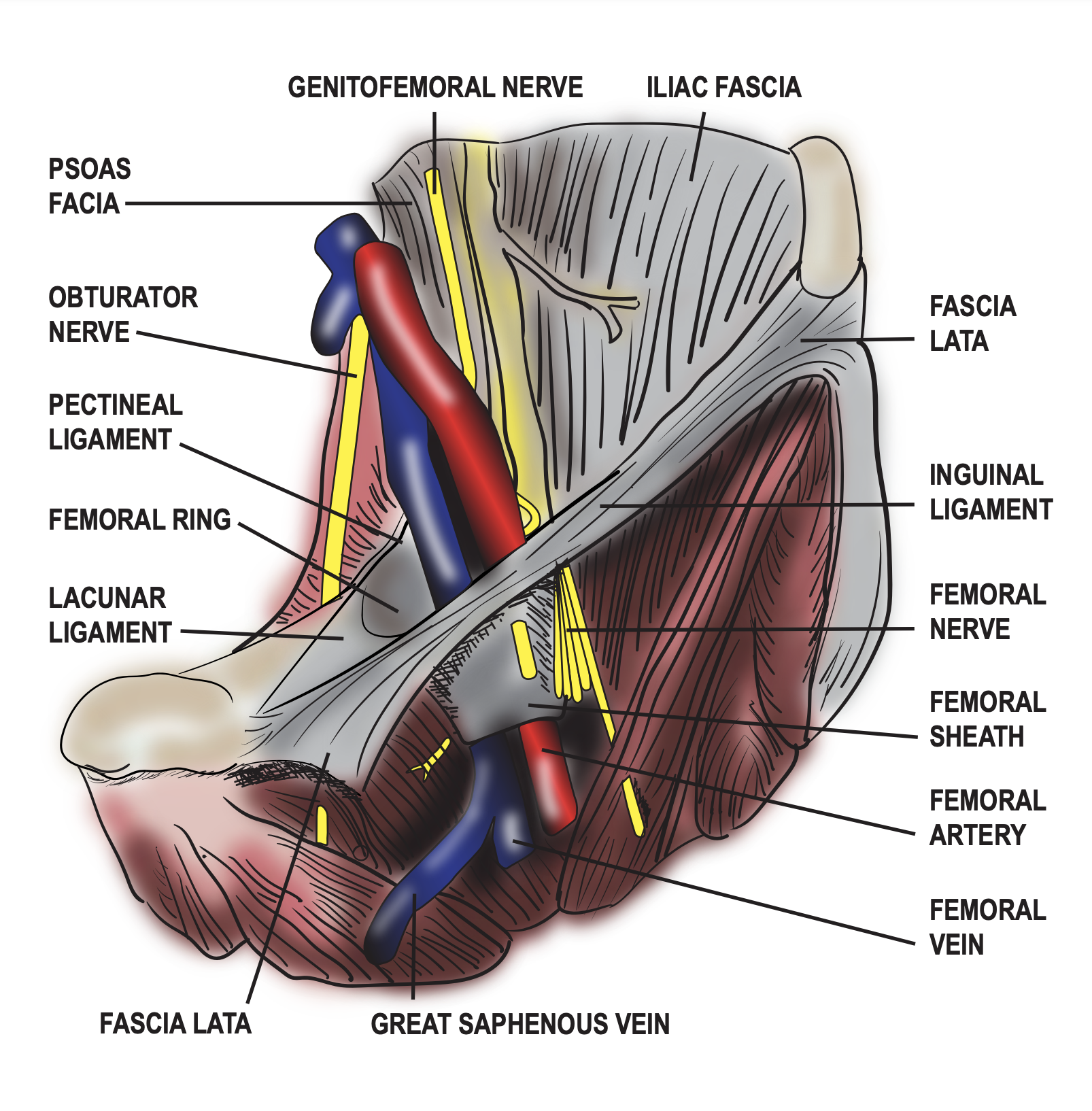
Diagram of the femoral sheath and its contents. Contributed by Penney Dellavalle.
References
HerniaSurge Group. International guidelines for groin hernia management. Hernia : the journal of hernias and abdominal wall surgery. 2018 Feb:22(1):1-165. doi: 10.1007/s10029-017-1668-x. Epub 2018 Jan 12 [PubMed PMID: 29330835]
Lytle WJ. Inguinal anatomy. Journal of anatomy. 1979 May:128(Pt 3):581-94 [PubMed PMID: 468709]
Yoshida S, Nakagomi K, Goto S. Abscess formation in the prevesical space and bilateral thigh muscles secondary to osteomyelitis of the pubis--basis of the anatomy between the prevesical space and femoral sheath. Scandinavian journal of urology and nephrology. 2004:38(5):440-1 [PubMed PMID: 15764260]
Level 3 (low-level) evidenceTotté E, Van Hee R, Kox G, Hendrickx L, van Zwieten KJ. Surgical anatomy of the inguinal region: implications during inguinal laparoscopic herniorrhaphy. European surgical research. Europaische chirurgische Forschung. Recherches chirurgicales europeennes. 2005 May-Jun:37(3):185-90 [PubMed PMID: 16088185]
Benjamin M. The fascia of the limbs and back--a review. Journal of anatomy. 2009 Jan:214(1):1-18. doi: 10.1111/j.1469-7580.2008.01011.x. Epub [PubMed PMID: 19166469]
Level 3 (low-level) evidenceGatton ML, Pearcy MJ, Pettet GJ, Evans JH. A three-dimensional mathematical model of the thoracolumbar fascia and an estimate of its biomechanical effect. Journal of biomechanics. 2010 Oct 19:43(14):2792-7. doi: 10.1016/j.jbiomech.2010.06.022. Epub 2010 Aug 14 [PubMed PMID: 20709320]
Vieira L, Embryology of the Fascial System. Cureus. 2020 Aug 30; [PubMed PMID: 33005546]
Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. The thoracolumbar fascia: anatomy, function and clinical considerations. Journal of anatomy. 2012 Dec:221(6):507-36. doi: 10.1111/j.1469-7580.2012.01511.x. Epub 2012 May 27 [PubMed PMID: 22630613]
Kaki A, Blank N, Alraies MC, Kajy M, Grines CL, Hasan R, Htun WW, Glazier J, Mohamad T, Elder M, Schreiber T. Access and closure management of large bore femoral arterial access. Journal of interventional cardiology. 2018 Dec:31(6):969-977. doi: 10.1111/joic.12571. Epub 2018 Nov 19 [PubMed PMID: 30456854]
Scaglioni MF, Suami H. Lymphatic anatomy of the inguinal region in aid of vascularized lymph node flap harvesting. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2015 Mar:68(3):419-27. doi: 10.1016/j.bjps.2014.10.047. Epub 2014 Nov 11 [PubMed PMID: 25465766]
Shen P, Conforti AM, Essner R, Cochran AJ, Turner RR, Morton DL. Is the node of Cloquet the sentinel node for the iliac/obturator node group? Cancer journal (Sudbury, Mass.). 2000 Mar-Apr:6(2):93-7 [PubMed PMID: 11069226]
Cesmebasi A, Yadav A, Gielecki J, Tubbs RS, Loukas M. Genitofemoral neuralgia: a review. Clinical anatomy (New York, N.Y.). 2015 Jan:28(1):128-35. doi: 10.1002/ca.22481. Epub 2014 Nov 5 [PubMed PMID: 25377757]
Iwanaga J, Simonds E, Schumacher M, Kikuta S, Watanabe K, Tubbs RS. Revisiting the genital and femoral branches of the genitofemoral nerve: Suggestion for a more accurate terminology. Clinical anatomy (New York, N.Y.). 2019 Apr:32(3):458-463. doi: 10.1002/ca.23327. Epub [PubMed PMID: 30592097]
Lonchena TK,McFadden K,Orebaugh SL, Correlation of ultrasound appearance, gross anatomy, and histology of the femoral nerve at the femoral triangle. Surgical and radiologic anatomy : SRA. 2016 Jan; [PubMed PMID: 25821034]
Rosenberg J, Bisgaard T, Kehlet H, Wara P, Asmussen T, Juul P, Strand L, Andersen FH, Bay-Nielsen M, Danish Hernia Database. Danish Hernia Database recommendations for the management of inguinal and femoral hernia in adults. Danish medical bulletin. 2011 Feb:58(2):C4243 [PubMed PMID: 21299930]
Clyde DR, de Beaux A, Tulloh B, O'Neill JR. Minimising recurrence after primary femoral hernia repair; is mesh mandatory? Hernia : the journal of hernias and abdominal wall surgery. 2020 Feb:24(1):137-142. doi: 10.1007/s10029-019-02007-6. Epub 2019 Aug 12 [PubMed PMID: 31407108]
Chen J, Lv Y, Shen Y, Liu S, Wang M. A prospective comparison of preperitoneal tension-free open herniorrhaphy with mesh plug herniorrhaphy for the treatment of femoral hernias. Surgery. 2010 Nov:148(5):976-81. doi: 10.1016/j.surg.2010.02.006. Epub 2010 Mar 31 [PubMed PMID: 20356615]
Level 1 (high-level) evidenceCeriani V, Faleschini E, Sarli D, Lodi T, Roncaglia O, Bignami P, Osio C, Somalvico F. Femoral hernia repair. Kugel retroparietal approach versus plug alloplasty: a prospective study. Hernia : the journal of hernias and abdominal wall surgery. 2006 Apr:10(2):169-74 [PubMed PMID: 16482402]
Kang JS, Qiao F, Nie L, Wang Y, He SW, Wu B. Preperitoneal femoral hernioplasty: an "umbrella" technique. Hernia : the journal of hernias and abdominal wall surgery. 2015 Oct:19(5):805-8. doi: 10.1007/s10029-014-1273-1. Epub 2014 Jun 14 [PubMed PMID: 24927966]
Level 2 (mid-level) evidenceChan G, Chan CK. Longterm results of a prospective study of 225 femoral hernia repairs: indications for tissue and mesh repair. Journal of the American College of Surgeons. 2008 Sep:207(3):360-7. doi: 10.1016/j.jamcollsurg.2008.04.018. Epub 2008 Jun 2 [PubMed PMID: 18722941]
Sorelli PG, El-Masry NS, Garrett WV. Open femoral hernia repair: one skin incision for all. World journal of emergency surgery : WJES. 2009 Nov 30:4():44. doi: 10.1186/1749-7922-4-44. Epub 2009 Nov 30 [PubMed PMID: 19948016]
Okazaki R, Poudel S, Hane Y, Saito T, Muto J, Syoji Y, Hase R, Senmaru N, Hirano S. Laparoscopic approach as a safe and effective option for incarcerated femoral hernias. Asian journal of endoscopic surgery. 2022 Apr:15(2):328-334. doi: 10.1111/ases.13010. Epub 2021 Nov 8 [PubMed PMID: 34749433]
Peitsch WK. A modified laparoscopic hernioplasty (TAPP) is the standard procedure for inguinal and femoral hernias: a retrospective 17-year analysis with 1,123 hernia repairs. Surgical endoscopy. 2014 Feb:28(2):671-82. doi: 10.1007/s00464-013-3208-9. Epub 2013 Sep 17 [PubMed PMID: 24043647]
Level 2 (mid-level) evidenceAiolfi A, Cavalli M, Ferraro SD, Manfredini L, Bonitta G, Bruni PG, Bona D, Campanelli G. Treatment of Inguinal Hernia: Systematic Review and Updated Network Meta-analysis of Randomized Controlled Trials. Annals of surgery. 2021 Dec 1:274(6):954-961. doi: 10.1097/SLA.0000000000004735. Epub [PubMed PMID: 33427757]
Level 1 (high-level) evidenceAiolfi A, Cavalli M, Del Ferraro S, Manfredini L, Lombardo F, Bonitta G, Bruni PG, Panizzo V, Campanelli G, Bona D. Total extraperitoneal (TEP) versus laparoscopic transabdominal preperitoneal (TAPP) hernioplasty: systematic review and trial sequential analysis of randomized controlled trials. Hernia : the journal of hernias and abdominal wall surgery. 2021 Oct:25(5):1147-1157. doi: 10.1007/s10029-021-02407-7. Epub 2021 Apr 13 [PubMed PMID: 33851270]
Level 1 (high-level) evidenceLockhart K, Dunn D, Teo S, Ng JY, Dhillon M, Teo E, van Driel ML. Mesh versus non-mesh for inguinal and femoral hernia repair. The Cochrane database of systematic reviews. 2018 Sep 13:9(9):CD011517. doi: 10.1002/14651858.CD011517.pub2. Epub 2018 Sep 13 [PubMed PMID: 30209805]
Level 1 (high-level) evidenceKunduz E, Sormaz İC, Yapalak Y, Bektasoglu HK, Gok AF. Comparison of surgical techniques and results for emergency or elective femoral hernia repair. Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES. 2019 Nov:25(6):611-615. doi: 10.14744/tjtes.2019.04524. Epub [PubMed PMID: 31701494]
Putnis S, Wong A, Berney C. Synchronous femoral hernias diagnosed during endoscopic inguinal hernia repair. Surgical endoscopy. 2011 Dec:25(12):3752-4. doi: 10.1007/s00464-011-1781-3. Epub 2011 Jun 3 [PubMed PMID: 21638171]
Level 2 (mid-level) evidenceAlhambra-Rodriguez de Guzmán C, Picazo-Yeste J, Tenías-Burillo JM, Moreno-Sanz C. Improved outcomes of incarcerated femoral hernia: a multivariate analysis of predictive factors of bowel ischemia and potential impact on postoperative complications. American journal of surgery. 2013 Feb:205(2):188-93. doi: 10.1016/j.amjsurg.2012.03.011. Epub 2012 Sep 26 [PubMed PMID: 23021195]
Level 2 (mid-level) evidenceHumes DJ, Radcliffe RS, Camm C, West J. Population-based study of presentation and adverse outcomes after femoral hernia surgery. The British journal of surgery. 2013 Dec:100(13):1827-32. doi: 10.1002/bjs.9336. Epub [PubMed PMID: 24227371]
Wiles BM, Child N, Roberts PR. How to achieve ultrasound-guided femoral venous access: the new standard of care in the electrophysiology laboratory. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2017 Jun:49(1):3-9. doi: 10.1007/s10840-017-0227-9. Epub 2017 Feb 7 [PubMed PMID: 28168447]
Powell JT, Mink JT, Nomura JT, Levine BJ, Jasani N, Nichols WL, Reed J, Sierzenski PR. Ultrasound-guidance can reduce adverse events during femoral central venous cannulation. The Journal of emergency medicine. 2014 Apr:46(4):519-24. doi: 10.1016/j.jemermed.2013.08.023. Epub 2014 Jan 22 [PubMed PMID: 24462032]
Level 2 (mid-level) evidenceKhan Z, Nattanamai P, Keerthivaas P, Newey CR. An Evaluation of Complications in Femoral Arterial Sheaths Maintained Post-Neuroangiographic Procedures. Cureus. 2018 Feb 26:10(2):e2230. doi: 10.7759/cureus.2230. Epub 2018 Feb 26 [PubMed PMID: 29713575]
Bhatia K, Guest W, Lee H, Klostranec J, Kortman H, Orru E, Qureshi A, Kostynskyy A, Agid R, Farb R, Radovanovic I, Nicholson P, Krings T, Pereira VM. Radial vs. Femoral Artery Access for Procedural Success in Diagnostic Cerebral Angiography : A Randomized Clinical Trial. Clinical neuroradiology. 2021 Dec:31(4):1083-1091. doi: 10.1007/s00062-020-00984-1. Epub 2020 Dec 29 [PubMed PMID: 33373017]
Level 1 (high-level) evidencePlata Bello A, Apatov SE, Benfante NE, Rivero Belenchón I, Picola Brau N, Mercader Barrull C, Jenjitranant P, Vickers AJ, Fine SW, Touijer KA. Prevalence of High-Risk Prostate Cancer Metastasis to Cloquet's Ilioinguinal Lymph Node. The Journal of urology. 2022 Jun:207(6):1222-1226. doi: 10.1097/JU.0000000000002439. Epub 2022 Jan 20 [PubMed PMID: 35050701]
Koh YX, Chok AY, Zheng H, Xu S, Teo MC. Cloquet's node trumps imaging modalities in the prediction of pelvic nodal involvement in patients with lower limb melanomas in Asian patients with palpable groin nodes. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2014 Oct:40(10):1263-70. doi: 10.1016/j.ejso.2014.05.008. Epub 2014 Jun 5 [PubMed PMID: 24947073]
Level 2 (mid-level) evidence