Introduction
The lingual artery, which supplies the tongue as well as the oral floor, is a major branch of the external carotid artery. It appears anteromedially from the external carotid artery, at the tip of the greater horn of the hyoid bone, between the superior thyroid artery and the facial artery.[1] The lingual artery moves medially to the hyoid bone while crossing the hypoglossal nerve (CN XII). It then courses deep to the stylohyoid and digastric muscles while subsequently passing between the middle constrictor and the hyoglossus muscles.[2] As the lingual artery progresses to the tip of the tongue, it branches to supply the adjacent tissues. The major branches of the lingual artery include the suprahyoid artery, the dorsal lingual artery, the sublingual artery, and the deep lingual artery, also known as the ranine artery.[3]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The lingual artery has multiple branches and subsequently supplies many structures in the lingual and sublingual regions. The first branch of the lingual artery is the suprahyoid artery, which courses along the hyoid bone, a sesamoid bone, while supplying the muscles attached to it. The next branch is the dorsal lingual artery, which supplies the posterior portion of the tongue, palatoglossal arch, lingual tonsil, soft palate, and epiglottis.[1] The sublingual artery is the third branch and supplies the sublingual gland, the genioglossus, the geniohyoid, the mylohyoid, the buccal and gingival mucosa, and the mandible.[1] The end branches of the right and left sublingual arteries anastomose in the lingual foramen on the posterior side of the mandible.[4]The deep lingual artery is the terminal branch of the lingual artery, and it supplies the body and tip of the tongue.
Of relevance, there is an anatomical triangular landmark where the lingual artery can be located with consistency. Lesser’s triangle, which is inside the submandibular triangle, contains the lingual artery as it courses toward the apex of the tongue from its origin of the external carotid artery. Lesser’s triangle is bound by the anterior belly of digastric muscle inferiorly, the posterior belly of the digastric muscle posteriorly, and the hypoglossal nerve superiorly.[5] The floor of Lesser’s triangle is the hyoglossus muscle, and the lingual artery is found deep to it.[6] The accessibility of the lingual artery in Lesser’s triangle makes it a perfect target for surgery.
The lingual artery has a diameter of about 2 to 5 mm, which increases as it approaches the external carotid artery.
Embryology
During the 4th and 5th weeks of embryological development, the aortic sac gives rise to the aortic arches. The external carotid artery develops from the 3rd aortic arch and gives rise to the lingual artery.[7]
The intra-embryonic vessels originate from blood islands in the splanchnic mesoderm in front of the protocordal disc, where a plexiform horseshoe-shaped network forms surrounding the cephalic portion of the embryo. At the same time, two groups of angioblastic cells, in a dorsal paramedian position, form two parallel vessels, the dorsal aorta, which connect cephalically connect to the plexiform network. The further development of the vascular system consists of the formation of larger caliber ducts with a primitive plexiform network. The most voluminous of these are the right and left primitive aortas, from which the fetal arterial tree originates and develops parallel to the heart tube and its subsequent evolution.The formation of an anastomosis between the intra- and extra-embryonic vessels completes the circulatory system.
Blood Supply and Lymphatics
The lingual artery is accompanied by the dorsal lingual vein, while the deep lingual vein lies near the mucous membrane of the inferior surface of the tongue.[2] The origin of the lingual artery is close to the deep cervical lymph nodes. The submandibular lymph nodes are located laterally to the lingual artery. Finally, the submental lymph nodes are inferolateral to the sublingual and deep lingual branches of the lingual artery.
Generally, the length of the lingual artery is 75% of the length of the tongue, from the dorsal portion up to the tip. The path of the artery has a lateral and inferior direction for about three-quarters of its length.
Nerves
The hypoglossal nerve (CN XII) is the last cranial nerve in the body, located on the posterior portion of the medulla oblongata. The hypoglossal nerve exits the skull in the posterior fossa via the hypoglossal canal. The hypoglossal nerve then descends deep to the sternocleidomastoid muscle and superficial to the external carotid artery. The hypoglossal nerve then makes a horizontal turn toward the greater horn of the hyoid bone and subsequently comes into proximity of the lingual artery.[8] The function of the hypoglossal nerve is to innervate the intrinsic and three extrinsic muscles of the tongue: the genioglossus, the styloglossus, and the hyoglossus.[9]
The hypoglossal-lingual neurovascular bundle (HLNVB) is located at the base of the tongue and is an important contributor to proper tongue structure and function.[10] Some several surgical implications and considerations require attention when dealing with the HLNVB. This article will discuss these later.
The chorda tympani is a branch of the facial nerve (CN VII) and provides taste sensation from the anterior two-thirds of the tongue. The lingual nerve provides general sensation from the anterior two-thirds of the tongue. The nerve fibers that make up the chorda tympani are special visceral afferents.[11] The chorda tympani appear traversing the middle ear in between the malleus and incus and eventually joining the lingual nerve.[11]
Muscles
The lingual artery branches off the external carotid artery in the neck-deep to the platysma muscle. The lingual artery moves medially to the greater hone of the hyoid bone and dives deep to the digastric and stylohyoid muscles. The lingual artery passes between the middle constrictor of the pharynx and the hyoglossus muscles.[2] At the anterior border of the hyoglossus muscle, the lingual artery ascends to the tip of the tongue.
Physiologic Variants
The lingual artery can have many anatomical variations. Of interest are trunks that form with other branches of the external carotid artery. The lingual artery can create a trunk with the facial artery called the linguofacial trunk, with the superior thyroid artery called the thyrolingual trunk, and with the superior thyroid and facial arteries called the thyrolinguofacial trunk.[3] Regarding the pathway that the lingual artery takes, variations are abundant. A classification system has been proposed to standardize and mitigate the seemingly endless lingual artery variants. This classification system pays close attention to the lingual artery’s relationship to the hyoglossus and mylohyoid muscles.[3]
Surgical Considerations
The lingual artery is an important component in various head and neck procedures. Otolaryngologists utilize the base of the tongue for treating sleep apnea, neoplasms, and dysphagia.[12] Resecting the tongue base needs to be done with care for the lingual artery due to the susceptibility of damage during surgery. Understanding the location of the lingual artery is imperative for decreasing intraoperative complications. Injury to the lingual artery during surgery can lead to life-threatening hemorrhage, and if both lingual arteries are damaged, necrosis of the tongue can result.[13]
There is both a transoral and transcervical approach to accessing the tongue in surgery. With the transoral approach, caution regarding the HLNVB to avoid functional deficits is necessary, while the transcervical approach allows for greater tongue-based resections with the preservation of both HLNVB.[10] The reason for the increased surgical flexibility at the base of the tongue has to do with the relationship of the HLNVB to the superior aspect of the hyoid bone.[10]
Clinical Significance
The lingual artery correlates with several clinical scenarios where adverse outcomes or complications arise. The surgery section of this review discussed how the lingual artery could become ligated, either intraoperatively or via trauma, and lead to necrosis. Recent research has demonstrated that bilateral lingual artery stenosis can also lead to necrosis. In a recent case report, a 61-year-old male underwent chemoradiotherapy for head and neck squamous cell carcinoma that leads to tongue necrosis via radiation-induced lingual artery stenosis.[14]
Pseudoaneurysms of the lingual artery can present with oral/nasal hemorrhage and may be mistaken for epistaxis.[15] A computer tomography angiography can be conducted on the lingual artery to show anatomical data in physiological settings, as in the pseudoaneurysm or stenosis.[16]
Giant cell arteritis (GCA), a medium and large vessel vasculitis, can cause lingual manifestations. Inflammation of the lingual artery in GCA can lead to edema, pallor, pain, and intermittent claudication with tongue necrosis being an exceedingly rare complication.[17]
Other Issues
A case report highlighted a trauma to the lingual artery due to traumatic intubation following cardiac surgery.[18]
The presence of a lingual carcinoma can cause a rupture of the lingual artery and cause severe hemorrhage.[19]
Facial trauma could cause dilation of the lingual artery (pseudoaneurysm), which could lead to hemorrhage.[20]
Media
(Click Image to Enlarge)

Arteries and Veins of the Tongue. Internal jugular vein, dorsalis linguae artery, lingual vein, veins of dorsum of tongue, and hypoglossal nerve.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)

The Mouth, Coronal section of tongue; showing intrinsic muscles, Insertion of Transversus, Styloglossus, Hyoglossus, Longitudinalis inferior, Lingual artery, Longitudinalis superior, Papillae of tongue, Septum, Vertical fibers of Genioglossus intersecting transversus
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
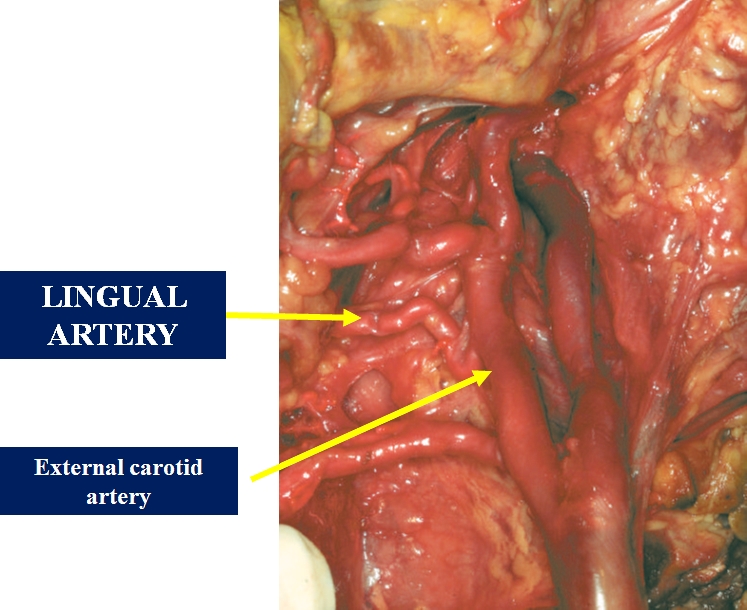
The figure shows the lingual artery from the external carotid artery. Contributed by Bruno Bordoni, PhD.
References
Buffoli B, Verzeletti V, Rezzani R, Rodella LF. Unusual branch of the lingual artery supplies the infrahyoid muscles. Anatomical science international. 2020 Jan:95(1):153-155. doi: 10.1007/s12565-019-00501-6. Epub 2019 Aug 23 [PubMed PMID: 31444702]
Sakamoto Y. Gross anatomical observations of attachments of the middle pharyngeal constrictor. Clinical anatomy (New York, N.Y.). 2014 May:27(4):603-9. doi: 10.1002/ca.22344. Epub 2013 Dec 17 [PubMed PMID: 24343865]
Seki S, Sumida K, Yamashita K, Baba O, Kitamura S. Gross anatomical classification of the courses of the human lingual artery. Surgical and radiologic anatomy : SRA. 2017 Feb:39(2):195-203. doi: 10.1007/s00276-016-1696-8. Epub 2016 May 17 [PubMed PMID: 27189234]
McDonnell D, Reza Nouri M, Todd ME. The mandibular lingual foramen: a consistent arterial foramen in the middle of the mandible. Journal of anatomy. 1994 Apr:184 ( Pt 2)(Pt 2):363-9 [PubMed PMID: 8014127]
Singh M, Vashistha A, Chaudhary M, Kaur G. Forgotten triangles of neck. Annals of maxillofacial surgery. 2016 Jan-Jun:6(1):91-3. doi: 10.4103/2231-0746.186149. Epub [PubMed PMID: 27563614]
Kikuta S, Iwanaga J, Kusukawa J, Tubbs RS. Triangles of the neck: a review with clinical/surgical applications. Anatomy & cell biology. 2019 Jun:52(2):120-127. doi: 10.5115/acb.2019.52.2.120. Epub 2019 Jun 30 [PubMed PMID: 31338227]
Meegalla N, Sood G, Nessel TA, Downs BW. Anatomy, Head and Neck: Facial Arteries. StatPearls. 2023 Jan:(): [PubMed PMID: 30725617]
Iaconetta G, Solari D, Villa A, Castaldo C, Gerardi RM, Califano G, Montagnani S, Cappabianca P. The Hypoglossal Nerve: Anatomical Study of Its Entire Course. World neurosurgery. 2018 Jan:109():e486-e492. doi: 10.1016/j.wneu.2017.10.006. Epub 2017 Oct 12 [PubMed PMID: 29032218]
Yu JL, Thaler ER. Hypoglossal Nerve (Cranial Nerve XII) Stimulation. Otolaryngologic clinics of North America. 2020 Feb:53(1):157-169. doi: 10.1016/j.otc.2019.09.010. Epub 2019 Nov 4 [PubMed PMID: 31699408]
Lauretano AM, Li KK, Caradonna DS, Khosta RK, Fried MP. Anatomic location of the tongue base neurovascular bundle. The Laryngoscope. 1997 Aug:107(8):1057-9 [PubMed PMID: 9261008]
Rao A, Tadi P. Anatomy, Head and Neck, Chorda Tympani. StatPearls. 2023 Jan:(): [PubMed PMID: 31536194]
Cohen DS, Low GM, Melkane AE, Mutchnick SA, Waxman JA, Patel S, Shkoukani MA, Lin HS. Establishing a danger zone: An anatomic study of the lingual artery in base of tongue surgery. The Laryngoscope. 2017 Jan:127(1):110-115. doi: 10.1002/lary.26048. Epub 2016 May 30 [PubMed PMID: 27238879]
Mun MJ, Lee CH, Lee BJ, Lee JC, Jang JY, Jung SH, Wang SG. Histopathologic Evaluations of the Lingual Artery in Healthy Tongue of Adult Cadaver. Clinical and experimental otorhinolaryngology. 2016 Sep:9(3):257-62. doi: 10.21053/ceo.2015.01137. Epub 2016 Jun 18 [PubMed PMID: 27334510]
Holtz F, Monnier Y, Borner U, Nisa L. Bilateral lingual artery stenosis: A rare, late complication of chemoradiotherapy. European annals of otorhinolaryngology, head and neck diseases. 2017 Sep:134(4):269-271. doi: 10.1016/j.anorl.2017.02.002. Epub 2017 Mar 11 [PubMed PMID: 28291634]
Sumita K, Karakama J, Makita I, Miki K, Yoshino Y, Yoshimura M, Maehara T, Nemoto S. [A Case of Pseudoaneurysm of the Lingual Artery that was Difficult to be Distinguished from Epistaxis]. No shinkei geka. Neurological surgery. 2018 Oct:46(10):911-916. doi: 10.11477/mf.1436203838. Epub [PubMed PMID: 30369494]
Level 3 (low-level) evidenceMei J, Liu Y, Zhao H, Liu B, Xu S, Wu JF. [The study of clinical anatomy of lingual artery in physiological condition]. Lin chuang er bi yan hou tou jing wai ke za zhi = Journal of clinical otorhinolaryngology, head, and neck surgery. 2007 May:21(9):396-9 [PubMed PMID: 17634021]
Sobrinho RABS, de Lima KCA, Moura HC, Araújo MM, de Assis CMRB, Gouveia PADC. Tongue Necrosis Secondary to Giant Cell Arteritis: A Case Report and Literature Review. Case reports in medicine. 2017:2017():6327437. doi: 10.1155/2017/6327437. Epub 2017 Mar 23 [PubMed PMID: 28424735]
Level 3 (low-level) evidenceVanDeCappelle C, Wong J, Buchanan IM, Korman B, Ricci C. Life-threatening lingual artery hemorrhage after cardiac surgery. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2017 Mar:64(3):333-334. doi: 10.1007/s12630-016-0770-3. Epub 2016 Nov 2 [PubMed PMID: 27807705]
Li ZP, Meng J, Wu HJ, Zhang J, Gu QP. [Application of superselective lingual artery embolization in treatment of severe hemorrhange in patients with carcinoma of tongue]. Zhonghua kou qiang yi xue za zhi = Zhonghua kouqiang yixue zazhi = Chinese journal of stomatology. 2018 Jun 9:53(6):425-427. doi: 10.3760/cma.j.issn.1002-0098.2018.06.012. Epub [PubMed PMID: 29886639]
Level 2 (mid-level) evidenceMargallo L, Zárate EO, Franco M, Garcia-Iruretagoyena M, Cherro R, Barbier L, Mendiola J, Constantinescu T. Lingual Artery Pseudoaneurysm after Severe Facial Trauma. Craniomaxillofacial trauma & reconstruction. 2018 Sep:11(3):219-223. doi: 10.1055/s-0037-1603454. Epub 2017 May 18 [PubMed PMID: 30087752]