 Anatomy, Shoulder and Upper Limb, Hand Cutaneous Innervation
Anatomy, Shoulder and Upper Limb, Hand Cutaneous Innervation
Introduction
Three independent nerves supply the cutaneous innervation of the hand (see Image. Hand Cutaneous Innervation). From lateral to medial, these nerves include the superficial branch of the radial, median, and ulnar nerve. These peripheral nerves originate from the C5 to T1 levels of the spinal column. The sensory distribution discussed here includes both the ventral and dorsal aspects of the hand, ending proximally at the level of the wrist. Also briefly discussed here are a set of muscles innervated by these nerves as they supply the cutaneous innervation of the hand.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Structure
The cutaneous innervation of the hand is formed primarily by the terminal branches of 3 nerves: the median, radial, and ulnar. The brachial plexus forms These nerves proximally, which arise from the cervical root levels C5 to T1. These nerves course through the axilla and various compartments of the arm and forearm until reaching the wrist, where each nerve's sensory and motor branches are distributed throughout the hand. The radial and median nerves receive and send input via each brachial plexus level C5 to T1, while the ulnar nerve receives and sends inputs via just the C8 and T1 spinal levels. The anatomic course of these nerves is discussed in greater detail below. These sensory branches include the superficial radial nerve, superficial and dorsal ulnar nerve, and the palmar branch of the median nerve. These nerves then give off digital nerve branches that feed into the individual digits, providing cutaneous sensory information to the brain.[2][3]
Function
The function of these nerves summates the cutaneous innervation of the hand and the muscular innervation of a few muscles, which are discussed in the muscles portion of this document. They provide the brain with touch, pressure, pain, and temperature sensations. These nerves contain sympathetic and autonomic afferent fibers and sympathetic efferent fibers providing innervation to the cutaneous blood vessels, sweat glands, and arrector pili muscles of hair follicles. These autonomic afferent fibers primarily supply the cutaneous innervation.[4]
Embryology
As with all peripheral nerves, the cutaneous innervation of the hand arises from neural crest cells, which derive from the embryonic ectoderm. These cells take the form of bilateral strips at the junction of the ectoderm and neural plate, which detach and migrate with the merging of the 2 ectodermal regions during embryogenesis. These neural crest cells migrate in a rostral to caudal distribution, ending in the formation of the peripheral nervous system, which includes the cutaneous innervation of the hand.[5]
Blood Supply and Lymphatics
The blood supply of the hand takes the form of the superficial and deep palmar arches, an anastomotic landmark formed from the ulnar and radial artery rami at the level of the wrist. These arches give off palmar digital arteries that feed the hand's digits, nerves, and muscles. The ulnar aspect of the arch follows with the course of the superficial ulnar nerve, discussed below, separate from it at the level of the bifurcation of this nerve. Branches of the median nerve follow the path of their respective palmar arteries.[6][7]
Nerves
Radial Nerve: Superficial Branch
This nerve yields sensory cutaneous innervation to a significant portion of the hand's dorsolateral aspect. The anatomic course of this nerve follows the course of the radial nerve. It lies slightly lateral to the radial artery and runs hidden beneath the brachioradialis muscle. It continues this path until approximately 7 cm above the wrist, piercing the deep fascia and dividing into 2 branches: lateral and medial.
- Lateral branch: Yields cutaneous innervation to the thumb's radial dorsal aspect, then joins the lateral antebrachial cutaneous nerve's dorsal terminal branch
- Median branch: Communicates first with the lateral antebrachial cutaneous, just proximal to the level of the wrist, then communicates with the dorsal branch of the ulnar nerve on the dorsal aspect of the hand distal to the wrist
Along this course, distal to the wrist, the superficial radial nerve gives off fibers innervating the dorsum of the hand. Around the anatomical level just described, it branches into terminal digital nerves, with each innervating specific portions of the hand as follows:
- First branch: Innervates the ulnar dorsal aspect of the thumb
- Second branch: Innervates the radial dorsal aspect of the index finger
- Third branch: Innervates the dorsal aspect of the joining sides of the index and middle finger
- Fourth branch: Communicates with a filament of the dorsal ulnar nerve, giving innervation to the dorsal aspect of the joining sides of the middle and ring fingers.
Aside from the thumb, the dorsal terminal aspect of the fingers discussed here can be innervated by terminal branches of the median nerve, as discussed below.[8][9]
Median Nerve
The first branch supplying cutaneous innervation is the palmar cutaneous branch of the median nerve. This branch begins proximal to the wrist and travels superficially to the flexor retinaculum, then gives off terminal fibers that supply cutaneous innervation to much of the lateral palm. After the median nerve passes through the carpal tunnel, it commonly divides into a smaller lateral branch and a thicker medial branch.
- Medial branch: Divides into the 2 common palmar digital nerves
- Lateral branch: Divides into the recurrent median nerve and 3 proper digital nerves.
The recurrent median nerve supplies motor innervation to the thenar muscle group, which includes opponens pollicis, abductor pollicis brevis, and the flexor pollicis brevis; it does not supply any of the cutaneous innervations of the hand. Starting with the 3 proper digital nerves off the lateral branch, 2 supply the cutaneous sensory innervation for both ventral lateral aspects of the thumb, while the remaining one supplies sensory innervation for the radial ventral aspect of the index finger. Next, the 2 common palmar digital nerves arising from the medial division of the median nerve yield their proper digital nerves. These proper digital nerves innervate the radial ventral aspect of the index finger, the middle finger's ventral aspects, and the ring finger's radial ventral aspect. These terminal branches may also innervate the terminal dorsal end of the digits just discussed.[10][11]
Ulnar Nerve
This nerve yields sensory cutaneous innervation to the dorsomedial and ventromedial aspect of the hand as well as motor innervation to the palmar brevis muscle; this is accomplished via 2 nerves: the dorsal cutaneous branch of the ulnar nerve and the palmar cutaneous branch of the ulnar nerve.
- Dorsal cutaneous ulnar branch: Originates, on average, 5 cm proximal to the ulnar styloid process, which then travels superficially to the dorsum of the hand. Here, it branches into common and proper digital nerves. The common digital nerve innervates the dorsum of the hand before splitting into more proper digital nerves. The summation of these proper digital nerves innervates the dorsum of the fifth and, most commonly, the ulnar dorsal aspect half of the fourth digit. The ulnar nerve bifurcates into the superficial and deep branches within the Guyon canal.
- Palmar cutaneous branch of the ulnar nerve: The superficial branch becomes the palmar cutaneous branch of the ulnar nerve within the palm. Here, it gives off fibers that innervate the ulnar aspect of the palm. The nerve then branches into proper and common digital nerves that supply the cutaneous innervation to the ventral aspect of the fifth digit and, most commonly, to the ulnar ventral aspect of the fourth digit.[12][13][14][15]
Muscles
The relevant muscles and their most commonly associated innervations are as follows (except the recurrent median nerve discussed previously):
- Palmaris brevis muscle: The superficial branch of the ulnar nerve
- First and second lumbrical: Median nerve
- Opponens pollicis: The recurrent branch of the median nerve
- Abductor pollicis brevis: The recurrent branch of the median nerve
- Flexor pollicis brevis: A recurrent branch of the median nerve
- Lumbricals:
Physiologic Variants
Anatomical variations primarily involve discrepancies between the anastomotic connections between the branches of the nerves discussed and variations in the origin of the common and proper digital nerves. Other variations usually involve the course or origin of the nerves as they enter the hand. Some of these variations are outlined here below.
Median Nerve
The anastomotic connection between the proper digital nerves of the median nerve and the superficial branch of the ulnar nerve sometimes originates from the median nerve instead of the ulnar nerve. The clinical consequence is that the median nerve may innervate the entire ring finger instead of only the radial half.[19][20][21] The median nerve has numerous branching pattern variations, including proximal, distal, and inside the carpal tunnel.[10]
Radial Nerve
A variation involving the superficial branch of the radial nerve as it courses through the forearm, where it maintains superficial to the brachioradialis until the level of the wrist. In this position, the nerve may be confused with either the medial or lateral antebrachial cutaneous nerves and thus should always be a consideration during surgery of this region.[22]
Ulnar Nerve
Occurring at the level of the hook of hamate, 5 types of bifurcations are described[10]:
- Type 1: Birfucates into a superficial sensory branch of the ulnar nerve (SSBUN) and a dorsal branch of the ulnar nerve (DBUN)
- Type 2: Trifurcates into a DBUN, third-digit common digital nerve, and a fifth-digit proper digital nerve
- Type 3: Similar to type 1, but the fifth-digit proper digital nerve originates off the DBUN
- Type 4: Trifurcates like type 2 but has an additional anastomotic superficial branch
- Type 5: Trifurcates like type 2 but has an additional distal DBUN off the fifth-digit proper digital nerve
Surgical Considerations
Any surgery near the entire course of the radial, ulnar, or median nerve could have downstream cutaneous sensory deficits of the hand if trauma occurs. Also, any surgery involving the brachial plexus or the spinal cord levels C5 to T1 could present with similar or identical deficits distally. Notably, carpal tunnel release holds the risk for median nerve damage as it enters the hand through the wrist. Also, anatomic variations such as those discussed prior should always be considered when working within the space of the forearm, wrist, or hand.[23][24][25][26]
Clinical Significance
Significant clinical sequelae involve the median, ulnar, and radial nerves. Some discussion follows, but it is important to note that there are relevant clinical consequences from almost every aspect of medicine.
General
Brachial plexopathy
The brachial plexus is a major anatomical landmark residing just lateral to the caudal cervical vertebrae. Originating from the spinal levels C5 to T1, it supplies the nerve fibers of the cutaneous innervation of the hand. Any damage to the brachial plexus causes downstream motor and sensory impairment. These injuries usually present with numbness, tingling, or pain in the digits and muscle weakness of the regions corresponding to their cervical spinal origin. Damage to the brachial plexus can come from any source, including trauma, iatrogenic, malignancy, compression, and ischemia.[27]
Cervical stenosis
In this clinical correlation, the transverse foramina of the cervical spine vertebrae becomes narrowed from osteoblastic changes. This narrowing can result in compression of the cervical spinal roots as they exit and, in severe cases, ischemia of these roots. Alteration to the conduction of these nerve roots via compression or ischemia leads to impaired sensory and strength of the corresponding upper extremity. Other presenting symptoms include neck pain, clumsiness of the ipsilateral upper extremity, burning, tingling, or numbness of the extremity.[28]
Wrist fractures
Any trauma to the wrist involving the displacement of the distal ulna or radius can lead to compression, trauma, or ischemia of their corresponding nerves. In this clinical correlation, the sensory and motor deficits are most often limited to the trauma's location and the distal aspects from there. This clinical picture, combined with a good history, should increase clinical suspicion of secondary neurovascular damage.[29]
Median
Carpal tunnel syndrome
This syndrome occurs when compression of the median nerve occurs while it traverses the narrow corridor of the carpal tunnel. This compression can occur secondary to swelling, trauma, and synovial thickening. Symptoms include numbness, tingling, burning, or pain, primarily localizing to the thumb, index, middle, and ring fingers. Weakness and fine motor control deficits may be present, as well. Risk factors include a hereditary component, repetitive hand use, improper hand or wrist positioning, pregnancy, and various health conditions such as diabetes, rheumatoid arthritis, and non-euthyroid states. Mild carpal tunnel syndrome is treatable with splinting, rest, and exercises, while more severe forms require surgery.[30]
Radial
Wartenberg syndrome
This is an entrapment syndrome involving the superficial branch of the radial nerve, also called cheiralgia paresthetica. Compression is thought to primarily occur at the posterior border of the brachioradialis, where the superficial radial nerves transition from superficial to deep, and compression is at greatest risk from repeated muscle use. Other etiologies include trauma, clothing that is too tight, and nerve stretch injuries. Presentation primarily consists of sensory deficits of the dorsal aspect of the thumb and dorsal first webspace. Other symptoms include burning, tingling, and clumsiness in this region.[31]
Ulnar
Cubital Tunnel Syndrome
This is the entrapment of the ulnar nerve as it passes through the cubital tunnel at the medial aspect of the elbow. This condition commonly occurs due to maintaining a flexed elbow for prolonged periods where the nerve is stretched and inflamed. Also, if the ulnar nerve slides in and out of the tunnel during flexion, this repetitive motion can be a source of inflammation and compression. Other causes of note are anything that leads to fluid buildup within the elbow, from a traumatic secondary source to another underlying illness. The presentation usually involves an early sensation of pain at the elbow level, but often, the syndrome does not present until it affects the hand. In this case, it is common to find burning, tingling, clumsiness, or numbness of the pinky and ring fingers.[32]
Media
(Click Image to Enlarge)
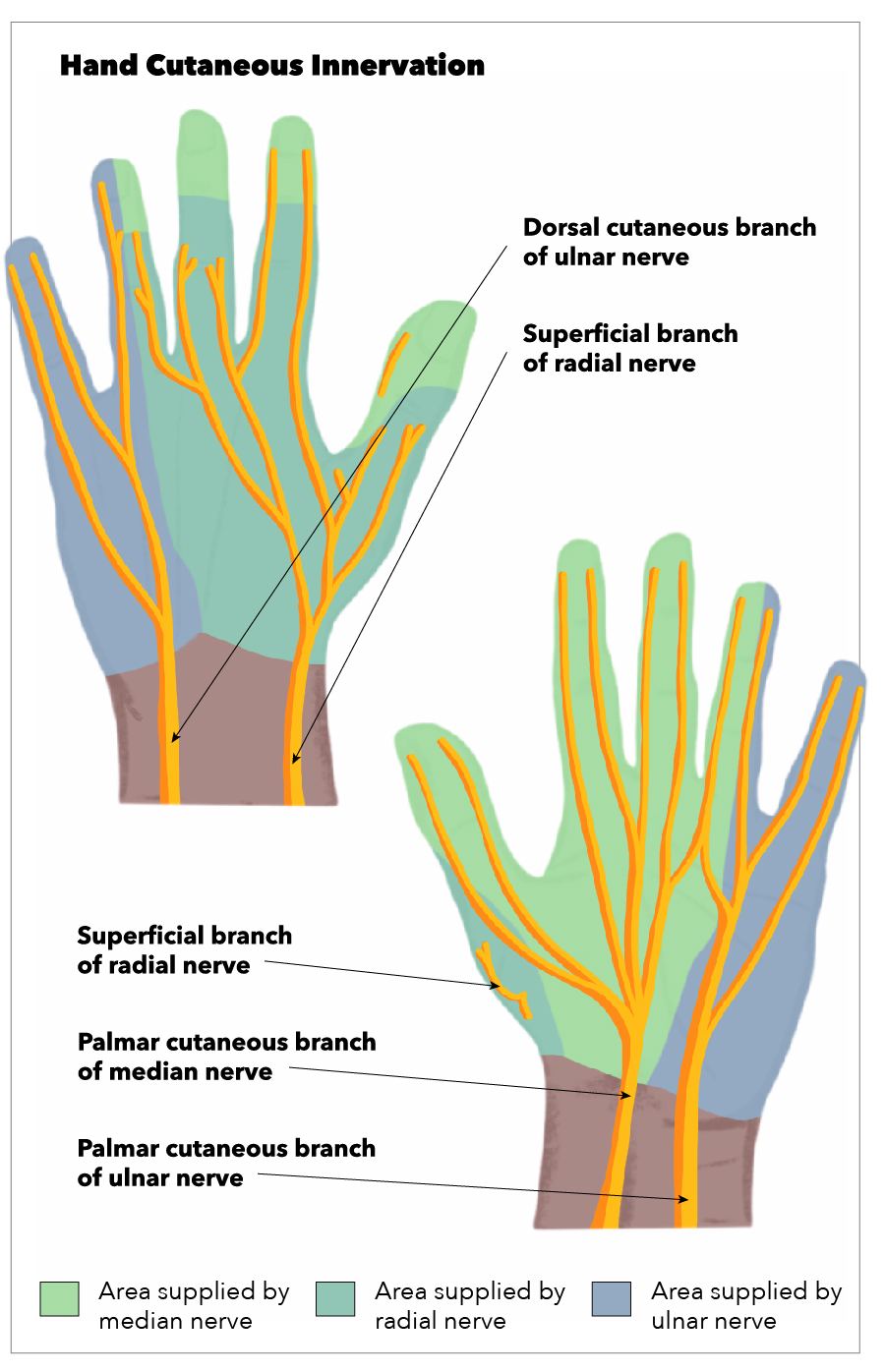
Hand Cutaneous Innervation. The superficial branch of the radial nerve, the palmar cutaneous branch of the median nerve, the palmar cutaneous branch of the ulnar nerve, the superficial branch of the radial nerve, and the dorsal cutaneous branch of the ulnar nerve.
Illustration by E Gregory
References
Nowakowski P, Bieryło A. Ultrasound guided axillary brachial plexus plexus block. Part 1--basic sonoanatomy. Anaesthesiology intensive therapy. 2015:47(4):409-16. doi: 10.5603/AIT.2015.0052. Epub [PubMed PMID: 26401746]
Chang KV, Mezian K, Naňka O, Wu WT, Lou YM, Wang JC, Martinoli C, Özçakar L. Ultrasound Imaging for the Cutaneous Nerves of the Extremities and Relevant Entrapment Syndromes: From Anatomy to Clinical Implications. Journal of clinical medicine. 2018 Nov 21:7(11):. doi: 10.3390/jcm7110457. Epub 2018 Nov 21 [PubMed PMID: 30469370]
Lleva JMC, Munakomi S, Chang KV. Ulnar Neuropathy. StatPearls. 2024 Jan:(): [PubMed PMID: 30480959]
Oaklander AL,Siegel SM, Cutaneous innervation: form and function. Journal of the American Academy of Dermatology. 2005 Dec; [PubMed PMID: 16310064]
Kaplan S, Odaci E, Unal B, Sahin B, Fornaro M. Chapter 2: Development of the peripheral nerve. International review of neurobiology. 2009:87():9-26. doi: 10.1016/S0074-7742(09)87002-5. Epub [PubMed PMID: 19682631]
Level 3 (low-level) evidenceZarzecki MP, Popieluszko P, Zayachkowski A, Pękala PA, Henry BM, Tomaszewski KA. The surgical anatomy of the superficial and deep palmar arches: A Meta-analysis. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2018 Nov:71(11):1577-1592. doi: 10.1016/j.bjps.2018.08.014. Epub 2018 Aug 24 [PubMed PMID: 30245020]
Level 1 (high-level) evidenceElsner T, Schramm U, Schrader M. Analysis of the vascular anatomy of the palm and its clinical relevance in Morbus Dupuytren. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2001 Jul:183(4):379-82 [PubMed PMID: 11508365]
Abrams RA, Brown RA, Botte MJ. The superficial branch of the radial nerve: an anatomic study with surgical implications. The Journal of hand surgery. 1992 Nov:17(6):1037-41 [PubMed PMID: 1430933]
Folberg CR, Ulson H Jr, Scheidt RB. THE SUPERFICIAL BRANCH OF THE RADIAL NERVE: A MORPHOLOGIC STUDY. Revista brasileira de ortopedia. 2009 Jan:44(1):69-74. doi: 10.1016/S2255-4971(15)30052-5. Epub 2015 Dec 6 [PubMed PMID: 26998456]
Wynter S, Dissabandara L. A comprehensive review of motor innervation of the hand: variations and clinical significance. Surgical and radiologic anatomy : SRA. 2018 Mar:40(3):259-269. doi: 10.1007/s00276-017-1898-8. Epub 2017 Jul 19 [PubMed PMID: 28725918]
DaSilva MF, Moore DC, Weiss AP, Akelman E, Sikirica M. Anatomy of the palmar cutaneous branch of the median nerve: clinical significance. The Journal of hand surgery. 1996 Jul:21(4):639-43 [PubMed PMID: 8842958]
Sulaiman S, Soames R, Lamb C. Ulnar nerve cutaneous distribution in the palm: Application to surgery of the hand. Clinical anatomy (New York, N.Y.). 2015 Nov:28(8):1022-8. doi: 10.1002/ca.22626. Epub 2015 Oct 5 [PubMed PMID: 26378873]
Depukat P, Mizia E, Zwinczewska H, Bonczar T, Mazur M, Dzikowska M, Pelka P, Matuszyk A. Topography of ulnar nerve and its variations with special respect to carpal region. Folia medica Cracoviensia. 2014:54(4):45-58 [PubMed PMID: 25891242]
Puna R, Poon P. The anatomy of the dorsal cutaneous branch of the ulnar nerve. The Journal of hand surgery, European volume. 2010 Sep:35(7):583-5. doi: 10.1177/1753193410373186. Epub 2010 May 24 [PubMed PMID: 20498153]
Tubbs RS, Rogers JM, Loukas M, Cömert A, Shoja MM, Cohen-Gadol AA. Anatomy of the palmar branch of the ulnar nerve: application to ulnar and median nerve decompressive surgery. Journal of neurosurgery. 2011 Jan:114(1):263-7. doi: 10.3171/2010.3.JNS091249. Epub 2010 Apr 2 [PubMed PMID: 20367079]
Dawson-Amoah K, Varacallo M. Anatomy, Shoulder and Upper Limb, Hand Intrinsic Muscles. StatPearls. 2024 Jan:(): [PubMed PMID: 30969632]
Okwumabua E, Sinkler MA, Bordoni B. Anatomy, Shoulder and Upper Limb, Hand Muscles. StatPearls. 2024 Jan:(): [PubMed PMID: 30725914]
Homma T, Sakai T. [Anatomy of intrinsic hand muscles]. Kaibogaku zasshi. Journal of anatomy. 1994 Apr:69(2):123-42 [PubMed PMID: 8023676]
Ferrari GP, Gilbert A. The superficial anastomosis on the palm of the hand between the ulnar and median nerves. Journal of hand surgery (Edinburgh, Scotland). 1991 Dec:16(5):511-4 [PubMed PMID: 1791361]
Biafora SJ, Gonzalez MH. Sensory communication of the median and ulnar nerves in the palm. Journal of surgical orthopaedic advances. 2007 Winter:16(4):192-5 [PubMed PMID: 18053401]
Level 3 (low-level) evidencePardal-Fernández JM, Guerrero-Solano JL, Godes-Medrano B, Sánchez-Honrubia RM. [Multiple abnormal innervation of the hand in one patient. Electrophysiological diagnosis]. Revista de neurologia. 2012 Mar 16:54(6):343-8 [PubMed PMID: 22403147]
Level 3 (low-level) evidenceHaugen TW, Cannady SB, Chalian AA, Shanti RM. Anatomical Variations of the Superficial Radial Nerve Encountered during Radial Forearm Free Flap Elevation. ORL; journal for oto-rhino-laryngology and its related specialties. 2019:81(2-3):155-158. doi: 10.1159/000496226. Epub 2019 Apr 29 [PubMed PMID: 31035280]
Webber CM, Shin AY, Kaufman KR. Upper extremity function in the free living environment of adults with traumatic brachial plexus injuries. Journal of electromyography and kinesiology : official journal of the International Society of Electrophysiological Kinesiology. 2022 Feb:62():102312. doi: 10.1016/j.jelekin.2019.05.013. Epub 2019 May 23 [PubMed PMID: 31151783]
Dekimpe C, Andreani O, Camuzard O, Raffaelli C, Petrover D, Foti P, Amoretti N. Ultrasound-guided percutaneous release of the carpal tunnel: comparison of the learning curves of a senior versus a junior operator. A cadaveric study. Skeletal radiology. 2019 Nov:48(11):1803-1809. doi: 10.1007/s00256-019-03207-y. Epub 2019 May 22 [PubMed PMID: 31114970]
Van Demark RE Jr, Anderson MC, List JT, Hayes M, Hayes M, Woodard D. Discovering an Anatomic Variant of the Palmaris Profundus during Open Carpal Tunnel Release. Plastic and reconstructive surgery. Global open. 2018 Aug:6(8):e1867. doi: 10.1097/GOX.0000000000001867. Epub 2018 Aug 3 [PubMed PMID: 30324055]
Verdecchia N, Johnson J, Baratz M, Orebaugh S. Neurologic complications in common wrist and hand surgical procedures. Orthopedic reviews. 2018 Mar 29:10(1):7355. doi: 10.4081/or.2018.7355. Epub 2018 Mar 29 [PubMed PMID: 29770175]
Khadilkar SV, Khade SS. Brachial plexopathy. Annals of Indian Academy of Neurology. 2013 Jan:16(1):12-8. doi: 10.4103/0972-2327.107675. Epub [PubMed PMID: 23661957]
Caridi JM, Pumberger M, Hughes AP. Cervical radiculopathy: a review. HSS journal : the musculoskeletal journal of Hospital for Special Surgery. 2011 Oct:7(3):265-72 [PubMed PMID: 23024624]
Cho CH, Kang CH, Jung JH. Ulnar nerve palsy following closed fracture of the distal radius: a report of 2 cases. Clinics in orthopedic surgery. 2010 Mar:2(1):55-8. doi: 10.4055/cios.2010.2.1.55. Epub 2010 Feb 4 [PubMed PMID: 20191002]
Level 3 (low-level) evidenceWipperman J, Goerl K. Carpal Tunnel Syndrome: Diagnosis and Management. American family physician. 2016 Dec 15:94(12):993-999 [PubMed PMID: 28075090]
Tosun N, Tuncay I, Akpinar F. Entrapment of the sensory branch of the radial nerve (Wartenberg's syndrome): an unusual cause. The Tohoku journal of experimental medicine. 2001 Mar:193(3):251-4 [PubMed PMID: 11315773]
Level 3 (low-level) evidenceCutts S. Cubital tunnel syndrome. Postgraduate medical journal. 2007 Jan:83(975):28-31 [PubMed PMID: 17267675]