Introduction
The scalene muscles are deep and positioned laterally in the neck (see Image. Neck Muscles). Innervation involves both the brachial plexus and the cervical plexus, contributing to a complex functional role. These multiarticular muscles facilitate accessory breathing and contribute to neck and head movement, as well as postural stability between the neck and head. Dysfunction can lead to pathological conditions such as thoracic outlet syndrome (TOS), reduced ventilatory capacity, and cervical pain. Medical interventions often aim to decrease excessive muscle tone, while rehabilitation focuses on restoring physiological length or enhancing contractile strength.
These muscles likewise have significant surgical importance. The anterior scalene serves as a key landmark for identifying the subclavian artery, the brachial plexus, and the phrenic nerve, which courses along its anterior surface. Partial or complete anterior scalene resection may be performed to relieve neurovascular compression during TOS decompression surgery. Additionally, the scalene muscles are relevant in central venous catheterization via the subclavian approach, as their proximity to major vessels increases the risk of vascular or nerve injury. Understanding the anatomy, function, and clinical significance of the scalene muscles helps clinicians manage various conditions in the cervicothoracic area.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The scalene muscles elevate the 1st and 2nd ribs during forced inspiration, functioning as secondary respiratory muscles.[1] Electrical activity persists even during nonforced breathing. When not engaged in respiration, these muscles remain active in the supine position and with the arm raised. Additionally, they contribute to cervical posture and play a role in neck movements, including lateral inclination and the initial degrees of head rotation. Bilateral contraction facilitates neck flexion.
Intercostal muscle afferents, particularly between the 8th and 10th ribs anteriorly, are closely linked to the scalene muscles, which respond bilaterally to unilateral stimulation. The exact mechanism remains unclear, but inspiration involving the lower ribs likely recruits the scalene muscles to support breathing.
The scalene muscles lie deep to the sternocleidomastoid muscle and lateral to the cervical spine, extending from the vertebrae to the 1st and 2nd ribs. These muscles are enclosed by the deep fascia, also known as the prevertebral fascia.
The anterior scalene originates from the anterior tubercles of the transverse processes of the 3rd to 6th cervical vertebrae and inserts on the scalene tubercle of the superior surface of the 1st rib (see Image. Anterior Muscles of the Neck). Some fibers may contact the pleural dome. The omohyoid muscle crosses over both the anterior and middle scalene muscles. The anterior scalene is thickest at the level of the cricoid cartilage and thinner at its origin and insertion. The phrenic nerve runs along its surface, sharing the muscle's fascia from the lateral to the medial border, passing behind the subclavian vein. The anterior and middle scalene muscles define the posterior interscalene gap (fissura scalenorum), through which the brachial plexus passes.[2]
The middle scalene originates from the transverse processes of the last 6 cervical vertebrae, between the anterior and posterior tubercles, and inserts on the superior surface of the 1st rib, posterior to the subclavian artery sulcus. The upper portion of the long thoracic nerve may pass between the middle and posterior scalene, through the middle scalene, or above it.[3] The posterior scalene originates from the posterior tubercles of the transverse processes of the last 3 or 4 cervical vertebrae and inserts on the anterior surface of the 2nd rib.
A 4th scalene muscle, the scalenus minimus, is present in approximately 30% to 71% of individuals.[4] This muscle arises from the anterior tubercle of the transverse process of the 7th cervical vertebra and inserts on the 1st rib and the Sibson fascia posteriorly, which covers the pleural dome. The scalenus minimus can be mistaken for the transverse pleural ligament.
Embryology
The scalene muscles develop from myoblasts originating in the hypaxial portion of the cervical myotomes, along with the prevertebral and geniohyoid muscles, during the 7th week of embryonic development.[5] The formation of these muscles is regulated by the surrounding connective tissue, which guides myoblast migration. The cervical connective tissue differs from the somitic mesoderm.
Blood Supply and Lymphatics
The scalene muscles receive blood supply from the 1st portion of the subclavian artery, referred to as the "prescalene area." The thyrocervical trunk passes medial to the anterior scalene and ascends before dividing into 2 terminal branches.[6] The inferior thyroid artery, the 1st branch, supplies the anterior scalene muscle. The ascending or superficial cervical artery, the 2nd branch, supplies the middle and posterior scalene muscles.[7][8][9][8] Venous drainage from the scalene muscles is directed into the brachiocephalic venous trunk.
The cervical region contains approximately 300 lymph nodes. Those draining the scalene muscles are consistently located within the posterior triangle of the neck. The drained lymph flows into the right and left jugular lymphatic trunks. Lymph from the right side enters the right lymphatic duct, while lymph from the left side drains into the thoracic duct.[10]
Nerves
The scalene muscles receive innervation from the anterior branches of the cervical spinal nerves spanning C3 to C8. Both the cervical and brachial plexuses contribute to this innervation, and their interaction is essential for the diverse functions of these muscles. Neuroanatomical variations in this region exist but are rare.[11]
Physiologic Variants
The scalene muscles, like any other anatomical region, exhibit various anatomical variations. The anterior scalene muscle may originate from C2 or exclude C6. This muscle's insertion may extend beyond the 1st rib to the 2nd or 3rd thoracic rib.[12] The muscle may also pass behind the subclavian artery, either unilaterally or bilaterally, and, in some cases, lie posterior to the 1st thoracic nerve. Literature reports rare instances of complete absence of the anterior scalene muscle, either unilaterally or bilaterally.[13] The middle scalene muscle may insert into the transverse processes of the atlas and extend toward the 2nd thoracic rib. Some reports describe an accessory middle scalene muscle forming a bridge with the anterior scalene, a variation potentially linked to symptoms resembling TOS.
The posterior scalene muscle may originate from C3 to C7, with some fibers merging with the middle scalene or the 1st intercostal muscle. The insertion of this muscle may extend to the 3rd thoracic rib, and in some individuals, the muscle may be absent. The middle scalene may be perforated by brachial plexus branches, such as C7 and C8, which terminate at the posterior scalene. Some studies describe a double-layered posterior scalene with distinct ventral and dorsal portions. The scalenus minimus may present as a flattened structure occupying a broad region of the thoracic outlet. The origin of this muscle may involve C6 and C7.
Surgical Considerations
Thoracic Outlet Syndrome
TOS arises from direct or indirect mechanical compression of the subclavian vessels or the brachial plexus between the clavicle, scalene muscles, and 1st rib. The most common clinical symptoms include fatigue, pain, and paresthesias affecting the upper extremity.[14] Diagnosis can be challenging due to dynamic, posture-dependent symptoms, which result from neurovascular compression when the upper extremity is elevated overhead. TOS should be considered in patients presenting with these symptoms, particularly if a cervical rib is present, which occurs in approximately 0.5% of the population.[15]
Case reports describe various forms of TOS associated with a hypertrophic anterior scalene muscle.[16] In some instances, resection of the anterior or middle scalene muscle (scalenectomy) is necessary. When abnormal muscle bundles compress the brachial neurovascular structures, ultrasound imaging may reveal the “wedge-sickle sign,” indicating the need for surgical intervention. In cases where TOS is directly linked to the scalene muscle, symptoms may be managed temporarily with type A botulinum toxin (Botox) injections, particularly in older patients requiring surgical delay.[17] Botox injections may also alleviate symptoms in individuals with spasmodic torticollis or cervical dystonia.
Neck Mass Dissections
Tumors can develop within the scalene muscles, including rare cases of myopericytoma.[18] Surgical removal is often required. Dissection for tumor or mass removal involves intramuscular dissection to achieve either marginal or radical resection of the tumor bed. Another rare tumor affecting the head and neck is myxoma, a mesenchymal neoplasm.[19] More commonly, benign tumors such as fibromatosis or hemangioma are found within the muscle and frequently require surgical excision.[20] Lymph node biopsies of the scalene region can help determine tumor type. In some cases, a scalenectomy may be performed to create access for the removal of deeper tumors, such as cervical schwannomas. Additionally, mass effects can result from direct trauma, leading to intramuscular hemangiomas.
Nerve Blocks and Catheter Considerations
Nerve blocks and catheters are increasingly utilized as healthcare shifts toward outpatient-based procedures.[21] Indications for nerve blocks include neurological pain management and certain depressive syndromes. Literature supports continuous interscalene blocks over single-injection blocks due to lower toxicity rates and reduced symptomatic rebound once the anesthetic wears off.[22][23] Another invasive technique is the stellate ganglion block, which involves passing a needle through multiple tissues, including the anterior and middle scalene muscles.[24]
Clinical Significance
Electromyography can assess scalene muscle function and detect contractile anomalies, aiding in the diagnosis of conditions like TOS.[25] Patients with temporomandibular joint dysfunction exhibit increased anterior scalene electrical activity compared to those without mandibular issues.[26] This finding may be valuable for physiotherapists and osteopaths, as scalene dysfunction can reduce ventilatory capacity, with mandibular disorders potentially being a symptom rather than the cause.
Hypertrophy or increased tone of the anterior scalene muscle may produce distal symptoms. Vascular compression of the subclavian artery can lead to pallor, cold sensations, cyanosis, and impaired arm function. If C5-C6 crosses the muscle in an abnormal manner, such as through hypertrophy or shortening, paresthesia, anesthesia, or weakness in the corresponding muscle groups may occur. Compression of the C8 root between 2 muscular attachments of the anterior scalene can cause tingling, pain, and weakness in the hand and interosseous muscles. Fusion of the anterior scalene tendon with the longus capitis muscle may contribute to headaches.[27]
If the suprascapular nerve traverses a hypertonic, hypertrophic, or shortened middle scalene muscle, weakness of the supraspinatus and infraspinatus muscles may result, along with paresthesia and shoulder pain, leading to scapulohumeral arthrokinematic dysfunction. Compression of the deep branch of the transverse cervical artery within the middle scalene could present with subtle symptoms, complicating diagnosis.
Increased posterior scalene thickness may alter the course of the long thoracic and dorsal scapular nerves, causing pain or weakness in the serratus anterior, levator scapulae, and rhomboid muscles. Additionally, the presence of the minimum scalene muscle may reduce space for the brachial plexus, subclavian artery, and subclavian vein, contributing to symptoms associated with TOS.[28]
Media
(Click Image to Enlarge)
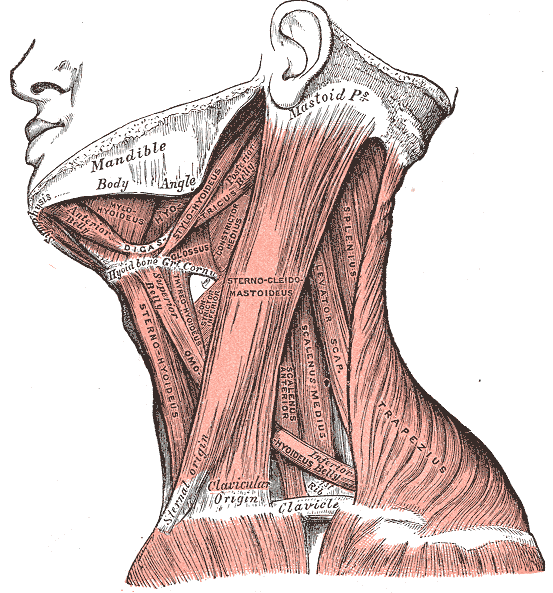
Neck Muscles. This lateral-view illustration shows the trapezius, sternocleidomastoideus, sternohyoideus, omohyoideus belly, scalenus anterior and medius, levator scapulae, splenius, mylohyoideus, thyrohyoideus, digastricus, and stylohyoideus muscles. The mandible, mastoid process, clavicle, and hyoid bone are also shown.
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
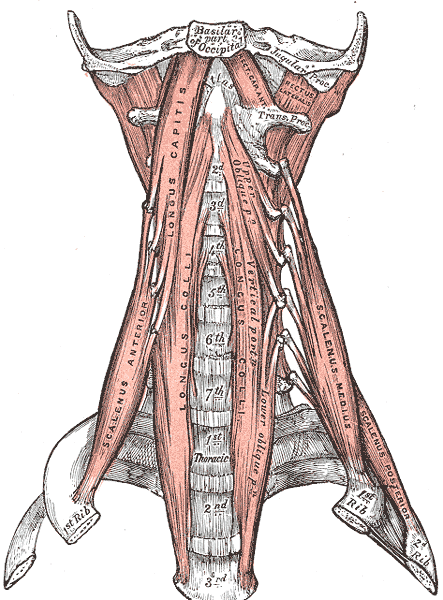
Anterior Muscles of the Neck. Anterior muscles of the neck include the basilar part of the occipital, jugular process, scalenus anterior, longus capitis, longus colli, scalenus medius and posterior, atlas, thoracic vertebrae, and cervical vertebrae.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Basoudan N, Rodrigues A, Gallina A, Garland J, Guenette JA, Shadgan B, Road J, Reid WD. Scalene and sternocleidomastoid activation during normoxic and hypoxic incremental inspiratory loading. Physiological reports. 2020 Jul:8(14):e14522. doi: 10.14814/phy2.14522. Epub [PubMed PMID: 32726513]
Feigl G, Hammer GP, Litz R, Kachlik D. The intercarotid or alar fascia, other cervical fascias, and their adjacent spaces - a plea for clarification of cervical fascia and spaces terminology. Journal of anatomy. 2020 Jul:237(1):197-207. doi: 10.1111/joa.13175. Epub 2020 Feb 20 [PubMed PMID: 32080853]
Chang KV, Wu WT, Mezian K, Naňka O, Özçakar L. Sonoanatomy revisited: the long thoracic nerve. Medical ultrasonography. 2019 Aug 31:21(3):349-352. doi: 10.11152/mu-1952. Epub [PubMed PMID: 31476216]
Natsis K, Totlis T, Didagelos M, Tsakotos G, Vlassis K, Skandalakis P. Scalenus minimus muscle: overestimated or not? An anatomical study. The American surgeon. 2013 Apr:79(4):372-4 [PubMed PMID: 23574846]
Connolly MR, Auchincloss HG. Anatomy and Embryology of the Thoracic Outlet. Thoracic surgery clinics. 2021 Feb:31(1):1-10. doi: 10.1016/j.thorsurg.2020.09.007. Epub [PubMed PMID: 33220766]
Ostrowski P, Bonczar M, Shafarenko K, Rams D, Dziedzic M, Gabryszuk K, Zarzecki M, Wojciechowski W, Walocha J, Koziej M. The thyrocervical trunk: an analysis of its morphology and variations. Anatomical science international. 2023 Mar:98(2):240-248. doi: 10.1007/s12565-022-00692-5. Epub 2022 Nov 9 [PubMed PMID: 36350499]
Su WD, Ohtsuka A, Taguchi T, Murakami T. Typology of the arteries in the human scalenus region, with special reference to the accessory ascending cervical artery. Acta medica Okayama. 2000 Dec:54(6):243-52 [PubMed PMID: 11132917]
Alabduladhem TO, Lasrado S. Anatomy, Head and Neck, Costocervical Trunk Arteries. StatPearls. 2025 Jan:(): [PubMed PMID: 32310480]
Jardaly AH, Bordoni B. Anatomy, Thorax, Thyrocervical Arteries. StatPearls. 2025 Jan:(): [PubMed PMID: 32310456]
Iwanaga J, Lofton C, He P, Dumont AS, Tubbs RS. Lymphatic System of the Head and Neck. The Journal of craniofacial surgery. 2021 Jul-Aug 01:32(5):1901-1905. doi: 10.1097/SCS.0000000000007230. Epub [PubMed PMID: 33201067]
Aheer GK, Villella J. Scalenus muscle and the C5 root of the brachial plexus: bilateral anatomical variation and its clinical significance. The Journal of the Canadian Chiropractic Association. 2021 Aug:65(2):229-233 [PubMed PMID: 34658395]
Rusnak-Smith S, Moffat M, Rosen E. Anatomical variations of the scalene triangle: dissection of 10 cadavers. The Journal of orthopaedic and sports physical therapy. 2001 Feb:31(2):70-80 [PubMed PMID: 11232741]
Collins RM, Bhana J, Patricios JS, Du Plessis A, Veller M, Schultz D, van Rensburg DC. Thoracic outlet syndrome in a patient with absent scalenus anterior muscle. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine. 2014 May:24(3):268-70. doi: 10.1097/JSM.0000000000000006. Epub [PubMed PMID: 24451700]
Panther EJ, Reintgen CD, Cueto RJ, Hao KA, Chim H, King JJ. Thoracic outlet syndrome: a review. Journal of shoulder and elbow surgery. 2022 Nov:31(11):e545-e561. doi: 10.1016/j.jse.2022.06.026. Epub 2022 Aug 10 [PubMed PMID: 35963513]
Braun RM, Shah KN, Rechnic M, Doehr S, Woods N. Quantitative Assessment of Scalene Muscle Block for the Diagnosis of Suspected Thoracic Outlet Syndrome. The Journal of hand surgery. 2015 Nov:40(11):2255-61. doi: 10.1016/j.jhsa.2015.08.015. Epub 2015 Oct 1 [PubMed PMID: 26429586]
Qaja E, Honari S, Rhee R. Arterial thoracic outlet syndrome secondary to hypertrophy of the anterior scalene muscle. Journal of surgical case reports. 2017 Aug:2017(8):rjx158. doi: 10.1093/jscr/rjx158. Epub 2017 Aug 21 [PubMed PMID: 28928918]
Level 3 (low-level) evidenceLikes K, Rochlin DH, Salditch Q, Dapash T, Baker Y, DeGuzman R, Selvarajah S, Freischlag JA. Diagnostic accuracy of physician and self-referred patients for thoracic outlet syndrome is excellent. Annals of vascular surgery. 2014 Jul:28(5):1100-5. doi: 10.1016/j.avsg.2013.12.011. Epub 2014 Jan 21 [PubMed PMID: 24462540]
Level 2 (mid-level) evidenceChaskes MB, Bishop JW, Bobinski M, Farwell DG. Myopericytoma of the Neck Originating From the Middle Scalene: A Case Report. Ear, nose, & throat journal. 2020 Aug:99(7):NP72-NP74. doi: 10.1177/0145561319839821. Epub 2019 May 29 [PubMed PMID: 31142159]
Level 3 (low-level) evidenceRachidi S, Sood AJ, Rumboldt T, Day TA. Intramuscular myxoma of the paraspinal muscles: A case report and systematic review of the literature. Oncology letters. 2016 Jan:11(1):466-470 [PubMed PMID: 26870235]
Level 1 (high-level) evidenceCho JK, Cha W, Sung MW. Intramuscular Hemangioma in the Anterior Scalene Muscle Diagnosed by Core Needle Biopsy. Clinical and experimental otorhinolaryngology. 2015 Sep:8(3):298-301. doi: 10.3342/ceo.2015.8.3.298. Epub 2015 Aug 13 [PubMed PMID: 26330928]
de Boer AS, Mintjes-de Groot AJ, Severijnen AJ, van den Berg JM, van Pelt W. Risk assessment for surgical-site infections in orthopedic patients. Infection control and hospital epidemiology. 1999 Jun:20(6):402-7 [PubMed PMID: 10395141]
Level 3 (low-level) evidenceSalviz EA, Xu D, Frulla A, Kwofie K, Shastri U, Chen J, Shariat AN, Littwin S, Lin E, Choi J, Hobeika P, Hadzic A. Continuous interscalene block in patients having outpatient rotator cuff repair surgery: a prospective randomized trial. Anesthesia and analgesia. 2013 Dec:117(6):1485-92. doi: 10.1213/01.ane.0000436607.40643.0a. Epub [PubMed PMID: 24257398]
Level 1 (high-level) evidenceBrockmeier S. Continuous interscalene block provided superior analgesic control through the first postoperative week after rotator cuff repair. The Journal of bone and joint surgery. American volume. 2014 Nov 19:96(22):1924. doi: 10.2106/JBJS.9622.ebo323. Epub [PubMed PMID: 25410514]
Kirkpatrick K, Khan MH, Deng Y, Shah KB. A Review of Stellate Ganglion Block as an Adjunctive Treatment Modality. Cureus. 2023 Feb:15(2):e35174. doi: 10.7759/cureus.35174. Epub 2023 Feb 19 [PubMed PMID: 36949968]
Silva Junior EFFD, Campos SL, Leite WS, Melo PVS, Lins RAC, Araújo MDGR, Guerino MR. Surface electromyography signal processing and evaluation on respiratory muscles of critically ill patients: A systematic review. PloS one. 2023:18(4):e0284911. doi: 10.1371/journal.pone.0284911. Epub 2023 Apr 27 [PubMed PMID: 37104255]
Level 1 (high-level) evidenceArmijo-Olivo S, Silvestre R, Fuentes J, da Costa BR, Gadotti IC, Warren S, Major PW, Thie NM, Magee DJ. Electromyographic activity of the cervical flexor muscles in patients with temporomandibular disorders while performing the craniocervical flexion test: a cross-sectional study. Physical therapy. 2011 Aug:91(8):1184-97. doi: 10.2522/ptj.20100233. Epub 2011 Jun 9 [PubMed PMID: 21659465]
Level 2 (mid-level) evidenceJull G. Cervicogenic headache. Musculoskeletal science & practice. 2023 Aug:66():102787. doi: 10.1016/j.msksp.2023.102787. Epub 2023 Jun 3 [PubMed PMID: 37301672]
Pitcher GS, Sen I, Mendes BC, Shuja F, DeMartino RR, Bower TC, Kalra M, Harmsen WS, Colglazier JJ. Thirty-year single-center experience with arterial thoracic outlet syndrome. Journal of vascular surgery. 2022 Aug:76(2):523-530. doi: 10.1016/j.jvs.2022.03.870. Epub 2022 Apr 1 [PubMed PMID: 35378247]