Introduction
Historically, cardiovascular research has gravitated toward the arterial vasculature that supplies oxygenated blood to cardiac myocytes. As biomedical technology advances, the downstream network of postcapillary coronary veins has gained further clinical relevance. The advent and improvement of cardiac interventions such as resynchronization therapy and retrograde cardioplegia make use of the coronary venous network’s close anatomical association with clinically valuable structures. The coronary venous network drains deoxygenated blood from the myocardium into one of two systems: the greater cardiac venous system and the smaller cardiac venous system. These systems are comprised of many complementary veins, the majority of which coalesce to form the coronary sinus. The coronary sinus is the major venous tributary of the greater cardiac venous system; it is responsible for draining most of the deoxygenated blood leaving the myocardium. Given the advancement of interventional cardiac procedures, a comprehensive appreciation of the coronary sinus is essential for furthering the medical care of future cardiovascular patients.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
At a length varying from 3 to 5 cm and a caliber of 1 cm, the coronary sinus is the largest coronary vein. It arises along the posterior aspect of the heart between the left atrium and the left ventricle. From there, it continues along the left posterior atrioventricular groove before emptying into the posteroinferior aspect of the right atrium, just medial to the entrance of the inferior vena cava and superior to the septal leaflet of the tricuspid valve.
The coronary sinus is a product of many venous tributaries. The origin of the coronary sinus is marked by the coalescence of the great cardiac vein and oblique vein of the left atrium (oblique vein of Marshall). Immediately downstream, the posterior vein of the left ventricle, middle cardiac vein, and small cardiac vein drain into the coronary sinus, respectively, just before it terminates at the right atrium.[1][2]
In summary, the following tributaries drain into the coronary sinus:
- Great cardiac vein
- Oblique vein of the left atrium
- Posterior vein of the left ventricle
- Middle cardiac vein
- Small cardiac vein
All tributaries, except for the oblique vein of the left atrium, contain valves at their junction with the coronary sinus. Located at the endpoint of the Great Cardiac Vein, the Vieussens Valve marks the origin of the coronary sinus. The coronary sinus continues along the left atrioventricular groove until it reaches the Thebesian valve, which is located at the orifice of the coronary sinus as it drains into the right atrium. The Thebesian valve prevents regurgitant blood flow from the right atrium from entering the coronary sinus during diastole.[3]
As the major tributary of the greater cardiac venous system, the coronary sinus returns approximately 55% of the coronary blood supply into the right atrium. The anterior cardiac veins, which range in numbers between 2 and 5, drain approximately 35% of the coronary blood supply into the right atrium. The remaining 10% is returned by the smallest cardiac veins (Thebesian veins), which drain into any of the four cardiac chambers.[4]
Embryology
In week 3 of embryonic development, the primitive heart tube differentiates into two separate structures. The primordial atrium persists to form the left and right atria, while the sinus venosus develops right and left horns. The primordial IVC and SVC drain into the right horn, which eventually is absorbed by the enlarging right atrium. The left horn persists to form the coronary sinus and its contiguous tributaries.[5]
Blood Supply and Lymphatics
The walls of the coronary sinus receive their supply of oxygenated blood and nutrients via the coronary vasa vasorum. The coronary vasa vasorum, or "the vessels of vessels," is a network of microvessels that branches off of the coronary arteries.[6]
Nerves
The coronary sinus undergoes autonomic regulation by the sympathetic nervous system (SNS) and parasympathetic nervous system (PNS), which are both regulated by the medulla in the brainstem. The SNS and PNS respectively vasodilate and vasoconstrict the coronary sinus in an opposing fashion.[7]
Muscles
The myocardial sleeve covering the coronary sinus is composed of striated cardiac muscle that runs continuously from both the right and left atria. Because myocardial tissue is innately arrhythmogenic, ectopic foci such as those seen in atrial fibrillation may potentially develop from tissue surrounding the coronary sinus.[8]
Physiologic Variants
The anatomical variants of the coronary sinus are manifold, ranging from the number of contiguous tributaries to the morphology of luminal valves. While the majority of anatomical variants are benign, some hold clinical implications for cardiac procedures. The presence of anomalous valves in the coronary sinus may hinder cardiac intervention techniques such as defibrillator lead implantation or retrograde cardioplegia.[4][9][10]
A persistent left superior vena cava (PLSVC) is a rare physiologic variation of the thoracic venous system in which the left brachiocephalic vein fails to develop. Venous blood from the left arm, head, and neck drains directly into the coronary sinus before entering the right atrium. Although PLSVC is clinically silent in isolation, it is commonly associated with other high-risk cardiac defects.[11]
Surgical Considerations
The location of the coronary sinus within the right atrium allows convenient access to the myocardial capillary network. Clinicians use this access in retrograde cardioplegia, a procedure in which paralytic agents are delivered retrogradely through the coronary sinus and its tributaries to the myocardium during cardiac surgery. Retrograde cardioplegia is now commonly used in conjunction with the classical anterograde approach, in which cardioplegic agents are administered through the coronary ossia into the coronary arteries. The concomitant use of retrograde cardioplegia with anterograde cardioplegia accounts for the risk of significant arterial stenoses that may prevent cardioplegic agents from reaching the myocardium at adequate doses. The use of both approaches has shown a superior return of postop myocardial function than the use of anterograde cardioplegia alone. Limitations to retrograde cardioplegia include PLSVC, in which cardioplegic agents may unintentionally reach the systemic circulation. A rare, albeit major complication of retrograde cardioplegia is that of coronary sinus rupture.[12]
Clinical Significance
The anatomical location of the coronary sinus provides a vital role in cardiac resynchronization therapy. A biventricular pacemaker is a device commonly used to treat a delay in ventricular contractions in those with advanced heart failure with an ejection fraction <35%. A pulse generator is implanted under the skin and utilizes 2 or 3 leads that are advanced into the heart to depolarize the ventricles in synchrony. The right lead is commonly placed in an anterior cardiac vein to pace the right ventricle, while the left lead is commonly placed in the coronary sinus to pace the left ventricle.[13]
From a cardiac electrophysiology standpoint, the coronary sinus serves as a site for electrode placement during mapping and ablation of left-sided accessory pathways. The coronary sinus is also of interest because its superficial myocardial sleeve is electrophysiologically active and may develop spontaneous arrhythmogenic foci.[14][15]
Media
(Click Image to Enlarge)
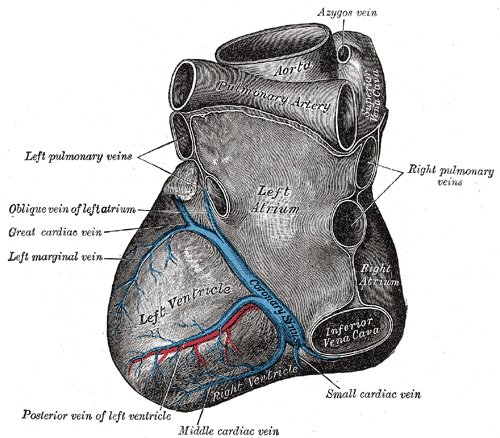
Anatomy of the Heart from the Left, Left Atrium, Left Ventricle, Azygos vein, Aorta, Coronary Sinus, Posterior vein of left ventricle, Oblique vein of left atrium, Cardiac vein, Left marginal vein
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
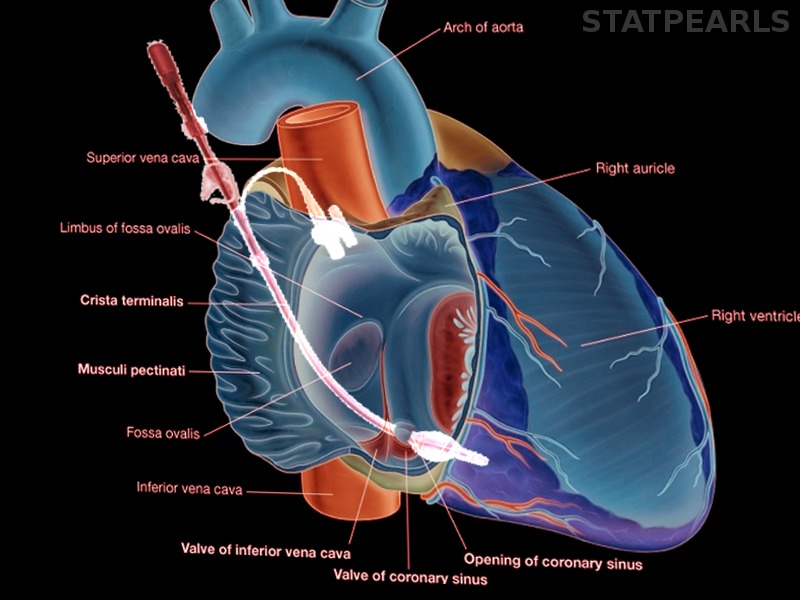
(Click Image to Enlarge)

Coronary sinus opening Image courtesy S Bhimji MD
(Click Image to Enlarge)
Retrograde cardioplegia Image courtesy S Bhimji MD
References
Loukas M, Bilinsky S, Bilinsky E, el-Sedfy A, Anderson RH. Cardiac veins: a review of the literature. Clinical anatomy (New York, N.Y.). 2009 Jan:22(1):129-45. doi: 10.1002/ca.20745. Epub [PubMed PMID: 19097063]
Ortale JR, Gabriel EA, Iost C, Márquez CQ. The anatomy of the coronary sinus and its tributaries. Surgical and radiologic anatomy : SRA. 2001:23(1):15-21 [PubMed PMID: 11370136]
Mazur M, Kuniewicz M, Klimek-Piotrowska W, Kucharska A, Mizia E, Mróz I, Wandzel-Loch B. Human coronary sinus - from Galen to modern times. Folia medica Cracoviensia. 2015:55(1):5-15 [PubMed PMID: 26774627]
Goodwill AG, Dick GM, Kiel AM, Tune JD. Regulation of Coronary Blood Flow. Comprehensive Physiology. 2017 Mar 16:7(2):321-382. doi: 10.1002/cphy.c160016. Epub 2017 Mar 16 [PubMed PMID: 28333376]
von Lüdinghausen M. The venous drainage of the human myocardium. Advances in anatomy, embryology, and cell biology. 2003:168():I-VIII, 1-104 [PubMed PMID: 12645157]
Level 3 (low-level) evidenceRitman EL, Lerman A. The dynamic vasa vasorum. Cardiovascular research. 2007 Sep 1:75(4):649-58 [PubMed PMID: 17631284]
Level 3 (low-level) evidenceKapa S, DeSimone CV, Asirvatham SJ. Innervation of the heart: An invisible grid within a black box. Trends in cardiovascular medicine. 2016 Apr:26(3):245-57. doi: 10.1016/j.tcm.2015.07.001. Epub 2015 Jul 9 [PubMed PMID: 26254961]
Antz M, Otomo K, Arruda M, Scherlag BJ, Pitha J, Tondo C, Lazzara R, Jackman WM. Electrical conduction between the right atrium and the left atrium via the musculature of the coronary sinus. Circulation. 1998 Oct 27:98(17):1790-5 [PubMed PMID: 9788835]
Level 3 (low-level) evidenceKaraca M, Bilge O, Dinckal MH, Ucerler H. The anatomic barriers in the coronary sinus: implications for clinical procedures. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2005 Nov:14(2):89-94 [PubMed PMID: 16374555]
Corcoran SJ, Lawrence C, McGuire MA. The valve of Vieussens: an important cause of difficulty in advancing catheters into the cardiac veins. Journal of cardiovascular electrophysiology. 1999 Jun:10(6):804-8 [PubMed PMID: 10376917]
Pahwa R, Kumar A. Persistent left superior vena cava: an intensivist's experience and review of the literature. Southern medical journal. 2003 May:96(5):528-9 [PubMed PMID: 12911199]
Level 3 (low-level) evidenceGundry SR, Kirsh MM. A comparison of retrograde cardioplegia versus antegrade cardioplegia in the presence of coronary artery obstruction. The Annals of thoracic surgery. 1984 Aug:38(2):124-7 [PubMed PMID: 6465990]
Level 3 (low-level) evidenceMedical Advisory Secretariat. Biventricular pacing (cardiac resynchronization therapy): an evidence-based analysis. Ontario health technology assessment series. 2005:5(13):1-60 [PubMed PMID: 23074464]
Chen YA, Nguyen ET, Dennie C, Wald RM, Crean AM, Yoo SJ, Jimenez-Juan L. Computed tomography and magnetic resonance imaging of the coronary sinus: anatomic variants and congenital anomalies. Insights into imaging. 2014 Oct:5(5):547-57. doi: 10.1007/s13244-014-0330-8. Epub 2014 Jul 22 [PubMed PMID: 25048808]
Habib A, Lachman N, Christensen KN, Asirvatham SJ. The anatomy of the coronary sinus venous system for the cardiac electrophysiologist. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2009 Nov:11 Suppl 5():v15-21. doi: 10.1093/europace/eup270. Epub [PubMed PMID: 19861386]