Introduction
Fetal circulation is unlike adult circulation as it uses physiological shunts to carry oxygenated blood to tissues and bypass developing organs. The viability of the fetus heavily relies on these shunts to adequately perfuse developing tissues and organs, especially the brain and heart. The ductus venosus is a shunt that allows oxygenated blood in the umbilical vein to bypass the liver and is essential for normal fetal circulation.[1] Blood becomes oxygenated in the placenta and travels to the right atrium via umbilical veins through the ductus venosus, then to the inferior vena cava.[1] This oxygenated blood then passes through the foramen ovale, an opening between the atria, into the left atrium to be distributed systemically.[1] Therefore, the ductus venosus plays a key role in maintaining this unique circulation pattern. Fetal circulation studies are done via Doppler ultrasound or MRI to ensure proper blood flow through these shunts.[2] If there is impedance or absence of flow through these shunts, it may correlate with aneuploidies, cardiac defects, and/or other postpartum disease states.[3] Postpartum, the ductus venosus closes, secondary to increased cardiac pressures and decreased circulating prostaglandins.[4] The ductus venosus is critical for proper fetal circulation, but disruption of flow in utero or failure to close this shunt postpartum can lead to many adverse antenatal and perinatal outcomes.
Development
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Development
During fetal development, when fetal-placental circulation gets established, blood flow between the fetus and placenta occurs through the paired umbilical arteries and the unpaired single umbilical vein. The umbilical vein directs oxygenated blood from the placenta towards the fetus, and the umbilical arteries carry deoxygenated blood back to the placenta (see figure). When the umbilical vein enters the fetal umbilicus, it branches into a large ductus venosus and a small portal sinus. The ductus venosus carrying oxygenated blood enters the inferior vena cava directly and subsequently empties the well-oxygenated blood into the left side of the heart through the foramen ovale between the right and the left atrium. The small portal sinus supplies the liver itself with oxygenated blood, which returns to the inferior vena cava with deoxygenated blood through the hepatic vein.[5]
Fetal rat liver models illustrate the development of the hepatic vascular system by gestation day 14 with one ductus venous in the liver parenchyma.[6] At this time, this shunt connects the terminal, bulging portion of the umbilical vein to the posterior inferior vena cava.[6] The ductus venosus and the umbilical vein degenerate during the perinatal period.[6] The orifice of the ductus venosus narrows and closes at birth due to decreased blood flow and pressure through the shunt.[7] The permanent closure of this shunt begins days postpartum and finishes after 1 to 3 months and consists of connective tissue.[7] At birth, the remnant of the ductus venosus gradually develops into a ligament called the ligamentum venosum.
Function
The primary function of the ductus venosus is to carry oxygenated blood from the umbilical vein to the inferior vena cava and, ultimately, the left heart for systemic circulation while the portal sinus supplies oxygenated blood to the liver itself.[1] The degree of shunting through the ductus venosus varies based on pressure and resistance differences in the liver.[7] The compression of the umbilical vein during hepatic development is why the ductus venosus is necessary to shunt blood to inferior vena cava.[8] If the shunt is not present or patent in utero, this can lead to hypoxia due to umbilical vein compression leading to a poor venous return of oxygenated blood to the heart.
Testing
In utero, ductus venosus blood flow waveforms are assessed using Doppler ultrasound to determine the patency of the shunt. It is recommended to use two positions for optimal results.[8]
1. A midsagittal view with the fetus supine to identify the ductus venosus, umbilical vein, and inferior vena cava.
2. A transverse plane abdominal Doppler to identify the ductus venosus.
Flow patterns may vary even in normal pregnancies.[9] According to one study, each trimester correlates with a classic blood flow pattern, with an increased frequency of aberrancy in each subsequent trimester.[9] Therefore, assessing fetal circulation is complicated as normal pregnancies have been shown to display seven different flow patterns.[9] A normal ductus venosus waveform contains two alternating peaks and two alternating troughs.[8] Assessing variations in these peaks and troughs aid in screening and detection of congenital heart defects, aneuploidies, and fetal growth restriction.[8]
Pathophysiology
Abnormal fetal venous circulation is observable in patients with the absence of the ductus venosus with the main abnormalities being[10]:
- Umbilical vein bypasses the hepatic system and draining into the right atrium
- Umbilical vein connects directly to the inferior vena cava via iliac veins
- Umbilical vein drains into the portal circulation
Researchers have noted that decreased or abnormal blood flow through the ductus venosus during the first trimester has links with aneuploidies such as trisomy 13, 18, 21, and Turner syndrome.[11] Therefore, Doppler during the first trimester is a beneficial screening tool for these conditions. Abnormal ductus venosus waveforms during atrial contraction are also associated with a three-fold increase in congenital heart defects.[12] Early fetal growth restriction can also be identified in the second trimester using ductus venosus Doppler, which shows increased shunting to preserve cerebral and cardiac blood flow.[8]
Clinical Significance
The absence or dysfunction of the ductus venosus can lead to various disease states, fetal anomalies, and adverse outcomes. The absence of this shunt is associated with fetal hydrops, chromosomal aberration, in utero heart failure, and portal vein absence.[10] Abnormal blood flow through the ductus venosus, assessed using Doppler, increases the risk of cardiovascular defects, fetal growth restriction, renal anomaly, perinatal death, and aneuploidy.[13]
Failure of this shunt to close postpartum leads to a condition called patent ductus venosus, which may lead to galactosemia, hypoxemia, hepatic dysfunction, and encephalopathy with hyperammonemia.[4] A patent ductus venosus pathophysiologically functions like a portal-systemic venous shunt. Depending on the size and the pressure within the shunt, the consequences may vary from entirely asymptomatic to hepatic dysfunction, portal hypertension, hyperammonemia, and hepatic encephalopathy. A patent ductus venosus is rare and managed surgically to prevent those anomalies mentioned above. Coil embolization or catheter closure may be considered.[14] Surgical correction should result in normalization of liver function tests due to restored blood flow.[14]
Rare familial cases of patients with liver disease were found to have a patent ductus venosus, which suggests an autosomal recessive inheritance pattern.[15] A hereditary case of patent ductus venosus may be considered in patients who present with hepatic dysfunction and encephalopathy of unknown etiology.[15]
Maternal diabetes may also adversely affect flow through the ductus venosus with an increased risk for fetal macrosomia and perinatal complications.[16] Fetuses of diabetic mothers have been shown to have decreased blood flow through the ductus venosus, especially in the third trimester.[16] This decreased shunting can lead to hypoxia during the perinatal period.[16]
Media
(Click Image to Enlarge)
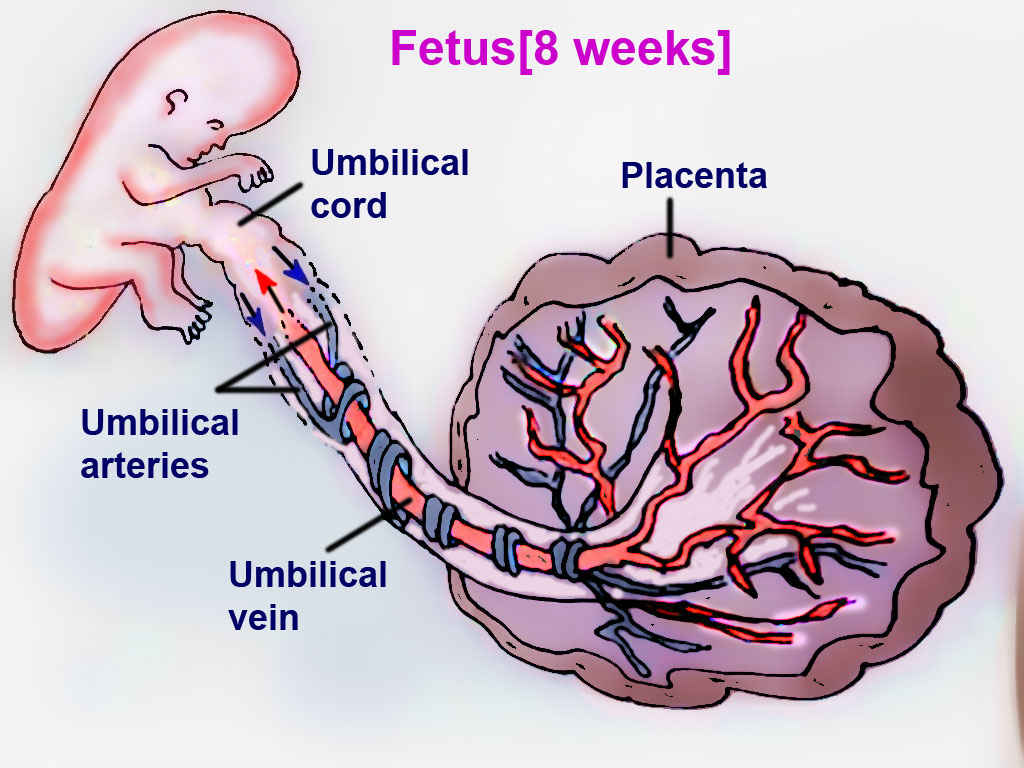
Fetal Circulation
Contributed by T Silappathikaram
(Click Image to Enlarge)
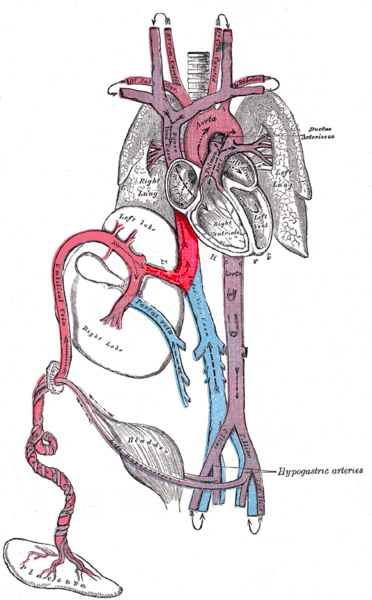
Ductus venosus connecting to the IVC Henry Gray (1918). Anatomy of the Human Body. Revised by Warren H. Lewis. Public domain. Image courtesy: https://commons.wikimedia.org/wiki/File:Gray502.png
References
Remien K, Majmundar SH. Physiology, Fetal Circulation. StatPearls. 2023 Jan:(): [PubMed PMID: 30969532]
Morton SU, Brodsky D. Fetal Physiology and the Transition to Extrauterine Life. Clinics in perinatology. 2016 Sep:43(3):395-407. doi: 10.1016/j.clp.2016.04.001. Epub 2016 Jun 11 [PubMed PMID: 27524443]
Braga M, Moleiro ML, Guedes-Martins L. Clinical Significance of Ductus Venosus Waveform as Generated by Pressure- volume Changes in the Fetal Heart. Current cardiology reviews. 2019:15(3):167-176. doi: 10.2174/1573403X15666190115142303. Epub [PubMed PMID: 30644348]
Poeppelman RS, Tobias JD. Patent Ductus Venosus and Congenital Heart Disease: A Case Report and Review. Cardiology research. 2018 Oct:9(5):330-333. doi: 10.14740/cr777w. Epub 2018 Oct 7 [PubMed PMID: 30344833]
Level 3 (low-level) evidenceMarty M, Kerndt CC, Lui F. Embryology, Fetal Circulation. StatPearls. 2023 Jan:(): [PubMed PMID: 30725834]
Nasu T, Arishima K. Development of the ductus venosus in the SD rat. Fukuoka igaku zasshi = Hukuoka acta medica. 2004 Jan:95(1):9-16 [PubMed PMID: 15031995]
Level 3 (low-level) evidenceEdelstone DI. Regulation of blood flow through the ductus venosus. Journal of developmental physiology. 1980 Aug:2(4):219-38 [PubMed PMID: 7012226]
Level 3 (low-level) evidenceTuran S, Turan OM. Harmony Behind the Trumped-Shaped Vessel: the Essential Role of the Ductus Venosus in Fetal Medicine. Balkan medical journal. 2018 Mar 15:35(2):124-130. doi: 10.4274/balkanmedj.2017.1389. Epub [PubMed PMID: 29553462]
Gürses C, Karadağ B, İsenlik BST. Normal variants of ductus venosus spectral Doppler flow patterns in normal pregnancies. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2020 Apr:33(8):1288-1294. doi: 10.1080/14767058.2018.1517323. Epub 2018 Oct 1 [PubMed PMID: 30153762]
Contratti G, Banzi C, Ghi T, Perolo A, Pilu G, Visentin A. Absence of the ductus venosus: report of 10 new cases and review of the literature. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2001 Dec:18(6):605-9 [PubMed PMID: 11844198]
Level 2 (mid-level) evidenceMaiz N, Valencia C, Kagan KO, Wright D, Nicolaides KH. Ductus venosus Doppler in screening for trisomies 21, 18 and 13 and Turner syndrome at 11-13 weeks of gestation. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2009 May:33(5):512-7. doi: 10.1002/uog.6330. Epub [PubMed PMID: 19338027]
Maiz N, Plasencia W, Dagklis T, Faros E, Nicolaides K. Ductus venosus Doppler in fetuses with cardiac defects and increased nuchal translucency thickness. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2008 Mar:31(3):256-60. doi: 10.1002/uog.5262. Epub [PubMed PMID: 18307193]
Level 2 (mid-level) evidenceOh C, Harman C, Baschat AA. Abnormal first-trimester ductus venosus blood flow: a risk factor for adverse outcome in fetuses with normal nuchal translucency. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2007 Aug:30(2):192-6 [PubMed PMID: 17518423]
Level 2 (mid-level) evidenceAraki T, Kamada M, Okamoto Y, Arai S, Oba O. Coil embolization of a patent ductus venosus in a 52-day-old girl with congenital heart disease. The Annals of thoracic surgery. 2003 Jan:75(1):273-5 [PubMed PMID: 12537231]
Level 3 (low-level) evidenceJacob S, Farr G, De Vun D, Takiff H, Mason A. Hepatic manifestations of familial patent ductus venosus in adults. Gut. 1999 Sep:45(3):442-5 [PubMed PMID: 10446116]
Level 3 (low-level) evidenceLund A, Ebbing C, Rasmussen S, Kiserud T, Kessler J. Maternal diabetes alters the development of ductus venosus shunting in the fetus. Acta obstetricia et gynecologica Scandinavica. 2018 Aug:97(8):1032-1040. doi: 10.1111/aogs.13363. Epub 2018 Jun 20 [PubMed PMID: 29752712]