Introduction
The femoral or thigh region of the lower limb is bounded proximally by the hip and distally by the knee (see Image. Right Femur Anatomy, Posterior Surface). Connective tissue septae divide this region into 3 muscle compartments: anterior, posterior, and medial. Femoral muscles contribute to the hip and knee's range of motion.[1] The lower limb's major neurovascular structures pass through the femoral compartments before entering or exiting the pelvis.[2]
Most thigh injuries arise from trauma or overuse. Surgically necessary femoral procedures include knee replacements and fracture repairs. The femoral compartment is paramount in orthopedic surgery due to its role in knee joint stability and weight-bearing. Understanding this compartment's anatomy allows clinicians to perform interventions effectively and optimize patient outcomes.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The Femur and Its Articulations
The "femoral region" is appropriately named, as this region surrounds the femur or thigh bone. The area extends between the femur's proximal articulation with the pelvis at the hip joint and distal articulation with the tibia and patella at the knee joint.[3]
The femur is a long bone, the longest in the human body. The femoral head articulates superomedially with the acetabulum. The acetabular fossa and cartilaginous lunate surface receive the femoral head at the hip joint.
The ligaments supporting the hip joint include the ligament of the head of the femur (ligamentum capitis femoris or ligamentum teres) and the joint capsule's iliofemoral, ischiofemoral, and pubofemoral ligaments. (see Image. Right Proximal Femur Anatomy). Within the ligament of the femoral head lies the foveal artery that serves the acetabular labrum and surrounding joint capsule.[4]
The femoral neck extends inferolaterally from the head and connects the femoral head to the femoral shaft (diaphysis or body). The greater and lesser trochanters are bony protuberances situated laterally and posteromedially, respectively, at the femoral neck and body's junction.
The femoral shaft is a long, cylindrical bone possessing a raised vertical structure along its posterior aspect, the linea aspera. The medial and lateral condyles are inferior femoral expansions that articulate with the medial and lateral tibial plateaus at the knee joint.[5]
The knee articulation is supported by the medial and lateral menisci and several ligaments, including the anterior and posterior cruciate, tibial (medial) collateral, fibular (lateral) collateral, and patellar ligaments. The patellar ligament is the infrapatellar portion of the quadriceps tendon.[6]
Proximal Lower Limb Function
The lower extremity is designed to support body weight and an erect posture as humans assume bipedal locomotion. The femoral region transmits weight from the pelvic girdle to the knee, legs, and feet. Each femur angulates at the trochanters and is oriented inferomedially from the hip to the knee.
The thigh plays a significant role in gait and locomotion due to its involvement in several movements and functions:
- The thigh muscles work synergistically to control movements at the lower limb joints, ensuring proper weight distribution and balance throughout the gait cycle.
- The quadriceps muscle propels the body forward during the stance phase of gait and provides stability and lower limb control during weight-bearing activities.
- The iliopsoas and rectus femoris contribute to hip flexion, allowing the leg to swing forward during the swing phase of gait.
- The gluteus maximus and hamstrings facilitate forward body movement during walking or running.
- The thigh muscles and soft tissues help control and absorb the shock generated during ground contact with each step. This shock absorption mechanism reduces impact forces transmitted through the lower limb joints and contributes to smooth and efficient locomotion.
- During the swing phase of gait, the thigh muscles lift and clear the foot from the ground, allowing for unimpeded forward movement.
- The thigh muscles dynamically adjust their activity and force output to adapt to changes in terrain, incline, or surface irregularities encountered during locomotion.
- Efficient thigh muscle coordination and activation minimize unnecessary movements and maximize mechanical advantage to conserve energy and reduce fatigue during prolonged activities.
Dysfunction or impairment of the thigh muscles can significantly impact an individual's ability to walk, run, or perform other activities of daily living.
Embryology
The incipient limb buds form during week 4 of embryonic development, with the upper limb buds appearing ahead of their inferior counterparts. Each limb bud's distal end contains apical ectodermal ridge tissue that mediates limb development and differentiation through week 8.[7] Limb bud mesodermal layers organize into what is known as the zone of polarizing activity, which produces the sonic hedgehog gene product. This protein activates the genes for the bone morphogenetic protein and Hoxd-9 through Hoxd-13. These genes help modulate proper limb growth and elongation.[8]
Initially, the lower limb buds grow along the coronal plane. By weeks 6 to 8, the lower limb buds start growth along the sagittal plane and rotate internally until the knee faces anteriorly.[7] The growth and differentiation of various limb structures proceed as described below.
Vasculature
The external iliac artery and a branch of the umbilical artery known as the axis artery (sciatic artery) develop in parallel. The femoral artery arises from the external iliac artery as the lower limb bud lengthens. The profunda femoris artery later arises from the femoral artery. The axis artery gives rise to the anterior tibial artery, which branches into the dorsalis pedis and posterior tibial arteries. The axis artery eventually regresses after contributing fully developed arterial structures, including the inferior gluteal, sciatic, proximal popliteal, and distal peroneal arteries.[9]
Muscle and Nervous Tissue
The developing lower limb musculature arises from mesoderm found in somites L1 to S2—areas served by the developing L2 to S3 ventral primary rami. Somitic mesodermal extension follows lower limb growth. The nerves segregate into the anterior and posterior divisions as mesodermal condensations form the corresponding muscular compartments.
The anterior mesodermal condensation later becomes the hip flexors and adductors. The posterior mesodermal condensation develops into the hip extensor and abductors. Meanwhile, the developing anterior thigh nerves later give rise to the tibial and obturator nerves. The growing posterior thigh nerves become the superior and inferior gluteal, femoral, and common fibular (peroneal) nerves.[10]
Bone Formation
The lateral plate mesoderm gives rise to most lower limb bones, including the femur. The femur undergoes endochondral ossification. The lateral plate mesoderm condenses and forms hyaline cartilage structures from weeks 5 to 6 of development. By weeks 7 to 9, primary ossification centers begin to form in the developing femur and tibia. The diaphysis continues development from week 9 to birth, while the epiphysis remains cartilaginous. Secondary ossification centers develop from birth onwards to form the epiphyseal plates, separated from the diaphysis by the metaphysis[11].
Blood Supply and Lymphatics
The external iliac artery's lower limb branches largely supply the femoral region. The external iliac artery exits the pelvis, traversing deep to the inguinal ligament, where it continues as the femoral artery. The femoral artery then enters the femoral triangle lateral to the femoral vein and deep inguinal lymph nodes in the femoral canal. The femoral artery and vein comprise the main vasculature of the femoral region and leg.
The common femoral artery is the part of the femoral artery between the inguinal ligament and profunda femoris' origin. This segment forms the 3 significant branches discussed below.
- The femoral artery arises distal to the profunda femoris' origin. This segment enters the adductor canal along the lateral border of the pectineus muscle and lies deep to the sartorius muscle within the anterior compartment. The femoral artery then exits the adductor hiatus, becoming the popliteal artery. This segment is sometimes referred to as the "superficial femoral artery."
- The profunda femoris is also known as the deep artery of the thigh or deep femoral artery. This blood vessel is the femoral region's primary arterial supply. The deep femoral artery arises from the femoral artery within the femoral triangle. This blood vessel passes deep to the adductor longus muscle, giving off branches supplying the adductor magnus and hamstring muscles in the posterior compartment. The medial femoral circumflex artery usually arises from the profunda femoris but sometimes diverges directly from the femoral artery.
- The lateral circumflex femoral artery is a branch that may arise lateral to or directly from the profunda femoris. This blood vessel typically diverges superficial to the hip joint capsule. The lateral circumflex femoral artery's branches wrap posteriorly around the proximal femoral shaft to supply the femoral head. A descending branch spirals around the inferolateral thigh to supply the region's muscles.[12]
The femoral vein and its tributaries return blood from the femoral region and lower limb via a similar, reverse path to the related arteries. The femoral vein follows the femoral artery, the profunda femoris vein follows the profunda femoris artery, and the lateral circumflex femoral veins follow the lateral circumflex femoral arteries.
The great saphenous vein is a major superficial vein of the lower limb that returns venous blood to the femoral vein. The great saphenous vein exits the leg to enter the thigh just posterior to the medial femoral condyle. The vein then rises through the femoral region, superficial to the fascia lata, before entering the saphenous opening and emptying into the femoral vein.[13][14]
Superficial lymphatic channels follow the great saphenous vein, typically draining into the superficial inguinal lymph nodes. These nodes extend superiorly toward the anterior superior iliac spine and inferiorly along the proximomedial thigh.[15] Deep thigh lymphatic channels follow the deep veins to empty into the deep inguinal lymph nodes.
Nerves
Nerves supplying the thigh branch out from the lumbosacral plexus. These nerves include the following:[16][17][18]
- The lateral femoral cutaneous nerve arises from the L2 to L3 roots and enters the thigh deep to the inguinal ligament. This nerve conveys sensation from the anterolateral thigh.
- The obturator nerve forms from the L2 to L4 nerves. The obturator nerve and its anterior and posterior branches innervate the medial thigh compartment muscles. This nerve also transmits sensory information from the medial thigh and femoral condylar areas.[19]
- The femoral nerve arises from the L2 to L4 rami. This thick nerve enters the thigh deep to the inguinal ligament and lateral to the femoral vessels. The femoral nerve divides into numerous muscular and cutaneous branches within the anterior thigh. The muscular branches supply the anterior thigh compartment muscles. The cutaneous branches relay anterior thigh sensory information to the spinal cord. The anterior femoral cutaneous nerve is a femoral nerve branch that transmits sensation from the anteromedial thigh.
- The saphenous nerve has contributions from the L2 to L4 roots, though it arises from the femoral nerve inferior to the femoral triangle. The saphenous nerve follows the femoral artery and vein in the adductor canal deep to the sartorius muscle.[20]
- The sciatic nerve arises from the L4 to S3 nerves. The sciatic nerve is the largest in the human body. This nerve supplies the posterior thigh compartment muscles. The branches of this nerve originating from the popliteal fossa and supplying the leg are the tibial and fibular nerves.
- The posterior femoral cutaneous nerve has contributions from the S1 to S3 roots and is often called the "posterior cutaneous nerve of the thigh." This nerve conveys sensation from the posterior thigh.
The dermatomes are segmental strips of skin with cutaneous innervation from a single spinal nerve level (see Image. Dermatome Map). Femoral dermatomal patterns wrap around the anterior thigh from superolateral to inferomedial and around the posterior thigh from superomedial to inferior. Dermatome maps vary individually due to the presence of both autonomous and overlapping dermatomes.
The L1 dermatome includes only the superior medial thigh and inguinal regions. Nerves L2 to L4 innervate the anterior femoral region. The L2 dermatome spans the inguinal ligament and anterior and inferomedial thigh regions. L3 supplies the anterior and medial thigh over the medial epicondyle. L4 innervates the inferoanterior thigh over the anteromedial knee aspect before descending medially into the leg. The L5 to S2 nerves supply the posterior thigh. The L5 dermatome includes the posterolateral femoral region. The S1 and S2 nerves innervate the posterior thigh. The S3 and S4 dermatomes span the medial gluteal cleft margin and perianal territory, respectively.
Muscles
Femoral muscles move the hip and knee joints (see Image. Right Hip and Femoral Muscles, Anterior View). These muscles are divided into 3 compartments: anterior, medial, and posterior. Muscles in the same compartment generally move in the same direction and are supplied by the same neurovascular structures.
Anterior Thigh Muscles
Anterior thigh muscles are the main hip flexors and knee extensors. The femoral nerve (L2-L4) innervates most of this compartment's muscles, which are discussed below. The tensor fascia lata is widely considered a gluteal muscle, though partly located in this region.
- The pectineus originates from the superior pubic ramus and distally attaches to an area inferior to the lesser trochanter. The pectineus flexes, adducts, and medially rotates the hip. This muscle receives motor innervation from both the femoral and obturator nerves in some individuals.
- The ilopsoas is composed of the iliacus, psoas major, and psoas minor. The iliacus' proximal attachment is broad, extending across the iliac crest, iliac fossa, superior sacrum, and sacroiliac ligaments. The psoas major originates from the T12 to L5 vertebrae's lateral margins and intervertebral discs and the L1 to L5 vertebrae's transverse processes. The psoas minor arises from the T12 to L1 vertebrae's lateral borders and intervertebral discs. The iliacus and psoas major share an insertion point in the lesser trochanter area. The psoas minor muscle ends proximal to this territory at the femur's pectineal line. These muscles act as a group to flex and stabilize the hip. The L1 to L3 ventral rami and femoral nerve supply the iliopsoas muscles.
- The sartorius, also called "tailor's muscle," is an elongated, slender muscle extending inferomedially from the anterior superior iliac spine and inserting on the superomedial tibia. This muscle contributes to hip flexion, abduction, lateral rotation, and knee flexion. The sartorius acts on both the hip and knee joints. The muscle moves in various directions but is weak due to its small cross-sectional area and great length. The femoral nerve innervates the sartorius.
- The quadriceps femoris is the 4-headed anterior femoral muscle group (see Image. Right Quadriceps Femoris, Anterior View). The quadriceps femoris is a powerful knee extensor. The component muscles arise from different regions in the proximal lower limb but insert on the patellar base through a common tendinous structure, the quadriceps tendon. The patellar ligament connects the quadriceps tendon to the tibial tuberosity on the proximal anterior tibia. The quadriceps femoris consists of the following muscles, all supplied by the femoral nerve:
- The rectus femoris is a bipennate muscle originating from the anterior inferior iliac spine and a region superior to the acetabulum. This muscle is a powerful knee flexor and is the only quadriceps component to cross, flex, and stabilize the hip joint.
- The vastus lateralis arises from the femur's greater trochanter and linea aspera.
- The vastus intermedius originates from the anterior and lateral femoral shaft borders and lies between the 2 other vastus muscles and deep to the rectus femoris.
- The vastus medialis is the most medially situated vastus muscle, originating from the linea aspera and intertrochanteric line of the femur.
- The articularis genu is a muscle that may arise from the vastus intermedius in some individuals and act like the quadriceps femoris' 5th head. This muscle is sometimes called the "tensor of the vastus intermedius" or "articular muscle of the knee."
Medial Thigh Muscles
The medial femoral compartment muscles are thigh adductors contributing to hip flexion and internal rotation. The obturator nerve (L2-L4) and its branches innervate this compartment.[21]
- The gracilis is an elongated muscle that extends inferiorly from the pubis' inferior aspect to the superomedial tibia. This muscle adducts the thigh and contributes to knee flexion and medial rotation.
- The adductor brevis arises from the inferior pubis, descending inferolaterally and inserting on the linea aspera and femur's pectineal line. The adductor brevis weakly flexes the knee and contributes to hip adduction.
- The adductor longus originates from the pubis and then descends inferolaterally before inserting on the linea aspera.
- The adductor magnus consists of "adductor" and "hamstring" portions. The adductor part arises from the inferior margin of the ischiopubic ramus and inserts on the posterior femur. The obturator nerve's posterior division innervates this muscle segment. The adductor part of the adductor magnus adducts the thigh and contributes to hip flexion. Meanwhile, the hamstring part of the muscle arises from the ischial tuberosity and descends inferiorly, inserting on the adductor tubercle on the posteromedial femur. The sciatic nerve's tibial division innervates this muscle segment and contributes to hip extension.
- The obturator externus originates from the obturator foramen's rim and obturator membrane and inserts on the femoral trochanteric fossa. This muscle laterally rotates and stabilizes the hip.
The adductor hiatus is a gap in the adductor magnus tendon proximal to the medial supracondylar ridge. Femoral neurovascular structures traverse the adductor hiatus before reaching the popliteal area.
Posterior Thigh Muscles
The posterior thigh muscles are part of the hamstring muscle group (see Image. Muscles of the Hip and Thigh). These muscles primarily extend the hip and flex the knee. The posterior femoral muscles are also involved in hip abduction, internal rotation, and external rotation.[22] Sciatic nerve branches innervate these muscles.
- The semitendinosus arises from the ischial tuberosity alongside the semimembranosus and distally attaches to the superomedial tibial surface.
- The semimembranosus originates from the ischial tuberosity with the semitendinosus and inserts on the posteromedial tibial condyle. This muscle also contributes to the oblique popliteal ligament.
- The biceps femoris consists of long and short heads. The long head arises from the ischial tuberosity with the other hamstrings, while the short head arises from the linea aspera and posteroinferior femur. The sciatic nerve's tibial division innervates the long head. Meanwhile, the common fibular nerve supplies the short head. Both biceps femoris heads insert on the fibular head, with the fibular collateral ligament splitting the muscle's tendon at this site.
The tibial division of the sciatic nerve innervates the semitendinosus and semimembranosus. These muscles extend the hip, flex the knee, and medially rotate the flexed knee.
Physiologic Variants
Femoral region anatomical variants are numerous and may involve femoral angulation, arterial origins, and the femoral canal's vascular routes. For example, the inclination of the angle formed by the femoral head, neck, and shaft exhibits sexual dimorphism. In male individuals, this angle is approximately 115° to 140°. In female persons, this angle is more acute. However, both sexes display considerable variation and overlap.[23]
Clinically, a decreased femoral inclination angle is known as coxa vara, while the opposite is known as coxa valga.[24] Developmental defects or pathological processes that weaken the femoral neck, such as osteomalacia, may impact the femoral angle of inclination.
Cadaveric studies reveal that the distance between the inguinal ligament and the origin of the profunda femoris and circumflex branches vary individually.[25] The profunda femoris' origin from the femoral artery may also change. The deep thigh artery arises posterolaterally in most people, but others may have this blood vessel emerging posteriorly or posteromedially from the femoral artery.[26]
Femoral artery and vein transposition in the femoral canal is uncommon but has been reported in ultrasound-guided case studies. This variant may cause confusion and complications when performing central femoral venous catheterization, especially without ultrasound guidance.[27]
Surgical Considerations
Femoral fracture reduction and fixation are common procedures involving the femoral region. A thorough understanding of the impact of fracture types on proximal femoral neurovascular anatomy can help prevent complications from these procedures (see Image. Inguinal Region).[28] Some cases are explained below.
Femoral Neck Fractures
Femoral neck fractures may result in avascular necrosis if the foveal artery within the femoral neck and ligamentum teres is cut. This injury can also result in a hip capsular hematoma that, if adequately contained, may cause less damage to surrounding structures. Repairing these fractures is performed via hemiarthroplasty, with a posterior approach to minimize blood loss and allow prosthesis articulation with the native acetabulum.[29]
Rarely, the arterial supply in this region may remain intact in nondisplaced or impacted femoral neck fractures. A posterior approach is also useful, usually performed with internal fixation via intramedullary nails.[30]
Intertrochanteric Hip Fractures
Hemorrhage is a risk with intertrochanteric hip fractures due to the proximity of the lateral circumflex arteries. Severe fractures may also involve the profunda femoris. A lateral surgical approach via a sliding hip screw may be taken during reduction and internal fixation. Besides the arteries involved, other structures in this area that must be considered during surgical planning are the lateral cutaneous nerve of the thigh and the sciatic nerve.[31]
Subtrochanteric and Femoral Midshaft Fractures
Subtrochanteric and femoral midshaft injuries may also lead to hemorrhage when the profunda femoris is involved. Compartment syndrome may arise from significant bleeding within the muscle compartments.[32] Repairing these fractures may involve anterograde or retrograde intramedullary nailing or open reduction with internal fixation by plate implantation.[33]
Clinical Significance
The femoral triangle and adductor canal are anatomical landmarks crucial for procedures such as perioperative pain management and femoral venous catheterization. Neurovascular structures supplying the thigh pass through these regions.[27]
The femoral triangle is a triangular region in the proximomedial thigh bordered superiorly by the inguinal ligament, medially by the adductor longus, and laterally by the sartorius (see Image. Femoral Triangle Structures). The structures within the femoral triangle from lateral to medial are the femoral nerve, artery, vein, and lymphatics, hence the mnemonic aid "NAVeL" for these structures. The femoral sheath encloses the femoral artery, vein, and lymphatics. The femoral nerve lies lateral to the femoral sheath.[34] The femoral artery and vein and the saphenous nerve pass deep to the sartorius before entering the adductor canal. The femoral triangle enables femoral pulse palpation, vascular access, and hernia assessment.
The adductor canal, also known as the Hunter or subsartorial canal, permits the passage of neurovascular structures from the anteromedial thigh to the posterior leg (see Image. Adductor Canal). The canal is bordered superficially and medially by the sartorius and vastoadductor membrane, posterolaterally by the adductor longus and magnus, and laterally by the vastus medialis. The adductor canal houses the saphenous nerve (superficial), femoral vein (medial), and femoral artery (lateral).[35]
Perioperative lower limb pain management may be achieved by a nerve block in the femoral triangle or both the femoral and adductor canals. Ultrasound-guided needle placement can help safely administer anesthetics to target the femoral and saphenous nerves in these territories. Lidocaine and bupivacaine are frequently used in these procedures. However, the choice of anesthetic may depend on clinical indications, the provider's judgment, and new drug developments.[36]
The femoral vein's location allows easy access during central venous line placement. Though less important than the internal jugular vein for central venous catheterization, the femoral vein has been proven to be an effective alternative route for such procedures.[37]
Media
(Click Image to Enlarge)
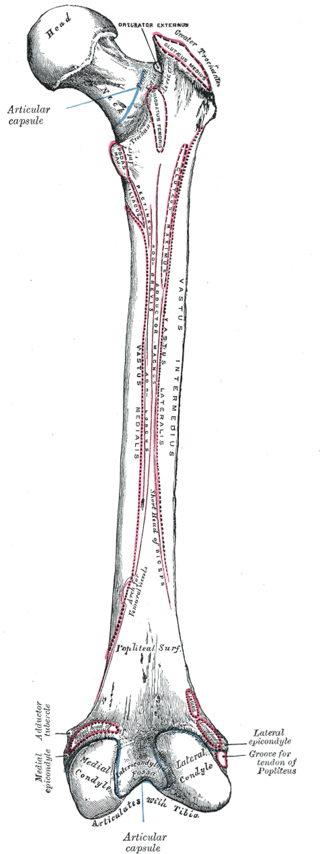
Right Femur Anatomy, Posterior Surface. Bony structures in this illustration include the greater trochanter, popliteal femoral surface, medial condyle, lateral condyle, tibia, lateral epicondyle, adductor tubercle, and medial epicondyle. Muscle attachment points shown are for the gluteus medius, iliacus, psoas major, vastus intermedius, vastus medialis, adductor magnus and brevis, and popliteus.
Gray's Anatomy
(Click Image to Enlarge)
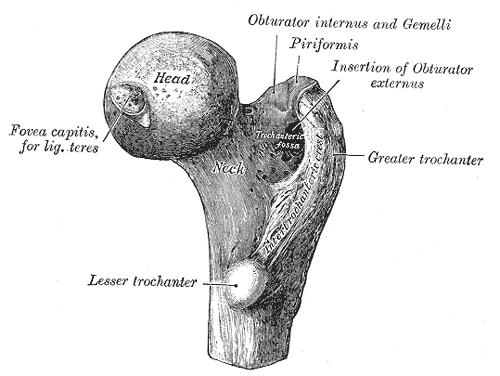
Right Proximal Femur Anatomy. This illustration shows the femoral head, fovea capitis, ligamentum teres, femoral neck, trochanteric fossa, trochanter, lesser trochanter, greater trochanter, intertrochanteric crest, and insertions for the obturator internus, gemelli, piriformis, obturator externus.
Gray's Anatomy
(Click Image to Enlarge)

Inguinal Region. This image includes the inferior epigastric artery and vein, rectus abdominis muscle, internal inguinal ring, Hesselbach triangle, inguinal ligament, inguinal canal, external inguinal ring, femoral ring, femoral vein, femoral artery, and spermatic cord.
Contributed by Beckie Palmer
(Click Image to Enlarge)

Muscles of the Hip and Thigh. The gluteal muscles include the gluteus maximus, gluteus medius, and gluteus minimus. Hip muscles include the piriformis, gemellus superior, gemellus inferior, and obturator internus. Thigh muscles include the adductor magnus, vastus lateralis, biceps femoris, semitendinosus, hamstring tendons, and gracilis.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
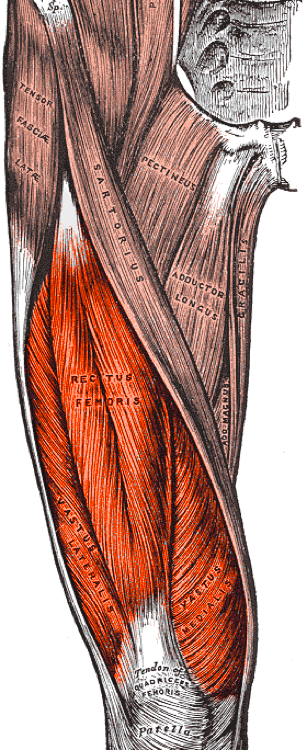
Right Quadriceps Femoris, Anterior View. This illustration shows the rectus femoris, vastus lateralis, and vastus medialis. Other structures are the tensor fascia lata, sartorius, pectineus, adductor longus, gracilis, adductor magnus, quadriceps femoris tendon, and patella.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
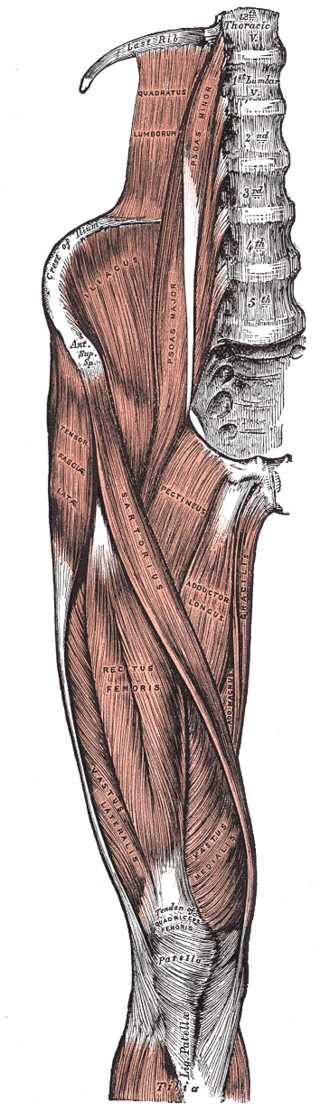
Right Hip and Femoral Muscles, Anterior View. This illustration shows the tensor fasciae latae, thoracic vertebrae, quadratus lumborum, psoas minor and major, crest of ilium, anterior superior iliac spine, iliacus, sartorius, pectineus, adductor longus, gracilis, adductor magnus, rectus femoris, vastus lateralis and medialis, tibia, patella, and quadriceps tendon.
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
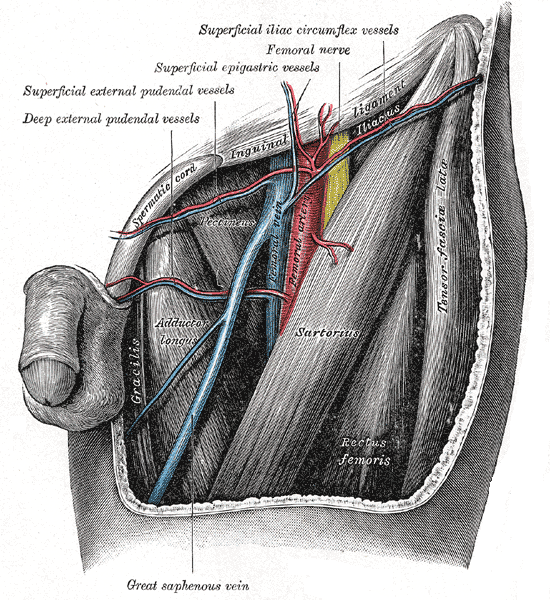
Femoral Triangle Structures. This anterior view shows the femoral artery, vein and nerve, and the deep external pudendal vessels, superficial external pudendal vessels, superficial epigastric vessels, and superficial iliac circumflex nerve.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
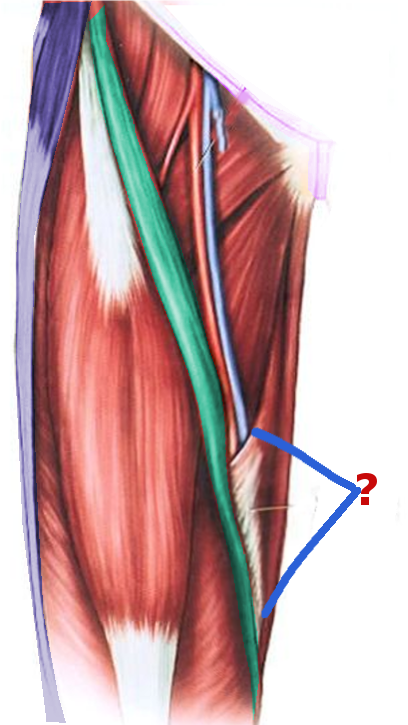
Adductor Canal. This anterior view shows the superficial femoral artery (red) and femoral vein passing through the adductor or Hunter canal (marked by "?"). The borders of this region include the femoral triangle's apex (proximal), adductor hiatus (distal), vastus medialis (anterolateral), adductor longus and magnus (posterolateral), and vastoadductor membrane (medial).
Image courtesy S Bhimji MD
(Click Image to Enlarge)
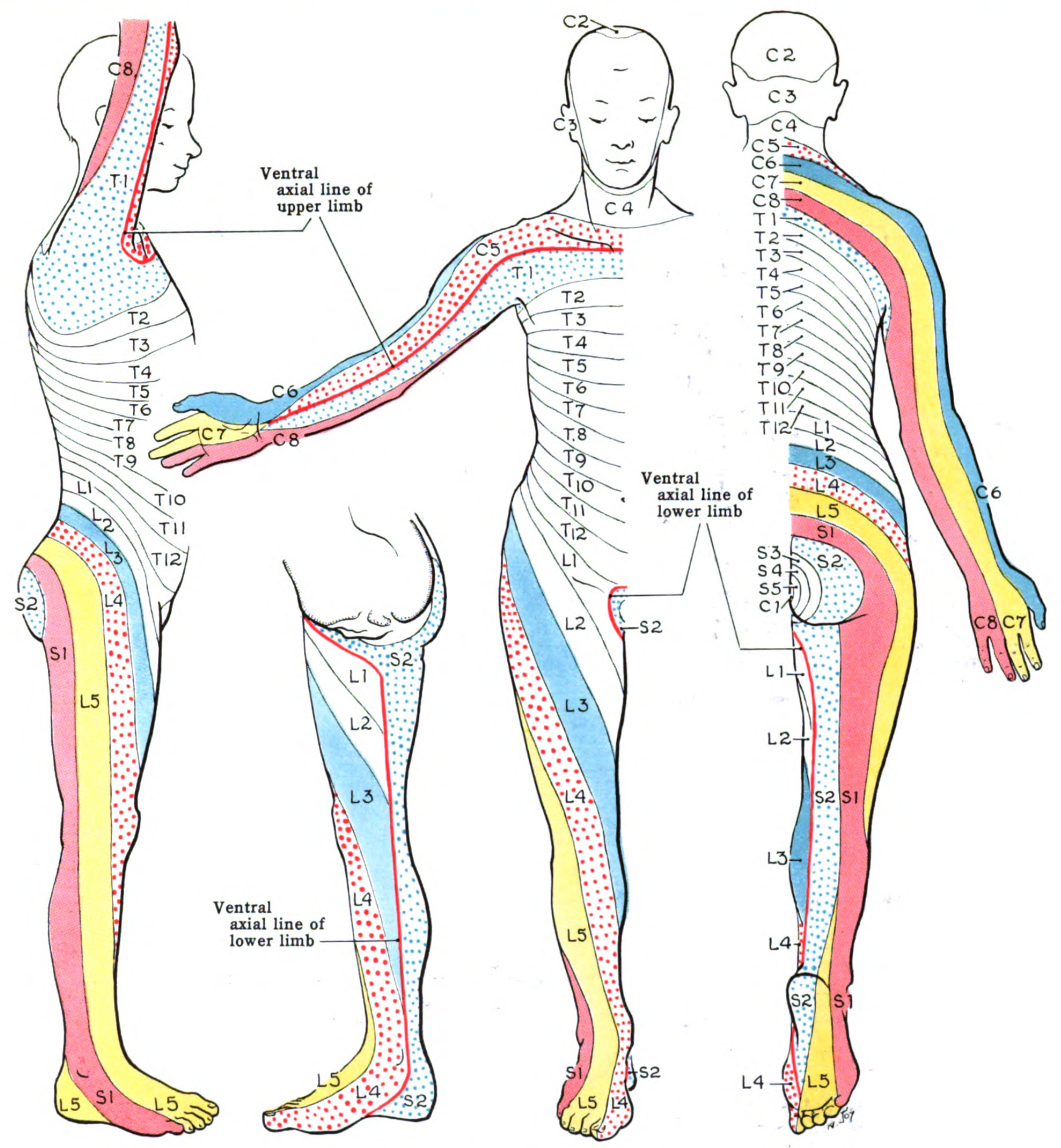
Dermatome Map. A dermatome is an area of skin receiving sensory innervation from a single spinal nerve dorsal root. Shown here is a map of the body's dermatomes.
Contributed from Wikimedia. Grant, John Charles Boileau (Public Domain) An atlas of anatomy, by regions 1962
References
Runge C, Jensen JM, Clemmesen L, Knudsen HB, Holm C, Børglum J, Bendtsen TF. Analgesia of Combined Femoral Triangle and Obturator Nerve Blockade Is Superior to Local Infiltration Analgesia After Total Knee Arthroplasty With High-Dose Intravenous Dexamethasone. Regional anesthesia and pain medicine. 2018 May:43(4):352-356. doi: 10.1097/AAP.0000000000000731. Epub [PubMed PMID: 29346228]
Ishiguro S, Yokochi A, Yoshioka K, Asano N, Deguchi A, Iwasaki Y, Sudo A, Maruyama K. Technical communication: anatomy and clinical implications of ultrasound-guided selective femoral nerve block. Anesthesia and analgesia. 2012 Dec:115(6):1467-70. doi: 10.1213/ANE.0b013e31826af956. Epub 2012 Aug 10 [PubMed PMID: 22886842]
Watanabe T, Ogihara H, Soeta T, Fujiwara T, Yoshida H. Comparison of range of motion during movement from supine to sitting position in healthy young and elderly participants. Journal of physical therapy science. 2019 Jan:31(1):102-107. doi: 10.1589/jpts.31.102. Epub 2019 Jan 29 [PubMed PMID: 30774215]
Gold M, Munjal A, Varacallo M. Anatomy, Bony Pelvis and Lower Limb, Hip Joint. StatPearls. 2024 Jan:(): [PubMed PMID: 29262200]
Cowan PT, Kahai P. Anatomy, Bones. StatPearls. 2024 Jan:(): [PubMed PMID: 30725884]
Gupton M, Imonugo O, Black AC, Launico MV, Terreberry RR. Anatomy, Bony Pelvis and Lower Limb, Knee. StatPearls. 2024 Jan:(): [PubMed PMID: 29763193]
Sheeba CJ, Andrade RP, Palmeirim I. Getting a handle on embryo limb development: Molecular interactions driving limb outgrowth and patterning. Seminars in cell & developmental biology. 2016 Jan:49():92-101. doi: 10.1016/j.semcdb.2015.01.007. Epub 2015 Jan 21 [PubMed PMID: 25617599]
Stainton H, Towers M. Polarizing Region Tissue Grafting in the Chick Embryo Limb Bud. Methods in molecular biology (Clifton, N.J.). 2018:1863():143-153. doi: 10.1007/978-1-4939-8772-6_8. Epub [PubMed PMID: 30324596]
Mróz I, Kielczewski S, Pawlicki D, Kurzydło W, Bachul P, Konarska M, Bereza T, Walocha K, Kaythampillai LN, Depukat P, Pasternak A, Bonczar T, Chmielewski P, Mizia E, Skrzat J, Mazur M, Warchoł Ł, Tomaszewski K. Blood vessels of the shin - anterior tibial artery - anatomy and embryology - own studies and review of the literature. Folia medica Cracoviensia. 2016:56(1):33-47 [PubMed PMID: 27513837]
Rivera RE, Hootnick DR, Gingold AR, Levinsohn EM, Kruger LM, Packard DS Jr. Anatomy of a duplicated human foot from a limb with fibular dimelia. Teratology. 1999 Nov:60(5):272-82 [PubMed PMID: 10525205]
Level 3 (low-level) evidenceDennis SC, Berkland CJ, Bonewald LF, Detamore MS. Endochondral ossification for enhancing bone regeneration: converging native extracellular matrix biomaterials and developmental engineering in vivo. Tissue engineering. Part B, Reviews. 2015 Jun:21(3):247-66. doi: 10.1089/ten.TEB.2014.0419. Epub 2014 Dec 4 [PubMed PMID: 25336144]
Level 3 (low-level) evidenceSun Q, Fan G, Li X, Gong J, Ge W, Cai M. Relationship Between Femur and Femoral Arteries for Identifying Risk Factors for Vascular Injury. Medical science monitor : international medical journal of experimental and clinical research. 2017 Apr 10:23():1733-1740 [PubMed PMID: 28392552]
Mednick RE, Alvi HM, Morgan CE, Stover MD, Manning DW. Femoral vein blood flow during a total hip arthroplasty using a modified Heuter approach. The Journal of arthroplasty. 2015 May:30(5):786-9. doi: 10.1016/j.arth.2014.12.015. Epub 2014 Dec 17 [PubMed PMID: 25660612]
Portugal IB, Ribeiro Ide L, Sousa-Rodrigues CF, Monte-Bispo RF, Rocha AC. Distribution of saphenous vein valves and its practical importance. Revista brasileira de cirurgia cardiovascular : orgao oficial da Sociedade Brasileira de Cirurgia Cardiovascular. 2014 Oct-Dec:29(4):564-8. doi: 10.5935/1678-9741.20140038. Epub [PubMed PMID: 25714210]
Level 2 (mid-level) evidenceRao AS, Rajmanickam K, Narayanan GS. Study of distribution of inguinal nodes around the femoral vessels and contouring of inguinal nodes. Journal of cancer research and therapeutics. 2015 Jul-Sep:11(3):575-9. doi: 10.4103/0973-1482.163735. Epub [PubMed PMID: 26458584]
Fracol ME, Janes LE, Ko JH, Dumanian GA. Targeted Muscle Reinnervation in the Lower Leg: An Anatomical Study. Plastic and reconstructive surgery. 2018 Oct:142(4):541e-550e. doi: 10.1097/PRS.0000000000004773. Epub [PubMed PMID: 30020229]
Swezey E, Bordoni B. Anatomy, Bony Pelvis and Lower Limb: Lateral Femoral Cutaneous Nerve. StatPearls. 2024 Jan:(): [PubMed PMID: 30335334]
Kendir S, Torun Bİ, Akkaya T, Comert A, Tuccar E, Tekdemir I. Re-defining the anatomical structures for blocking the nerves in adductor canal and sciatic nerve through the same injection site: an anatomical study. Surgical and radiologic anatomy : SRA. 2018 Nov:40(11):1267-1274. doi: 10.1007/s00276-018-2094-1. Epub 2018 Aug 23 [PubMed PMID: 30167824]
Üçeyler N, Vollert J, Broll B, Riediger N, Langjahr M, Saffer N, Schubert AL, Siedler G, Sommer C. Sensory profiles and skin innervation of patients with painful and painless neuropathies. Pain. 2018 Sep:159(9):1867-1876. doi: 10.1097/j.pain.0000000000001287. Epub [PubMed PMID: 29863528]
Migirov A, Arbor TC, Vilella RC. Anatomy, Abdomen and Pelvis: Adductor Canal (Subsartorial Canal, Hunter Canal). StatPearls. 2024 Jan:(): [PubMed PMID: 32310506]
Launico MV, Sinkler MA, Nallamothu SV. Anatomy, Bony Pelvis and Lower Limb: Femoral Muscles. StatPearls. 2024 Jan:(): [PubMed PMID: 29763184]
Yamauchi K, Kato C, Kato T. Characteristics of individual thigh muscles including cross-sectional area and adipose tissue content measured by magnetic resonance imaging in knee osteoarthritis: a cross-sectional study. Rheumatology international. 2019 Apr:39(4):679-687. doi: 10.1007/s00296-019-04247-2. Epub 2019 Jan 28 [PubMed PMID: 30689015]
Level 2 (mid-level) evidenceChang A, Breeland G, Black AC, Hubbard JB. Anatomy, Bony Pelvis and Lower Limb: Femur. StatPearls. 2024 Jan:(): [PubMed PMID: 30422577]
Hartel MJ, Petersik A, Schmidt A, Kendoff D, Nüchtern J, Rueger JM, Lehmann W, Grossterlinden LG. Determination of Femoral Neck Angle and Torsion Angle Utilizing a Novel Three-Dimensional Modeling and Analytical Technology Based on CT Datasets. PloS one. 2016:11(3):e0149480. doi: 10.1371/journal.pone.0149480. Epub 2016 Mar 2 [PubMed PMID: 26933877]
Seto AH, Tyler J, Suh WM, Harrison AT, Vera JA, Zacharias SJ, Daly TS, Sparling JM, Patel PM, Kern MJ, Abu-Fadel M. Defining the common femoral artery: Insights from the femoral arterial access with ultrasound trial. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions. 2017 Jun 1:89(7):1185-1192. doi: 10.1002/ccd.26727. Epub 2016 Aug 27 [PubMed PMID: 27566991]
Nasr AY, Badawoud MH, Al-Hayani AA, Hussein AM. Origin of profunda femoris artery and its circumflex femoral branches: anatomical variations and clinical significance. Folia morphologica. 2014 Feb:73(1):58-67. doi: 10.5603/FM.2014.0008. Epub [PubMed PMID: 24590524]
Yu SK, Chung TT, Yeh CC, Cherng CH, Lin SL. A patient with femoral triangle anatomy transposition challenges NAVY rule. Journal of clinical anesthesia. 2018 Feb:44():80-81. doi: 10.1016/j.jclinane.2017.11.014. Epub [PubMed PMID: 29161543]
Radowsky JS, Rodriguez CJ, Wind GG, Elster EA. A Surgeon's Guide to Obtaining Hemorrhage Control in Combat-Related Dismounted Lower Extremity Blast Injuries. Military medicine. 2016 Oct:181(10):1300-1304 [PubMed PMID: 27753567]
Waewsawangwong W, Ruchiwit P, Huddleston JI, Goodman SB. Hip arthroplasty for treatment of advanced osteonecrosis: comprehensive review of implant options, outcomes and complications. Orthopedic research and reviews. 2016:8():13-29. doi: 10.2147/ORR.S35547. Epub 2016 Jun 28 [PubMed PMID: 30774467]
Liu C, Von Keudell A, McTague M, Rodriguez EK, Weaver MJ. Ideal length of thread forms for screws used in screw fixation of nondisplaced femoral neck fractures. Injury. 2019 Mar:50(3):727-732. doi: 10.1016/j.injury.2019.01.036. Epub 2019 Jan 31 [PubMed PMID: 30772052]
Gao YS, Guo YJ, Yu XG, Chen Y, Chen C, Lu NJ. A novel cerclage wiring technique in intertrochanteric femoral fractures treated by intramedullary nails in young adults. BMC musculoskeletal disorders. 2018 Oct 6:19(1):359. doi: 10.1186/s12891-018-2284-3. Epub 2018 Oct 6 [PubMed PMID: 30292231]
Streubel PN, Gardner MJ, Ricci WM. Management of femur shaft fractures in obese patients. The Orthopedic clinics of North America. 2011 Jan:42(1):21-35, v. doi: 10.1016/j.ocl.2010.07.004. Epub 2010 Oct 8 [PubMed PMID: 21095432]
Christ AB, Chawla H, Gausden EB, Villa JC, Wellman DS, Lorich DG, Helfet DL. Radiographic and Clinical Outcomes of Periprosthetic Distal Femur Fractures Treated With Open Reduction Internal Fixation. Journal of orthopaedic trauma. 2018 Oct:32(10):515-520. doi: 10.1097/BOT.0000000000001265. Epub [PubMed PMID: 30247279]
Level 2 (mid-level) evidenceMahabadi N, Lew V, Kang M. Anatomy, Abdomen and Pelvis: Femoral Sheath. StatPearls. 2024 Jan:(): [PubMed PMID: 29494010]
Wong WY, Bjørn S, Strid JM, Børglum J, Bendtsen TF. Defining the Location of the Adductor Canal Using Ultrasound. Regional anesthesia and pain medicine. 2017 Mar/Apr:42(2):241-245. doi: 10.1097/AAP.0000000000000539. Epub [PubMed PMID: 28002228]
Aso K, Izumi M, Sugimura N, Okanoue Y, Kamimoto Y, Yokoyama M, Ikeuchi M. Additional benefit of local infiltration of analgesia to femoral nerve block in total knee arthroplasty: double-blind randomized control study. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2019 Jul:27(7):2368-2374. doi: 10.1007/s00167-018-5322-7. Epub 2018 Dec 8 [PubMed PMID: 30536047]
Level 1 (high-level) evidenceSaugel B, Scheeren TWL, Teboul JL. Ultrasound-guided central venous catheter placement: a structured review and recommendations for clinical practice. Critical care (London, England). 2017 Aug 28:21(1):225. doi: 10.1186/s13054-017-1814-y. Epub 2017 Aug 28 [PubMed PMID: 28844205]