 Anatomy, Bony Pelvis and Lower Limb: Calf Flexor Hallucis Longus Muscle
Anatomy, Bony Pelvis and Lower Limb: Calf Flexor Hallucis Longus Muscle
Introduction
The flexor hallucis longus (FHL) muscle is one of the four muscles that compose the deep posterior compartment of the lower limb. The other three deep muscles are the flexor digitorum longus (FDL), tibialis posterior, and popliteus muscles. The flexor hallucis longus originates at the posterior surface of the fibula and inserting at the plantar aspect at the base of the distal phalanx of the great toe. The primary function of the flexor hallucis longus is flexion of the great toe, also serving to plantarflex and invert the foot. The antagonistic muscle is the extensor hallucis longus (EHL).[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The flexor hallucis longus is located towards the fibular aspect of the lower limb. The fibers of the flexor hallucis longus run obliquely inferiorly and posteriorly, passing through the tarsal tunnel on the medial aspect of the foot. The distal end of the flexor hallucis longus muscle is composed primarily of the tendon. This tendon runs inferiorly to the sustentaculum tali of the calcaneus, where it is stabilized by the annular ligament, traversing through the sole of the foot in-between the two heads of the flexor hallucis brevis muscle, continuing to the base of the great toe’s distal phalanx. The tendon passes through the grooves of the talus and the calcaneus, where it is connected to the flexor digitorum longus by a fibrous slip.[1][2]
Much like the other deep posterior compartment muscles of the leg, the flexor hallucis longus muscle assists with plantar flexion and inversion of the foot. The unique function of the flexor hallucis longus is the ability to flex the great toe through plantar flexion of the talocrural joint and the metatarsophalangeal and interphalangeal joints of the great toe while also aiding in supinating the ankle.[2]
Blood Supply and Lymphatics
The arterial supply to the flexor hallucis longus muscle is the muscular branch of the peroneal portion of the posterior tibial artery.[3] The venous system that drains this muscle is the peroneal vein, which is a branch of the popliteal vein. The lymphatic drainage of the flexor hallucis longus is the popliteal lymph nodes; the popliteal lymph nodes drain into the deep and superficial inguinal nodes.[1]
Nerves
The tibial nerve, composed of spinal roots L4, L5, S1, S2, and S3, innervates the flexor hallucis longus; it receives most of its nerve supply from the S1 and S2 but also receives innervation from L5 as well via the muscular branch of the tibial nerve.[1]
Physiologic Variants
A slip runs from the flexor digitorum longus to the flexor hallucis longus in most individuals, but an additional slip can also be viewed as an anatomical variant. This extremely rare extra muscle slip is known as the peroneocalcaneus internus. It originates inferiorly or laterally from the flexor hallucis longus muscle at the back of the fibula and passes over the sustentaculum tali alongside the flexor hallucis tendon, inserting into the calcaneus.[4][5]
In patients with an anatomically variable flexor hallucis longus, research has found that the mean distance to the neurovascular tibial bundle increased, as the normal anatomy was 0.9 mm apart, while the anatomically varying individuals were 1.3 mm apart. This increased distance helps to improve safety in hindfoot endoscopic procedures.[4] The anatomical variance between the flexor digitorum longus and flexor hallucis longus muscles in the plantar foot is vital for facilitating tendon harvesting, thereby reducing morbidity, and can help explain the possible postoperative functional loss. The slip between the two might also contribute to why the flexion of the lesser toes remains after transferring the flexor digitorum longus muscle.[5]
Surgical Considerations
In terms of surgical significance, the flexor hallucis longus has a role in Achilles (calcaneal) tendon rupture. A torn Achilles tendon usually presents as a patient reporting a "popping" feeling during strenuous exercise. Achilles tendon ruptures are especially common in patients with intermittent physical activity and are the most common tendon rupture in the lower extremity.[6] Symptoms are weakness and difficulty walking, and pain in the heel. In some chronic cases, physical exam findings include increased resting ankle dorsiflexion while prone and bent at the knee and calf atrophy. There usually is a palpable gap on the heel, and the patient will demonstrate a decreased range of motion in ankle plantar flexion and increased passive dorsiflexion. A Thompson test is used to help make a diagnosis and presents with a lack of plantar flexion when the examiner squeezes the calf.[7]
With the flexor hallucis longus tendon having proximity to the Achilles tendon, the flexor hallucis longus is the most commonly used tendon for tendon transfer when the Achilles tendon is irreparable. The Achilles tendon usually is irreparable with a chronic retracted tear. The combination of its line of pull and proximity makes it the ideal candidate for Achilles tendon replacement. The surgical procedure for the flexor hallucis longus tendon replacing the Achilles tendon is called transfer for Achilles reconstruction.[8][9]
Clinical Significance
A common issue seen with flexor hallucis longus dysfunction is stenosing tenosynovitis, which commonly occurs in ballet dancers who undergo extreme plantarflexion while performing various ballet movements. First-line treatment is rest and physical therapy, but a surgical approach is used if the injury is debilitating enough, followed by a well-crafted rehabilitation program. Anti-inflammatory medications can also be prescribed to alleviate symptoms.[10] Diagnosis of stenosing tenosynovitis has proven challenging as many symptoms overlap with flexor hallucis tendinitis, plantar fasciitis, and tarsal tunnel syndrome.[11]
Hallux saltans is another condition that arises from flexor hallucis longus muscle overuse. A nodule develops along the tendon that can cause a “popping effect” during contraction due to friction with surrounding tissues. If the nodule continues to grow, this can cause stenosis of the flexor hallucis longus tendon leading to the stifling of the range of motion in the big toe, leading to relative immobility.[12] When contracted, the appearance of the great toe takes on that of a rigidly flexed interphalangeal joint, a clinical finding known as a checkrein deformity.[13]
Many clinical issues with the flexor hallucis longus muscle and tendon get overlooked because of the muscle being small in size. Diagnosis is via MRI to evaluate the pathology and condition of the flexor hallucis longus tendon. Diagnostic ultrasound is used to assess muscle movement and identify potential impingement sites.[11][12]
The flexor hallucis longus tendon also has utility for tendon transfer in chronic calcaneal (Achilles) tendon rupture. Single-incision flexor hallucis longus transfers for calcaneal tendon ruptures are considered a simple method with miniscule morbidity and complications.[8][9]
Media
(Click Image to Enlarge)
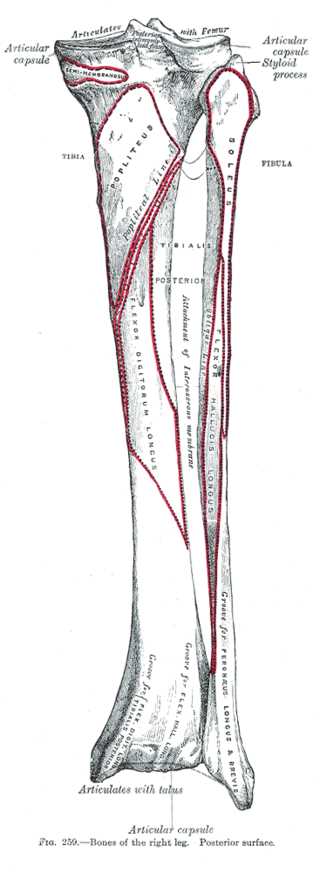
Posterior View of Right Leg Bone Anatomy. Anatomy includes tibia, fibula, femur, semimembranosus, styloid process, soleus, popliteus, popliteal, tibialis, flexor digitorum longus, flexor hallucis longus, peroneus longus, brevis, and talus.
Gray's Anatomy
(Click Image to Enlarge)
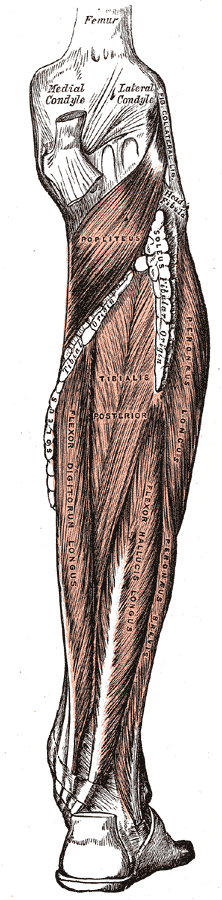
Posterior Muscles of the Leg, Popliteus, Tibialis Posterior, Peroneus Longus, Flexor Digitorum Longus, Flexor Hallucis Longus, Peroneus Brevis, Femur
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
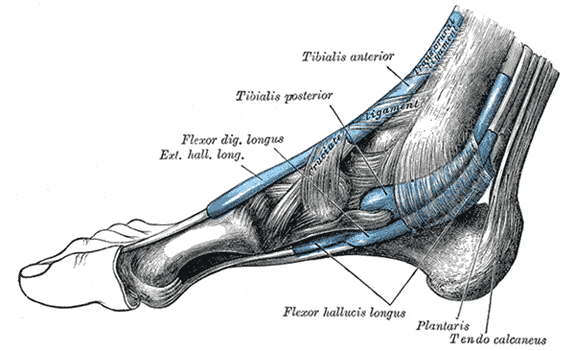
The mucous sheaths of the tendons around the ankle; Medial aspect, Exterior Hallucis Longus, Flexor digitorum longus, Tibialis posterior and Anterior, Flexor hallucis longus, Plantaris, Tendon calcaneus
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Edama M, Kubo M, Onishi H, Takabayashi T, Yokoyama E, Inai T, Watanabe H, Nashimoto S, Kageyama I. Anatomical study of toe flexion by flexor hallucis longus. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2016 Mar:204():80-5. doi: 10.1016/j.aanat.2015.11.008. Epub 2015 Dec 15 [PubMed PMID: 26704354]
Mostafa E, Graefe SB, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Leg Posterior Compartment. StatPearls. 2023 Jan:(): [PubMed PMID: 30726025]
Sassu P, Acland RD, Salgado CJ, Mardini S, Ozyurekoglu T. Anatomy and vascularization of the flexor hallucis longus muscle and its implication in free fibula flap transfer: an anatomical study. Annals of plastic surgery. 2010 Feb:64(2):233-7. doi: 10.1097/SAP.0b013e3181a2c772. Epub [PubMed PMID: 20098112]
Vega J, Redó D, Savín G, Malagelada F, Dalmau-Pastor M. Anatomical variations of flexor hallucis longus tendon increase safety in hindfoot endoscopy. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2017 Jun:25(6):1929-1935. doi: 10.1007/s00167-017-4465-2. Epub 2017 Feb 20 [PubMed PMID: 28220191]
Plaass C, Abuharbid G, Waizy H, Ochs M, Stukenborg-Colsman C, Schmiedl A. Anatomical variations of the flexor hallucis longus and flexor digitorum longus in the chiasma plantare. Foot & ankle international. 2013 Nov:34(11):1580-7. doi: 10.1177/1071100713494780. Epub 2013 Jun 20 [PubMed PMID: 23788233]
Lemme NJ, Li NY, DeFroda SF, Kleiner J, Owens BD. Epidemiology of Achilles Tendon Ruptures in the United States: Athletic and Nonathletic Injuries From 2012 to 2016. Orthopaedic journal of sports medicine. 2018 Nov:6(11):2325967118808238. doi: 10.1177/2325967118808238. Epub 2018 Nov 26 [PubMed PMID: 30505872]
Thermann H. [Achilles tendon rupture-Part 1: etiology and diagnostics]. Der Chirurg; Zeitschrift fur alle Gebiete der operativen Medizen. 2019 Oct:90(10):863-872. doi: 10.1007/s00104-019-01024-6. Epub [PubMed PMID: 31531684]
Abubeih H, Khaled M, Saleh WR, Said GZ. Flexor hallucis longus transfer clinical outcome through a single incision for chronic Achilles tendon rupture. International orthopaedics. 2018 Nov:42(11):2699-2704. doi: 10.1007/s00264-018-3976-x. Epub 2018 May 12 [PubMed PMID: 29754186]
Level 2 (mid-level) evidenceLee J, Williams C, Lowrey C, Gould G, Markert R, Laughlin R. Flexor Hallucis Longus Tendon Transfer Fixation. Foot & ankle specialist. 2017 Feb:10(1):31-36. doi: 10.1177/1938640016666917. Epub 2016 Sep 20 [PubMed PMID: 27604514]
Vosseller JT, Dennis ER, Bronner S. Ankle Injuries in Dancers. The Journal of the American Academy of Orthopaedic Surgeons. 2019 Aug 15:27(16):582-589. doi: 10.5435/JAAOS-D-18-00596. Epub [PubMed PMID: 30789380]
Anderson MR, Bell DE, Ketz JP. Flexor Hallucis Longus Muscle and Tendon Transfer for the Treatment of Achilles Tendon Wounds. Foot & ankle international. 2018 Feb:39(2):205-209. doi: 10.1177/1071100717739395. Epub 2017 Nov 24 [PubMed PMID: 29171303]
Martinez-Salazar EL, Vicentini JRT, Johnson AH, Torriani M. Hallux saltans due to stenosing tenosynovitis of flexor hallucis longus: dynamic sonography and arthroscopic findings. Skeletal radiology. 2018 May:47(5):747-750. doi: 10.1007/s00256-017-2853-9. Epub 2017 Dec 28 [PubMed PMID: 29285554]
Rodriguez-Collell JR, Mifsut-Miedes D. Checkrein Deformity of the Hallux and Second Toe after Soft-Tissue Injury. Case reports in orthopedics. 2021:2021():8459586. doi: 10.1155/2021/8459586. Epub 2021 Jan 26 [PubMed PMID: 33575050]
Level 3 (low-level) evidence