Introduction
Laser-assisted in situ keratomileusis (LASIK) is a common ophthalmologic surgical procedure used to correct refractive error. LASIK was patented in 1989 by Dr. Gholam Peyman.[1] The first publication of LASIK used in patient care was by Dr. Ioannis Pallikaris et al., in the early 1990s. This procedure quickly became popular due to decreased time of recovery and post-surgical complications, with no decrease in efficacy.[2] Since its implementation in clinical practice, LASIK is among the most scrutinized and studied surgical procedures to have gone through FDA inspection.[3] Thirty years later, with advancements in technique and equipment, LASIK continues to provide efficient, predictable, and safe outcomes with patients reporting satisfaction with the procedure as compared to using spectacles or contact lenses.[4][5][6]
A Historical Perspective
Understanding the impact of LASIK in refractive correction requires knowledge of its development. The first significant breakthrough in refractive therapy came in the 1930s, with radial keratotomy by Dr. Tsutomu Sato in Japan. By making incisions deep into Descemet’s membrane, the flattening of the cornea helped correct myopia. However, many complications, like corneal decompensation, came from these deep incisions. Alternative methods were developed, such as the hexagonal keratectomy by Dr. Antonio Méndez in Mexico.[7] At this time, it was still difficult to correct patients with astigmatism or the asymmetric shape of the cornea.
Keratomileusis is the medical term for corneal reshaping, which came about in the 1950s and ’60s with the work of Spanish ophthalmologist José Barraquer. His technique initially involved the microkeratome, a mechanical instrument that, with its oscillating sharp blade, cuts the top layer of the cornea away to create a lenticule and reveal underlying stroma. An additional cut through the stroma was made, and the lenticule was sutured back into place. This technique came to be known as anterior lamellar keratoplasty (ALK).[2] He also developed a procedure called keratophakia, which corrected hyperopia by freezing and shaping donor corneal stroma with a cryolathe and then placing it into the patient’s cornea.[2] His microkeratome, however, was rudimentary and led to imprecise treatments. The microkeratome was further improved in the 1980s through Barraquer’s student, Dr. Luis Ruiz. Variations on corneal excision and replacement by implantation also followed through the years, but it came with the risk of tissue rejection and corneal tearing.[2][7]
The excimer, or “excited dimer” laser and its medical use, was discovered in 1970 by Dr. Stephen Trokel and Dr. Rangaswamy Srinivasan in the early 1980s.[8] These works led the way to the development of photorefractive keratectomy (PRK). Dr. Marguerite McDonald was the first to perform this in the late 1980s.[9][10] This technique uses a noble gas combined with a halogen to create a laser to ablate the superficial layers of the cornea.[11] PRK allowed for more precise reshaping and further refractive correction.[7]
LASIK is essentially a combination of ALK and PRK, which was first utilized in the early 1990s.[2] Advances in lenticule flap creation were made to allow for a hinged cap instead of a free cap. With the innovation of the femtosecond laser, developed by Dr. Imola Ratkay-Traub, Dr. Tibor Juhasz, and Dr. Ron Kurtz in the early 1990s, a corneal flap could be created without a mechanical blade and then replaced without sutures.[7][12]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The refractive power of the eye is attributed, in part, to the cornea. It is responsible for about two-thirds of the eye’s power of refraction.[13] LASIK alters the cornea’s refractive power in myopic, hyperopic, and astigmatic patients.
The cornea is the one-half millimeter thick tissue comprising the anterior surface of the eye. It has five layers consisting of, from superficial to deep, a squamous epithelial layer, the anterior basement membrane (Bowman’s), a stroma filled with keratocytes and collagen, and the posterior basement membrane (Descemet’s) with a single layer endothelium separating it from the anterior chamber of the eye.[14]
LASIK surgery changes the refractive power of the cornea first by creating a hinged corneal flap from the epithelium, Bowman’s membrane, and the superficial part of the corneal stroma. The more posterior layers of the stroma are exposed for ablation treatment. Thus, for a myopic treatment, central corneal curvature is decreased with the ablation, and the total refractive power of the eye decreases to attain emmetropia, or normal vision (see figure 1). For a hyperopic treatment, the paracentral area is flattened, leading to a steeper central cornea and an increase in refractive power (see figure 1). After targeted laser therapy to the stroma, the flap is replaced, and reepithelialization occurs over the flap margin. Sutures are not necessary.
Indications
LASIK is an option in patients with low to high myopia, with or without astigmatism. It has been shown that LASIK can improve myopia from -2.00 to -20.00 D; however, it is generally indicated in patients with low to moderate myopia, from -0.5 D up to -9.00 D, as these patients have a higher probability of reaching emmetropia.[15][16] This procedure is also reported as safe and efficacious in patients with hyperopia and astigmatism.[17][18][19] While LASIK can treat hyperopia with more predictable outcomes up to +6.00 D, it is recommended to perform LASIK for hyperopic patients of up to +4.00 D and astigmatism up to 5.00 D.[19][20][21][22] The ophthalmic surgeon decides on choosing excimer laser ablation or other treatment options for the patient based on the type and severity of the refractive error, as well as other factors such as the patient’s age, corneal thickness, crystalline lens changes, keratometry, and corneal topography results, among others.
Currently, LASIK is the most common laser treatment for refractive error. In addition to its applications for a wide variety of refractive errors, patients suffer relatively little pain compared with techniques that do not create a flap, with recovery time to baseline being only a few days.[2][15][19] It is essential to clarify with the patient the realistic expectations of LASIK. These procedures are typically high in cost and are not usually covered by insurance because companies consider these procedures as cosmetic and not medically necessary. This high cost, roughly $1,500 to $2,500 per eye, can be attributed to the use of two lasers (excimer laser and femtosecond laser) in most practices.[2][23] In addition, the patient should be informed that LASIK does not correct presbyopia; thus, reading glasses may still be necessary. A myopic shift with cataract formation may also occur at a later age.[23]
Contraindications
Absolute Contraindications
Refractive Instability
Changes greater than 0.5 D in the last year constitute instability, and LASIK is not recommended for patients since it is a permanent procedure and operating on eyes that change rapidly may lead to severe complications such as postoperative ectasia.[24] According to the FDA guidelines for LASIK, conditions that may lead to refractive instability include pregnancy, nursing, and uncontrolled diabetes mellitus.
Corneal Ectasia
A normal corneal thickness is around 540-550 microns.[25] If the preoperative cornea is less than 500 microns, or if the postoperative residual stromal thickness is less than 250 microns, it increases the risk of developing keratectasia by 5%.[25][26]
Keratoconus
A cone-shaped cornea is an absolute contraindication for LASIK due to the risk of the condition causing corneal ectasia.[27] A practitioner must also be aware of subclinical keratoconus, including forme fruste keratoconus (FFK), which is, by definition, keratoconus that is not detectable with slit-lamp and corneal topography testing. Therefore, it may be a false negative.[28]
Uncontrolled Systemic Diseases
Systemic lupus erythematosus, Sjögren syndrome, rheumatoid arthritis, Graves disease, Crohn's disease, and other diseases that cause keratoconjunctivitis sicca or other forms of ocular pathology.[29]
Active Infection
Bacterial blepharitis and keratitis can increase the risk of spreading infection and inflammation through the cornea into the eye.
Relative Contraindications
Age
While LASIK is generally not advised for children due to the changes in refraction during adolescence, it has been successful in patients under 18 years old with high myopia or other severe pathologies.[30]
Herpes Zoster Ophthalmicus or Herpes Simplex Keratitis
Active infection by Herpes should be treated before surgery occurs. A study determined that it is safe to operate on patients with a history of ocular Herpes; however, it is recommended to wait one year for the virus to be in remission before surgical intervention.[31]
Cataract
Patients with mild cataracts may still receive LASIK surgery, but with the caveat that when the cataract progresses, visual acuity may be impaired despite LASIK. Intraocular lens implantation following cataract surgery is an indicated alternative procedure to LASIK.[23]
Glaucoma
Patients with glaucoma who undergo LASIK may develop a false decrease in intraocular pressure (IOP) after surgery due to decreased corneal thickness.[32] In addition, advanced patients with glaucoma have the risk of increased damage to the optic nerve during surgery due to the transient increase in intraocular pressure from the initial suction applied on the cornea.[33]
Corneal Dystrophy (CD)
Certain diseases like Fuchs endothelial corneal dystrophy may be accelerated with surgical interventions such as LASIK.[34] Patients with other forms of corneal dystrophies, such as granular corneal dystrophy and lattice corneal dystrophy, may receive LASIK, but recurrence of the disease is a possibility.[35]
Keloidosis
It is suggested by some sources that patients with a history of keloids may have their surgical results complicated by the disease.[19][23] However, it has been reported that patients with keloids undergoing refractive surgery report good outcomes.[36]
Pupil Size
It has been historically reported that patients with a larger pupil size may have an increased risk for postsurgical visual complications, such as halos/star-bursting with light, and glare.[37] However, with the advent of new technology lasers, larger ablation, and blend/transition zones, the correlation of large pupil size and visual complications is diminishing.[38]
Equipment
Excimer Laser
There are various excimer lasers approved by the United States Federal Drug Agency (US FDA), each with advantages that may be chosen according to the patient’s needs. Differences among lasers include beam size, beam repetition speed, and other benefits such as eye-tracking.[39] Today, the technical approach called custom-LASIK is often utilized, either using topography-guided (using the measured corneal topography to configure the laser) or wavefront-guided (calculating the light refraction off of the cornea to configure the laser) approaches.[40] These customized lasers may be used in conjunction with spot or slit-scanning lasers and help decrease post-surgical complications by shaping the cornea with more precision.[41]
Femtosecond Laser
Flap creation can be made with various approaches, as described in the technique section; however, the general approach with LASIK currently is to create the flap using a femtosecond laser. The advantage of the laser over mechanical techniques is that the flap can be created thinner and with more precision, which leads to better results and fewer flap-related complications after surgery.[42]
Preparation
Before a screening examination, contact lenses should be temporarily discontinued 1 to 2 weeks in advance to allow the corneal surface to stabilize, thus giving more accurate measurements.[23] A thorough history and physical examination should be completed to help identify any contraindications to LASIK. In addition to visual acuity testing, a full eye examination must be performed prior to considering surgery. This exam should include an assessment of general eye health by slit-lamp exam, fundoscopic exam, dry eye evaluation, and intraocular pressure.
The cornea is evaluated by keratometry and pachymetry.[43] Good candidates for LASIK will have a normal corneal thickness of approximately 550 microns.[25] Topography and tomography are crucial for good refractive screening and have become the standard of care for pre-operative screening to rule out keratoconus.[27]
For a more detailed evaluation of candidacy, the Randleman criteria can help screen patients who are at high risk for developing post-surgical corneal ectasia. The criteria consider variables such as topographical results, corneal thickness, age, and spherical manifest refraction.[44][45] A score of 4 or more is considered a high risk for developing post-LASIK ectasia.[44]
Once the patient is approved for LASIK, the Munnerlyn formula is used to calculate the ablation zone and depth for LASIK treatment, which incorporates the thickness of tissue ablated, the diameter of the optic zone, and the dioptric correction.[46] The percentage of tissue altered (PTA), which considers corneal thickness, ablation depth, and flap thickness, also helps physicians predict risk for post-LASIK corneal ectasia; it has been shown that a PTA of 40% or more is correlated with the development of ectasia.[47]
Technique or Treatment
Pre-Surgery
All equipment should be checked for safety, and to ensure patient topographical data is imported into the excimer laser. The patient should be given education on the routine of the procedure, as well as signing an informed consent document.
Surgical Technique
In general, LASIK surgery is performed in the following manner: the patient is brought to the table and placed in a comfortable supine position. The fellow eye is taped closed, and the operative eye is positioned open with a speculum.[19] The eye is anesthetized with eye drops. A suction ring is placed on the cornea, while the cornea is marked for flap creation by either a microkeratome or a femtosecond laser.[48] With the laser, the flap is delineated through the formation of micro-cavitation bubbles in a cleavage plane. The flap has a customized diameter, thickness, side-cut angle, hinge length, and hinge position. The femtosecond laser has largely superseded the microkeratome for flap creation.[49][50]
After the flap is created, the surgeon carefully reflects the flap to reveal the underlying stroma. The surgeon positions and signals the excimer laser to provide sculpting to the stromal surface through photoablation.[48] The surgeon then replaces the flap to its original position. It is safe for the patient to receive LASIK in both eyes on the same day.[19]
Post-Surgery
The patient instills preservative-free artificial tears because dry eyes are a common side-effect of surgery. Patients are advised to use artificial tears frequently, but if symptoms persist, the use of punctal plugs may be prescribed. The patient is also given antibiotics, and steroidal eye drops to use for 5 to 14 days after the surgery.[51] The patient follows up with their surgeon as prescribed by their practice, and after examination, may require additional minor LASIK adjustments to correct residual refractive error, known as an enhancement procedure, usually within a year of the initial procedure. Enhancement procedures occur in about 10% of patients and more frequently in patients with high initial corrections, over 40 years old, or with astigmatism.[52]
Alternate Procedures
There are other laser-assisted procedures that may be options for the patient with refractive errors. In addition, with advances in technology, variations to LASIK have been implemented successfully in practice.
PRK
One study shows that while LASIK has better results for visual acuity sooner after the surgery, patients with PRK tended to maintain better refraction years after the initial surgery.[53] Another study shows better outcomes with PRK, in patients with low to high myopia, with fewer complications compared to LASIK, despite other studies reporting better outcomes with LASIK.[54][55] Multiple studies show similar yet excellent outcomes in both procedures.[5] The physician must use clinical judgment in deciding which procedure will result in optimal outcomes for the patient. While pain has historically been labeled as a disadvantage of PRK, the use of bandage contact lenses and NSAIDs have led to a smooth post-op recovery with little pain.[19][23]
Femtosecond Lenticule Extraction (FLEx) or Small Incision Lenticule Extraction (SMILE)
The femtosecond laser removes the squamous epithelium without leaving a flap. It is indicated in patients with higher myopia (-6.00 D to -12.00 D) compared to LASIK.[2] Studies have shown similar clinical outcomes as compared to LASIK, with fewer incidences of dry eyes after surgery.[2][56]
Laser Epithelial Keratomileusis (LASEK)
Lasek is a procedure where an alcohol solution is used to assist in the removal of the superficial corneal layer. Epi-LASEK uses an epi-microkeratome to remove the layer. Both techniques are variants of PRK and can be considered as viable alternative procedures.[5]
Complications
Dry Eyes
One of the most common transient side-effects from LASIK is dry eyes due to a lack of tear production. This is due to the interruption of the lacrimal reflex as a result of nervous tissue being severed during the procedure.[23][56][57][58] Various studies have shown dry eyes to occur in 85% to 98% of patients one week after surgery.[57][59][60] This number drops to around 60% at 1 month [60]. Artificial tears and/or punctal plugs are applied until the nerves regenerate.
Visual Aberrations
20% of patients will report some form of visual change.[23] Some patients may suffer from visual changes such as glare, halo, or star-bursting patterns around lights, haze, and decreased contrast sensitivity. The FDA reports that visual disturbances tend to stabilize three to six months after the procedure.
Diffuse Lamellar Keratitis
Patients may also report blurriness and foreign body sensation that may be caused by diffuse lamellar keratitis (DLK), or “sands of Sahara” syndrome, a sterile inflammatory response.[23] Inflammatory cell infiltrates occur beneath the corneal flap interface.[61] This phenomenon may happen in as many as 1 in 50 cases of LASIK. DLK usually presents one to two days post-operatively and resolves with appropriate corticosteroid treatment after one week.[62]
Corneal Flap Complications
The incidence of microstriae, macrostriae, buttonholing, incomplete cap, free cap, cap dislodgement, and epithelial ingrowth after surgery, is a low-risk event, with 0.1-4% of patients reporting some form of complication.[1][23] It has been shown that corneal flap complications can lead to visual acuity loss.[56][63]
Post-LASIK Ectasia
A thin cornea before surgery may increase the risk of developing ectasia or further thinning of the cornea. The incidence has been reported from 0.04% to 0.6%.[44][64] Femtosecond-assisted LASIK can help prevent this complication due to the thinner flaps created.[65] The use of the Randleman criteria, as described in the preparation section, can also screen for patients who are at high risk of developing ectasia.[44]
Infectious Keratitis
Less than 0.1% of patients will develop an infection after LASIK.[66] The most common sources of infection come from gram-positive organisms, such as Staphylococcus species, or atypical mycobacteria, especially if the onset of infection is one-two weeks after surgery.[67]
Rare Complications
Ischemic optic neuropathy, retinal detachment, vitreous hemorrhage, and posterior vitreous detachment, are potential but very rare complications of LASIK, occurring in less than 0.1% of patients.[1][23][68][69][70]
Clinical Significance
While LASIK may be used in refractive errors, it was shown that this procedure is reliable in patients with myopia of - 6.0 D or less and astigmatism of less than 2.0 D.[71] A recent meta-analysis study showed similar improvement of visual acuity and patient safety with LASIK compared to other refractive surgical procedures.[72] This procedure has the added advantages of rapid recovery and decreased postoperative pain.[23][55] Several studies report a 92% to 95% rate of satisfaction among patients who obtained LASIK surgery.[4]
Enhancing Healthcare Team Outcomes
The professional team in LASIK treatment typically consists of ophthalmic surgeons, optometrists, nurses, medical assistants, and technicians. Team members work together in the outpatient setting to determine the best candidates for LASIK to prevent unnecessary costs and complications to the patient. The team, on the day of surgery, is responsible for adhering to standard clinical protocols, including obtaining the patient’s informed consent for the procedure, the correct marking of which eye will receive each specific treatment, the proper placement, and preoperative evaluation of necessary equipment for the procedure, a timeout called before the operation, and patient education throughout the treatment process. Communication among team members is vital, concerning any changes in patient status at any time before, during, or after the procedure and optimizes patient outcomes.[73] [Level 5]
Nursing, Allied Health, and Interprofessional Team Interventions
The team educates the patient regarding the procedure and obtains informed consent before surgery. They perform instrumentation checks with correct placement and distribution during the procedure and ensure sterility. Communication with other team members is crucial for patient safety.
Nursing, Allied Health, and Interprofessional Team Monitoring
The team guides the patient through post-procedure education for proper eye care, including the administration of prescribed eye drops. They assist with patient follow-up in an outpatient setting, with eye examinations to document visual acuity and visual changes.
Media
(Click Image to Enlarge)
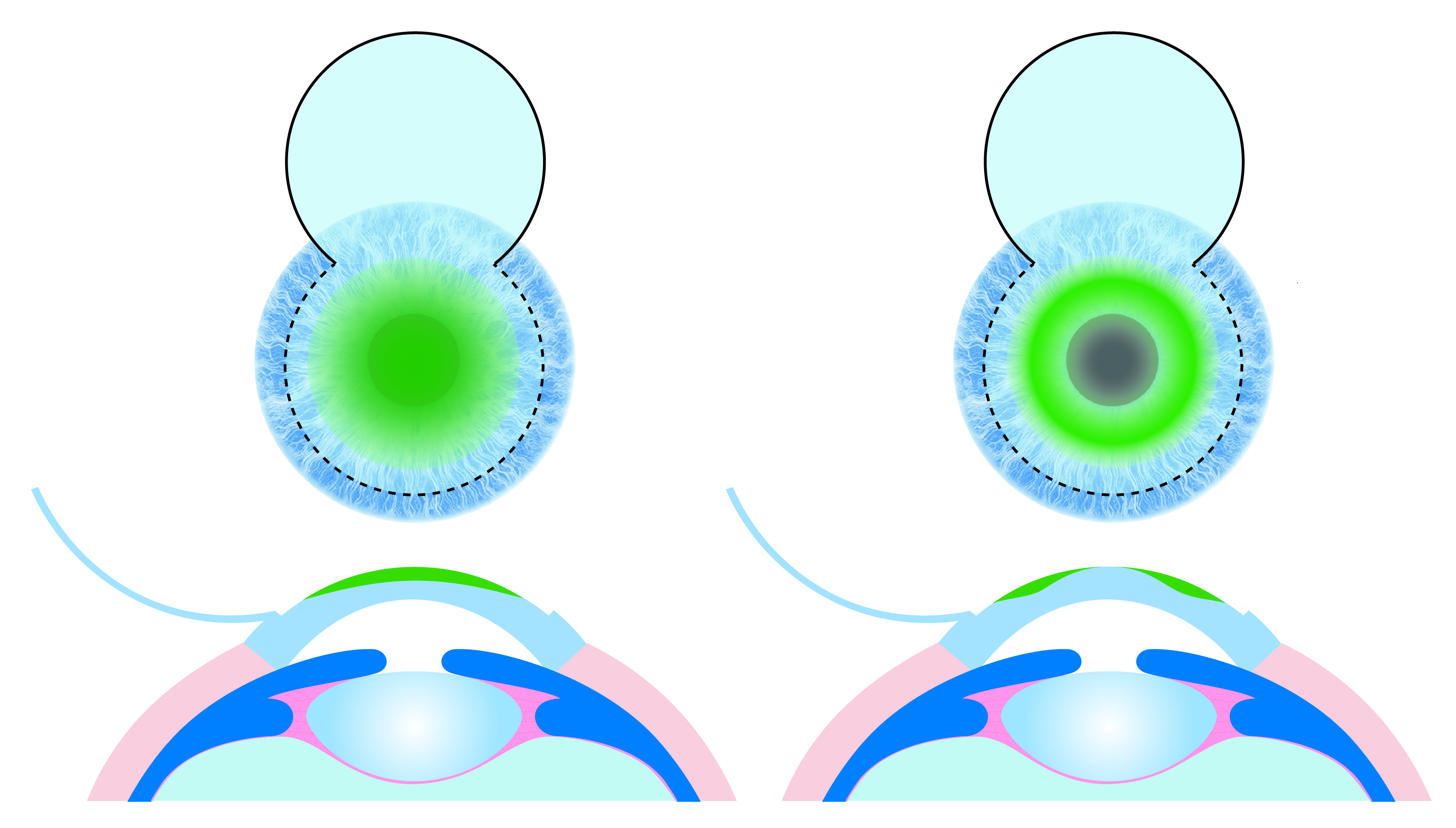
Figure 1. LASIK correction of myopia (left) flattens the central corneal surface, thus correcting the focal plane on the retina. LASIK correction of hyperopia (right) sculpts the cornea to make a steeper central area, thus correcting the focal plane on the retina. Contributed by Steven Linn, OD.
References
Ting DSJ, Srinivasan S, Danjoux JP. Epithelial ingrowth following laser in situ keratomileusis (LASIK): prevalence, risk factors, management and visual outcomes. BMJ open ophthalmology. 2018:3(1):e000133. doi: 10.1136/bmjophth-2017-000133. Epub 2018 Mar 29 [PubMed PMID: 29657982]
Shah R. History and Results; Indications and Contraindications of SMILE Compared With LASIK. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2019 Sep-Oct:8(5):371-376. doi: 10.1097/01.APO.0000580132.98159.fa. Epub [PubMed PMID: 31567264]
Moshirfar M, Shah TJ, Skanchy DF, Linn SH, Kang P, Durrie DS. Comparison and analysis of FDA reported visual outcomes of the three latest platforms for LASIK: wavefront guided Visx iDesign, topography guided WaveLight Allegro Contoura, and topography guided Nidek EC-5000 CATz. Clinical ophthalmology (Auckland, N.Z.). 2017:11():135-147. doi: 10.2147/OPTH.S115270. Epub 2017 Jan 4 [PubMed PMID: 28115827]
Tran K, Ryce A. Laser Refractive Surgery for Vision Correction: A Review of Clinical Effectiveness and Cost-effectiveness. 2018 Jun 22:(): [PubMed PMID: 30379512]
O'Brart DP. Excimer laser surface ablation: a review of recent literature. Clinical & experimental optometry. 2014 Jan:97(1):12-7. doi: 10.1111/cxo.12061. Epub 2013 May 8 [PubMed PMID: 23656608]
Chiam NPY, Mehta JS. Comparing Patient-Reported Outcomes of Laser In Situ Keratomileusis and Small-Incision Lenticule Extraction: A Review. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2019 Sep-Oct:8(5):377-384. doi: 10.1097/APO.0000000000000258. Epub [PubMed PMID: 31478935]
McAlinden C. Corneal refractive surgery: past to present. Clinical & experimental optometry. 2012 Jul:95(4):386-98. doi: 10.1111/j.1444-0938.2012.00761.x. Epub 2012 Jun 7 [PubMed PMID: 22672114]
Trokel SL, Srinivasan R, Braren B. Excimer laser surgery of the cornea. American journal of ophthalmology. 1983 Dec:96(6):710-5 [PubMed PMID: 6660257]
Level 3 (low-level) evidenceZarei-Ghanavati S, Nosrat N, Morovatdar N, Abrishami M, Eghbali P. Efficacy of corneal cooling on postoperative pain management after photorefractive keratectomy: A contralateral eye randomized clinical trial. Journal of current ophthalmology. 2017 Dec:29(4):264-269. doi: 10.1016/j.joco.2017.04.004. Epub 2017 May 11 [PubMed PMID: 29270472]
Level 1 (high-level) evidenceMcDonald MB, Kaufman HE, Frantz JM, Shofner S, Salmeron B, Klyce SD. Excimer laser ablation in a human eye. Case report. Archives of ophthalmology (Chicago, Ill. : 1960). 1989 May:107(5):641-2 [PubMed PMID: 2719572]
Level 3 (low-level) evidenceManche EE, Carr JD, Haw WW, Hersh PS. Excimer laser refractive surgery. The Western journal of medicine. 1998 Jul:169(1):30-8 [PubMed PMID: 9682628]
Ratkay-Traub I, Ferincz IE, Juhasz T, Kurtz RM, Krueger RR. First clinical results with the femtosecond neodynium-glass laser in refractive surgery. Journal of refractive surgery (Thorofare, N.J. : 1995). 2003 Mar-Apr:19(2):94-103 [PubMed PMID: 12701713]
Level 3 (low-level) evidenceNanda GG, Alone DP. REVIEW: Current understanding of the pathogenesis of Fuchs' endothelial corneal dystrophy. Molecular vision. 2019:25():295-310 [PubMed PMID: 31263352]
Level 3 (low-level) evidenceVaidyanathan U, Hopping GC, Liu HY, Somani AN, Ronquillo YC, Hoopes PC, Moshirfar M. Persistent Corneal Epithelial Defects: A Review Article. Medical hypothesis, discovery & innovation ophthalmology journal. 2019 Fall:8(3):163-176 [PubMed PMID: 31598519]
Salah T, Waring GO 3rd, el Maghraby A, Moadel K, Grimm SB. Excimer laser in situ keratomileusis under a corneal flap for myopia of 2 to 20 diopters. American journal of ophthalmology. 1996 Feb:121(2):143-55 [PubMed PMID: 8623883]
Level 2 (mid-level) evidenceArtini W, B Riyanto S, Hutauruk JA, D Gondhowiardjo T, Kekalih A. Predictive Factors for Successful High Myopia Treatment Using High-Frequency Laser-In-Situ Keratomileusis. The open ophthalmology journal. 2018:12():214-225. doi: 10.2174/1874364101812010214. Epub 2018 Jul 23 [PubMed PMID: 30123384]
Lindstrom RL, Linebarger EJ, Hardten DR, Houtman DM, Samuelson TW. Early results of hyperopic and astigmatic laser in situ keratomileusis in eyes with secondary hyperopia. Ophthalmology. 2000 Oct:107(10):1858-63; discussion 1863 [PubMed PMID: 11013186]
Level 1 (high-level) evidenceLyle WA, Jin GJ. Laser in situ keratomileusis for consecutive hyperopia after myopic LASIK and radial keratotomy. Journal of cataract and refractive surgery. 2003 May:29(5):879-88 [PubMed PMID: 12781270]
Bower KS, Weichel ED, Kim TJ. Overview of refractive surgery. American family physician. 2001 Oct 1:64(7):1183-90 [PubMed PMID: 11601800]
Level 3 (low-level) evidenceBuzard KA, Fundingsland BR. Excimer laser assisted in situ keratomileusis for hyperopia. Journal of cataract and refractive surgery. 1999 Feb:25(2):197-204 [PubMed PMID: 9951664]
Choi RY, Wilson SE. Hyperopic laser in situ keratomileusis: primary and secondary treatments are safe and effective. Cornea. 2001 May:20(4):388-93 [PubMed PMID: 11333326]
Level 2 (mid-level) evidenceMotwani M, Pei R. Treatment of moderate-to-high hyperopia with the WaveLight Allegretto 400 and EX500 excimer laser systems. Clinical ophthalmology (Auckland, N.Z.). 2017:11():999-1007. doi: 10.2147/OPTH.S136061. Epub 2017 May 24 [PubMed PMID: 28579751]
Wilkinson JM, Cozine EW, Kahn AR. Refractive Eye Surgery: Helping Patients Make Informed Decisions About LASIK. American family physician. 2017 May 15:95(10):637-644 [PubMed PMID: 28671403]
Hashmani S, Hashmani N, Kumar S, Kumar S, Dhomeja V, Razak S, Rajani H, Hanfi AN, Adhi I. Reasons for Refusing Laser-Assisted in Situ Keratomileusis in a Pakistani Population. Cureus. 2017 Jun 25:9(6):e1391. doi: 10.7759/cureus.1391. Epub 2017 Jun 25 [PubMed PMID: 28775931]
Probst LE, Machat JJ. Mathematics of laser in situ keratomileusis for high myopia. Journal of cataract and refractive surgery. 1998 Feb:24(2):190-5 [PubMed PMID: 9530593]
Binder PS. Ectasia after laser in situ keratomileusis. Journal of cataract and refractive surgery. 2003 Dec:29(12):2419-29 [PubMed PMID: 14709307]
Giri P, Azar DT. Risk profiles of ectasia after keratorefractive surgery. Current opinion in ophthalmology. 2017 Jul:28(4):337-342. doi: 10.1097/ICU.0000000000000383. Epub [PubMed PMID: 28594648]
Level 3 (low-level) evidenceLuz A, Lopes B, Hallahan KM, Valbon B, Fontes B, Schor P, Dupps WJ Jr, Ambrósio R Jr. Discriminant Value of Custom Ocular Response Analyzer Waveform Derivatives in Forme Fruste Keratoconus. American journal of ophthalmology. 2016 Apr:164():14-21. doi: 10.1016/j.ajo.2015.12.020. Epub 2015 Dec 29 [PubMed PMID: 26743618]
Sutton G, Lawless M, Hodge C. Laser in situ keratomileusis in 2012: a review. Clinical & experimental optometry. 2014 Jan:97(1):18-29. doi: 10.1111/cxo.12075. Epub 2013 Jun 21 [PubMed PMID: 23786377]
O'Keefe M, Nolan L. LASIK surgery in children. The British journal of ophthalmology. 2004 Jan:88(1):19-21 [PubMed PMID: 14693763]
de Rojas Silva V, Rodríguez-Conde R, Cobo-Soriano R, Beltrán J, Llovet F, Baviera J. Laser in situ keratomileusis in patients with a history of ocular herpes. Journal of cataract and refractive surgery. 2007 Nov:33(11):1855-9 [PubMed PMID: 17964388]
Level 3 (low-level) evidenceAjazaj V, Kaçaniku G, Asani M, Shabani A, Dida E. Intraocular Pressure After Corneal Refractive Surgery. Medical archives (Sarajevo, Bosnia and Herzegovina). 2018 Nov:72(5):341-343. doi: 10.5455/medarh.2018.72.341-343. Epub [PubMed PMID: 30524165]
Osman E. Laser refractive surgery in glaucoma patients. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2011 Apr:25(2):169-73. doi: 10.1016/j.sjopt.2010.04.003. Epub 2010 Apr 21 [PubMed PMID: 23960918]
Güell JL, El Husseiny MA, Manero F, Gris O, Elies D. Historical Review and Update of Surgical Treatment for Corneal Endothelial Diseases. Ophthalmology and therapy. 2014 Dec:3(1-2):1-15. doi: 10.1007/s40123-014-0022-y. Epub 2014 Feb 18 [PubMed PMID: 25134494]
Jun I, Jung JW, Choi YJ, Kim TI, Seo KY, Kim EK. Long-term Clinical Outcomes of Phototherapeutic Keratectomy in Corneas With Granular Corneal Dystrophy Type 2 Exacerbated After LASIK. Journal of refractive surgery (Thorofare, N.J. : 1995). 2018 Feb 1:34(2):132-139. doi: 10.3928/1081597X-20171220-01. Epub [PubMed PMID: 29425392]
Level 2 (mid-level) evidenceLee JY, Youm DJ, Choi CY. Conventional Epi-LASIK and lamellar epithelial debridement in myopic patients with dermatologic keloids. Korean journal of ophthalmology : KJO. 2011 Jun:25(3):206-9. doi: 10.3341/kjo.2011.25.3.206. Epub 2011 May 24 [PubMed PMID: 21655048]
Level 3 (low-level) evidenceTeus MA, de Benito-Llopis L, García-González M. Comparison of visual results between laser-assisted subepithelial keratectomy and epipolis laser in situ keratomileusis to correct myopia and myopic astigmatism. American journal of ophthalmology. 2008 Sep:146(3):357-362. doi: 10.1016/j.ajo.2008.05.022. Epub 2008 Jul 9 [PubMed PMID: 18614136]
Level 2 (mid-level) evidenceMyung D, Schallhorn S, Manche EE. Pupil size and LASIK: a review. Journal of refractive surgery (Thorofare, N.J. : 1995). 2013 Nov:29(11):734-41. doi: 10.3928/1081597X-20131021-02. Epub [PubMed PMID: 24203804]
Khoramnia R, Salgado JP, Wuellner C, Donitzky C, Lohmann CP, Winkler von Mohrenfels C. Safety, efficacy, predictability and stability of laser in situ keratomileusis (LASIK) with a 1000-Hz scanning spot excimer laser. Acta ophthalmologica. 2012 Sep:90(6):508-13. doi: 10.1111/j.1755-3768.2010.02052.x. Epub 2011 Jan 25 [PubMed PMID: 21266022]
Level 3 (low-level) evidenceEl Awady HE, Ghanem AA, Saleh SM. Wavefront-optimized ablation versus topography-guided customized ablation in myopic LASIK: comparative study of higher order aberrations. Ophthalmic surgery, lasers & imaging : the official journal of the International Society for Imaging in the Eye. 2011 Jul-Aug:42(4):314-20. doi: 10.3928/15428877-20110421-01. Epub 2011 Apr 28 [PubMed PMID: 21534496]
Level 1 (high-level) evidenceShehadeh MM, Akkawi MT, Aghbar AA, Musmar MT, Khabbas MN, Kharouf MF, Al-Labadi L. Outcomes of Wavefront-Optimized Laser-Assisted In-Situ Keratomileusis and Photorefractive Keratectomy for correction of Myopia and Myopic Astigmatism over One Year Follow-Up. The open ophthalmology journal. 2018:12():256-263. doi: 10.2174/1874364101812010256. Epub 2018 Sep 26 [PubMed PMID: 30294393]
Bashir ZS, Ali MH, Anwar A, Ayub MH, Butt NH. Femto-lasik: The recent innovation in laser assisted refractive surgery. JPMA. The Journal of the Pakistan Medical Association. 2017 Apr:67(4):609-615 [PubMed PMID: 28420926]
Kim CY, Song JH, Na KS, Chung SH, Joo CK. Factors influencing corneal flap thickness in laser in situ keratomileusis with a femtosecond laser. Korean journal of ophthalmology : KJO. 2011 Feb:25(1):8-14. doi: 10.3341/kjo.2011.25.1.8. Epub 2011 Jan 17 [PubMed PMID: 21350688]
Randleman JB, Woodward M, Lynn MJ, Stulting RD. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008 Jan:115(1):37-50 [PubMed PMID: 17624434]
Level 2 (mid-level) evidenceRandleman JB, Trattler WB, Stulting RD. Validation of the Ectasia Risk Score System for preoperative laser in situ keratomileusis screening. American journal of ophthalmology. 2008 May:145(5):813-8. doi: 10.1016/j.ajo.2007.12.033. Epub 2008 Mar 10 [PubMed PMID: 18328998]
Level 2 (mid-level) evidenceMeyer B, Sluyterman van Langeweyde G, Wottke M. Refractive outcomes of an advanced aspherically optimized profile for myopia corrections by LASIK: a retrospective comparison with the standard aspherically optimized profile. Clinical ophthalmology (Auckland, N.Z.). 2015:9():379-92. doi: 10.2147/OPTH.S75812. Epub 2015 Feb 23 [PubMed PMID: 25750516]
Level 2 (mid-level) evidenceOng HS, Farook M, Tan BBC, Williams GP, Santhiago MR, Mehta JS. Corneal Ectasia Risk And Percentage Tissue Altered In Myopic Patients Presenting For Refractive Surgery. Clinical ophthalmology (Auckland, N.Z.). 2019:13():2003-2015. doi: 10.2147/OPTH.S215144. Epub 2019 Oct 14 [PubMed PMID: 31686775]
Kohnen T, Strenger A, Klaproth OK. Basic knowledge of refractive surgery: correction of refractive errors using modern surgical procedures. Deutsches Arzteblatt international. 2008 Feb:105(9):163-70; quiz 170-2. doi: 10.3238/arztebl.2008.0163. Epub 2008 Feb 29 [PubMed PMID: 19633786]
Xia LK, Yu J, Chai GR, Wang D, Li Y. Comparison of the femtosecond laser and mechanical microkeratome for flap cutting in LASIK. International journal of ophthalmology. 2015:8(4):784-90. doi: 10.3980/j.issn.2222-3959.2015.04.25. Epub 2015 Aug 18 [PubMed PMID: 26309880]
Pajic B, Vastardis I, Pajic-Eggspuehler B, Gatzioufas Z, Hafezi F. Femtosecond laser versus mechanical microkeratome-assisted flap creation for LASIK: a prospective, randomized, paired-eye study. Clinical ophthalmology (Auckland, N.Z.). 2014:8():1883-9. doi: 10.2147/OPTH.S68124. Epub 2014 Sep 22 [PubMed PMID: 25284975]
Level 1 (high-level) evidenceCampos M, Muccioli C, Malta JB, Gerade RA, LA Salame A, Belfort R. Efficacy and tolerability of a combined gatifloxacin plus prednisolone formulation for topical prophylaxis after LASIK. Clinical ophthalmology (Auckland, N.Z.). 2011:5():209-14. doi: 10.2147/OPTH.S17059. Epub 2011 Feb 15 [PubMed PMID: 21386913]
Hersh PS, Fry KL, Bishop DS. Incidence and associations of retreatment after LASIK. Ophthalmology. 2003 Apr:110(4):748-54 [PubMed PMID: 12689897]
Level 2 (mid-level) evidenceMori Y, Miyata K, Ono T, Yagi Y, Kamiya K, Amano S. Comparison of laser in situ ketatomileusis and photorefractive keratectomy for myopia using a mixed-effects model. PloS one. 2017:12(3):e0174810. doi: 10.1371/journal.pone.0174810. Epub 2017 Mar 31 [PubMed PMID: 28362808]
Ghadhfan F, Al-Rajhi A, Wagoner MD. Laser in situ keratomileusis versus surface ablation: visual outcomes and complications. Journal of cataract and refractive surgery. 2007 Dec:33(12):2041-8 [PubMed PMID: 18053901]
Level 2 (mid-level) evidenceAlió JL, Ortiz D, Muftuoglu O, Garcia MJ. Ten years after photorefractive keratectomy (PRK) and laser in situ keratomileusis (LASIK) for moderate to high myopia (control-matched study). The British journal of ophthalmology. 2009 Oct:93(10):1313-8. doi: 10.1136/bjo.2007.131748. Epub 2008 Feb 21 [PubMed PMID: 18292203]
Level 2 (mid-level) evidenceToda I. Dry Eye After LASIK. Investigative ophthalmology & visual science. 2018 Nov 1:59(14):DES109-DES115. doi: 10.1167/iovs.17-23538. Epub [PubMed PMID: 30481814]
Xie W. Recent advances in laser in situ keratomileusis-associated dry eye. Clinical & experimental optometry. 2016 Mar:99(2):107-12. doi: 10.1111/cxo.12361. Epub [PubMed PMID: 27012690]
Level 3 (low-level) evidenceToda I, Asano-Kato N, Komai-Hori Y, Tsubota K. Dry eye after laser in situ keratomileusis. American journal of ophthalmology. 2001 Jul:132(1):1-7 [PubMed PMID: 11438046]
De Paiva CS, Chen Z, Koch DD, Hamill MB, Manuel FK, Hassan SS, Wilhelmus KR, Pflugfelder SC. The incidence and risk factors for developing dry eye after myopic LASIK. American journal of ophthalmology. 2006 Mar:141(3):438-45 [PubMed PMID: 16490488]
Level 1 (high-level) evidenceYu EY, Leung A, Rao S, Lam DS. Effect of laser in situ keratomileusis on tear stability. Ophthalmology. 2000 Dec:107(12):2131-5 [PubMed PMID: 11097583]
Level 1 (high-level) evidenceSmith RJ, Maloney RK. Diffuse lamellar keratitis. A new syndrome in lamellar refractive surgery. Ophthalmology. 1998 Sep:105(9):1721-6 [PubMed PMID: 9754183]
Level 3 (low-level) evidenceLinebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: diagnosis and management. Journal of cataract and refractive surgery. 2000 Jul:26(7):1072-7 [PubMed PMID: 10946202]
Stulting RD, Carr JD, Thompson KP, Waring GO 3rd, Wiley WM, Walker JG. Complications of laser in situ keratomileusis for the correction of myopia. Ophthalmology. 1999 Jan:106(1):13-20 [PubMed PMID: 9917775]
Level 1 (high-level) evidencePallikaris IG, Kymionis GD, Astyrakakis NI. Corneal ectasia induced by laser in situ keratomileusis. Journal of cataract and refractive surgery. 2001 Nov:27(11):1796-802 [PubMed PMID: 11709254]
Level 2 (mid-level) evidencePerez-Straziota C, Randleman JB. Femtosecond-assisted LASIK: Complications and Management. International ophthalmology clinics. 2016 Spring:56(2):59-66. doi: 10.1097/IIO.0000000000000105. Epub [PubMed PMID: 26938338]
Llovet F, de Rojas V, Interlandi E, Martín C, Cobo-Soriano R, Ortega-Usobiaga J, Baviera J. Infectious keratitis in 204 586 LASIK procedures. Ophthalmology. 2010 Feb:117(2):232-8.e1-4. doi: 10.1016/j.ophtha.2009.07.011. Epub 2009 Dec 14 [PubMed PMID: 20006909]
Level 2 (mid-level) evidenceLinke SJ, Richard G, Katz T. [Infectious keratitis after LASIK--update and survey of the literature]. Klinische Monatsblatter fur Augenheilkunde. 2011 Jun:228(6):531-6. doi: 10.1055/s-0029-1245549. Epub 2010 Nov 24 [PubMed PMID: 21108166]
Level 3 (low-level) evidenceLuna JD, Artal N, Reviglio VE, Juarez CP. LASIK-induced optic neuropathy. Ophthalmology. 2002 May:109(5):817-8 [PubMed PMID: 11986055]
Level 3 (low-level) evidenceArevalo JF, Lasave AF, Torres F, Suarez E. Rhegmatogenous retinal detachment after LASIK for myopia of up to -10 diopters: 10 years of follow-up. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2012 Jul:250(7):963-70. doi: 10.1007/s00417-011-1907-2. Epub 2012 Jan 5 [PubMed PMID: 22218710]
Level 2 (mid-level) evidenceAl-Rashaed S, Al-Halafi AM. Retinal detachment after laser in situ keratomileusis. Middle East African journal of ophthalmology. 2011 Jul:18(3):224-7. doi: 10.4103/0974-9233.84052. Epub [PubMed PMID: 21887078]
Sugar A, Rapuano CJ, Culbertson WW, Huang D, Varley GA, Agapitos PJ, de Luise VP, Koch DD. Laser in situ keratomileusis for myopia and astigmatism: safety and efficacy: a report by the American Academy of Ophthalmology. Ophthalmology. 2002 Jan:109(1):175-87 [PubMed PMID: 11772601]
Wen D, McAlinden C, Flitcroft I, Tu R, Wang Q, Alió J, Marshall J, Huang Y, Song B, Hu L, Zhao Y, Zhu S, Gao R, Bao F, Yu A, Yu Y, Lian H, Huang J. Postoperative Efficacy, Predictability, Safety, and Visual Quality of Laser Corneal Refractive Surgery: A Network Meta-analysis. American journal of ophthalmology. 2017 Jun:178():65-78. doi: 10.1016/j.ajo.2017.03.013. Epub 2017 Mar 20 [PubMed PMID: 28336402]
Level 2 (mid-level) evidenceBrown MJ. Comanagement of refractive surgery. International ophthalmology clinics. 2000 Summer:40(3):21-7 [PubMed PMID: 10941643]