Introduction
Poorly controlled hypertension (HTN) affects several systems such as the cardiovascular, renal, cerebrovascular, and retina. The damage to these systems is known as target-organ damage (TOD).[1] HTN affects the eye causing 3 types of ocular damage: choroidopathy, retinopathy, and optic neuropathy.[2] Hypertensive retinopathy (HR) occurs when the retinal vessels get damaged due to elevated blood pressure. There has been significant evidence that hypertensive retinopathy acts as a predictor of systemic morbidity and mortality due to TOD.[1] A study by Erden et al. showed that the increase in the incidence of retinopathy is related to the degree of severity and duration of HTN.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Apart from essential and secondary hypertension, there are other factors which play an important role in the development of hypertensive retinopathy. The prevalence of hypertensive retinopathy is more in Afro-Caribbean as compared to Europeans and more in women as compared to men. Genetic factors can also play a role with certain genotypes associated with an increased risk of hypertensive retinopathy.[4] Pontremoli et al. studied the genetic factors linked to hypertensive retinopathy and found the deletion of the allele of the angiotensin-converting enzyme has a higher risk associated with the development of hypertensive retinopathy.[5] Smoking is considered to have a strong association with severe or malignant hypertensive retinopathy as studied by Poulter et al.[6] Renal dysfunction (persistent microalbuminuria and low creatinine clearance) in patients has shown to be a marker for hypertensive retinopathy and end-organ damage.[7] Uckaya et al. found an association with plasma leptin. It was observed that plasma leptin levels were higher in patients with hypertensive retinopathy and postulated that it is associated with vascular endothelium damage.[8]
Epidemiology
The severity and duration of hypertension are directly proportional to the incidence of hypertensive retinopathy as studied by Erden et al. The incidence of hypertensive retinopathy in their study was 66.3%[3]. Kabedi et al. stated hypertensive retinopathy incidence of 83.6% out of the total hypertensive patients and found chronic kidney disease to be the most significant factor to predict severe hypertensive retinopathy.[1] As per the study conducted by Del Brutto et al., hypertensive retinopathy grade 1 was recorded in 37%, and grade 2 hypertensive retinopathy was noted in 17% of hypertensive patients.[9]
Pathophysiology
Retinal blood vessels have distinct features, which differentiate them from other blood vessels[10]:
- The absence of sympathetic nerve supply
- Autoregulation of blood flow
- Presence of blood-retinal barrier
Thus, an increase in blood pressure (BP) is transferred directly to the vessels which initially constrict. However, a further increase in BP overcomes this compensatory tone and damage to the muscle layer and endothelium ensues.
Hypertensive retinopathy has the following phases[2]:
Vasoconstrictive Phase
In this phase, the local autoregulatory mechanisms come into play. This causes vasospasm and retinal arteriole narrowing, which is evident by the decrease in the arteriole to venule ratio (Normal = 2:3). In older patients with arteriosclerosis, focal arteriolar narrowing develops, as affected vascular segments cannot undergo narrowing.
Sclerotic Phase
Persistent increase in BP causes certain changes in vessel wall:
- Intima layer: Thickening
- Media layer: Hyperplasia
- Arteriolar wall: Hyaline degeneration
This leads to a severe form of arteriolar narrowing, arteriovenous (AV) crossing changes, and widening and accentuation of light reflex (silver and copper wiring). AV crossing changes occur when a thickened arteriole crosses over a venule and subsequently compresses it as the vessels share a common adventitious sheath. The vein, in turn, appears dilated and torturous distal to the AV crossing.
Exudative Phase
Seen in patients with severely increased BP; characterized by the disruption of the blood-brain barrier and leakage of blood and plasma into the vessel wall disrupting the autoregulatory mechanisms. In this stage, retinal signs occur such as retinal hemorrhage (flame-shaped and dot blot), hard exudate formation, necrosis of smooth muscle cells and retinal ischemia (cotton-wool spots).
Malignant Hypertension
Severe intracranial hypertension leads to optic nerve ischemia and edema (papilledema). Also, fibrinoid necrosis of choroidal arterioles occurs leading to segmental infarction of choriocapillaries. This gives rise to:
- Elschnig's spots: Where the overlying retinal pigment epithelium (RPE) appears yellow
- Siegrist's streak: RPE hyperplasia over choroidal infarcts
- Neurosensory RPE detachments
These signs are termed as choroidopathy.
History and Physical
Clinical Features[4]
Hypertensive retinopathy is usually asymptomatic and is diagnosed on fundoscopic features. The following are signs of hypertensive retinopathy.
AV Crossing Changes
- Salus’s sign: Deflection of retinal vein as it crosses the arteriole.
- Gunn’s sign: Tapering of the retinal vein on either side of the AV crossing.
- Bonnet’s sign: Banking of the retinal vein distal to the AV crossing.
Arterial Changes
- Decrease in the arteriovenous ratio to 1:3 ( the normal ratio is 2:3).
- Change in the arteriolar light reflex (light reflex appears as copper and/or silver wiring)
Retinal Changes
- Retinal hemorrhages:
- Dot-blot hemorrhages: Bleeding in the inner retinal layer
- Flame shaped hemorrhage: Bleeding is in the superficial retinal layer
- Retinal exudates:
- Hard exudates: Lipid deposits in the retina
- Soft exudates: These are also known as cotton wool spots which appear due to ischemia of the nerve fibers
Macular Changes
Macular star formation due to deposition of hard exudates around the macula.
Optic Nerve Changes
Optic disk swelling (also known as hypertensive optic neuropathy)
In a study by Wong et al., they identified certain retinal signs to be associated with increased risk for stroke. The signs are AV nicking, focal arteriolar narrowing (as this is associated with arteriosclerosis), microaneurysms, cotton wool spots, retinal hemorrhages (dot blot and flame-shaped), and decreased AV ratio.[11]
Evaluation
Classification
The following are classification systems for hypertensive retinopathy based on fundus examination with indirect ophthalmoscopy or +90 D lens.
Keith-Wagner- Barker classification
- Group 1: Slight constriction of retinal arterioles
- Group 2: Group 1 + focal narrowing of retinal arterioles + AV nicking
- Group 3: Group 2 + flame-shaped haemorrhages + cotton-wool spots + hard exudates
- Group 4: Group 3 + optic disc swelling
Scheie Classification
For Hypertensive Retinopathy
- Stage 0: No visible abnormalities
- Stage 1: Diffuse arteriolar narrowing
- Stage 2: Stage 1 + focal arteriolar constriction
- Stage 3: Stage 2 + retinal hemorrhage
- Stage 4: Stage 3 + hard exudates + retinal edema+ optic disc swelling
For Arteriosclerosis
- Stage 0: Normal
- Stage 1: Broadening of arteriolar light reflex
- Stage 2: Stage 1 + AV crossing changes
- Stage 3: Copper wiring of arterioles
- Stage 4: Silver wiring of arterioles
Treatment / Management
The main purpose of screening for hypertensive retinopathy is that retinal vessels are the only blood vessels visible on routine examination. The effects of chronically elevated HTN are easily visible in the eye as hypertensive retinopathy and choroidopathy, and this reflects the vascular changes occurring in other systems. Ophthalmologists and general physicians should work in collaborations to ensure that hypertensive patients are efficiently screened, and timely managed to reduce the risk of ocular and systemic morbidity and mortality.[12] Henderson et al., however, noted that Hypertensive retinopathy is associated with an increased risk of stroke even after controlling BP and other vascular risk factors.[2]
The management of hypertensive retinopathy depends on the severity of the disease:
- Mild hypertensive retinopathy: The treatment consists of controlling of BP with regular monitoring.
- Moderate hypertensive retinopathy: Referral to a physician is essential to exclude other associated factors like diabetes mellitus and to check for any cardiovascular abnormalities. Routine care including BP control and monitoring is a must.
- Severe hypertensive retinopathy: Requires urgent treatment and referral as it has the strongest association with mortality. Other systems such as renal, cardiovascular, and brain should be monitored for signs of TOD.
Important to note is that BP should be lowered in a controlled fashion. This is crucial to prevent ischemic damage to vital organs such as optic nerve and brain.
Differential Diagnosis
The other conditions which present with optic disc swelling are:
- Diabetic papillopathy
- Central retinal vein occlusion
- Anterior ischemic optic neuropathy
- Neuroretinitis
Conditions which mimic chronic hypertensive retinopathy are:
- Diabetic retinopathy
- Retinal venous obstruction
- Hyperviscosity syndrome
- Ocular ischemic syndrome
- Radiation retinopathy
Prognosis
Chronic hypertensive retinopathy rarely causes significant visual loss. The retinal changes can be halted when hypertension is treated. However, arteriolar narrowing and AV changes persist. For untreated malignant hypertension, the mortality is high as 50% within 2 months of diagnosis and almost 90% by the end of 1 year.[13] Vision loss in hypertensive retinopathy is because of either secondary optic atrophy after prolonged papilloedema or retinal pigmentary changes after exudative retinal detachment.
Complications
Complications include[14]:
- Retinal artery occlusion
- Retinal vein occlusion
- Macro aneurysm of retinal arteriole
- Diabetic retinopathy (DR): Both hypertensive retinopathy and DR together in a patient is called as mixed retinopathy. HTN is also known to be a major risk factor for the progression of DR.
- Anterior ischemic optic neuropathy
- Age-related macular degeneration
- Glaucoma
- Retinal arteriolar emboli
- Epiretinal membrane formation
- Cystoid macular edema
Enhancing Healthcare Team Outcomes
Hypertension has effects on multiple systems, and it is important to have care coordination between the physician, physician assistant, nurse practitioner, ophthalmologist, nephrologist, and cardiologist to ensure early detection and control of hypertension and improve patient outcomes. Patients with hypertension need to be informed that they should follow up regularly with an ophthalmologist for a complete eye assessment. In addition, patients need to be educated about the importance of compliance with antihypertensive medications.[15] (Level V)
Outcomes
In most patients, hypertensive retinopathy does not cause vision loss as long as the hypertension is treated. However, if the blood pressure remains untreated, it can lead to vision loss within a short period of time. The cause of the vision loss is either due to retinal pigmentary changes or secondary to optic atrophy, neither of which is reversible. [16](Level V)
Media
(Click Image to Enlarge)
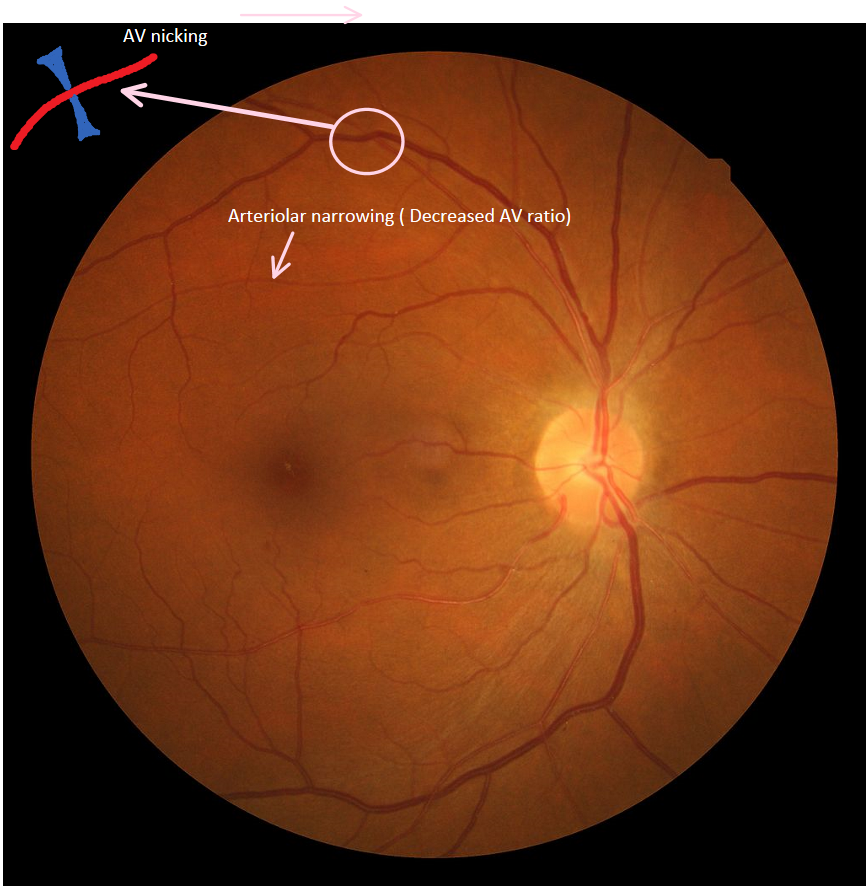
Hypertensive Retinopathy Contributed by Pranav Modi
References
Kabedi NN, Mwanza JC, Lepira FB, Kayembe TK, Kayembe DL. Hypertensive retinopathy and its association with cardiovascular, renal and cerebrovascular morbidity in Congolese patients. Cardiovascular journal of Africa. 2014 Sep-Oct:25(5):228-32. doi: 10.5830/CVJA-2014-045. Epub [PubMed PMID: 25629539]
Henderson AD, Bruce BB, Newman NJ, Biousse V. Hypertension-related eye abnormalities and the risk of stroke. Reviews in neurological diseases. 2011:8(1-2):1-9 [PubMed PMID: 21769065]
Erden S, Bicakci E. Hypertensive retinopathy: incidence, risk factors, and comorbidities. Clinical and experimental hypertension (New York, N.Y. : 1993). 2012:34(6):397-401. doi: 10.3109/10641963.2012.663028. Epub 2012 Apr 2 [PubMed PMID: 22468968]
Chatterjee S, Chattopadhyay S, Hope-Ross M, Lip PL. Hypertension and the eye: changing perspectives. Journal of human hypertension. 2002 Oct:16(10):667-75 [PubMed PMID: 12420190]
Level 3 (low-level) evidencePontremoli R, Sofia A, Tirotta A, Ravera M, Nicolella C, Viazzi F, Bezante GP, Borgia L, Bobola N, Ravazzolo R, Sacchi G, Deferrari G. The deletion polymorphism of the angiotensin I-converting enzyme gene is associated with target organ damage in essential hypertension. Journal of the American Society of Nephrology : JASN. 1996 Dec:7(12):2550-8 [PubMed PMID: 8989733]
Poulter NR. Independent effects of smoking on risk of hypertension: small, if present. Journal of hypertension. 2002 Feb:20(2):171-2 [PubMed PMID: 11821697]
Biesenbach G, Zazgornik J. High prevalence of hypertensive retinopathy and coronary heart disease in hypertensive patients with persistent microalbuminuria under short intensive antihypertensive therapy. Clinical nephrology. 1994 Apr:41(4):211-8 [PubMed PMID: 8026113]
Uckaya G, Ozata M, Sonmez A, Kinalp C, Eyileten T, Bingol N, Koc B, Kocabalkan F, Ozdemir IC. Is leptin associated with hypertensive retinopathy? The Journal of clinical endocrinology and metabolism. 2000 Feb:85(2):683-7 [PubMed PMID: 10690876]
Del Brutto OH, Mera RM, Viteri EM, Pólit J, Ledesma EA, Cano JA, Plaza KJ, Zambrano M, Costa AF. Hypertensive retinopathy and cerebral small vessel disease in Amerindians living in rural Ecuador: The Atahualpa Project. International journal of cardiology. 2016 Sep 1:218():65-68. doi: 10.1016/j.ijcard.2016.05.020. Epub 2016 May 13 [PubMed PMID: 27232913]
Chaine G, Kohner EM. [Hypertensive retinopathy]. Journal francais d'ophtalmologie. 1983:6(12):995-1005 [PubMed PMID: 6674324]
Level 3 (low-level) evidenceWong TY, Klein R, Couper DJ, Cooper LS, Shahar E, Hubbard LD, Wofford MR, Sharrett AR. Retinal microvascular abnormalities and incident stroke: the Atherosclerosis Risk in Communities Study. Lancet (London, England). 2001 Oct 6:358(9288):1134-40 [PubMed PMID: 11597667]
Fraser-Bell S, Symes R, Vaze A. Hypertensive eye disease: a review. Clinical & experimental ophthalmology. 2017 Jan:45(1):45-53. doi: 10.1111/ceo.12905. Epub 2017 Jan 21 [PubMed PMID: 27990740]
Keith NM, Wagener HP, Barker NW. Some different types of essential hypertension: their course and prognosis. The American journal of the medical sciences. 1974 Dec:268(6):336-45 [PubMed PMID: 4616627]
Bhargava M, Ikram MK, Wong TY. How does hypertension affect your eyes? Journal of human hypertension. 2012 Feb:26(2):71-83. doi: 10.1038/jhh.2011.37. Epub 2011 Apr 21 [PubMed PMID: 21509040]
Wolz J, Audebert H, Laumeier I, Ahmadi M, Steinicke M, Ferse C, Michelson G. Telemedical assessment of optic nerve head and retina in patients after recent minor stroke or TIA. International ophthalmology. 2017 Feb:37(1):39-46. doi: 10.1007/s10792-016-0222-7. Epub 2016 Mar 26 [PubMed PMID: 27016938]
Do DV, Wang X, Vedula SS, Marrone M, Sleilati G, Hawkins BS, Frank RN. Blood pressure control for diabetic retinopathy. The Cochrane database of systematic reviews. 2015 Jan 31:1():CD006127. doi: 10.1002/14651858.CD006127.pub2. Epub 2015 Jan 31 [PubMed PMID: 25637717]
Level 1 (high-level) evidence