Introduction
“Intraepidermal” means that the cancerous cells are located in the epidermis from where they originally developed (in situ). Squamous cell carcinoma in situ (SCCIS) is a vitiated, superficial growth of cancerous cells on the skin’s outer layer. It is not a severe condition but could develop into a full form of invasive skin cancer if not detected early or well managed. It is also known as carcinoma in situ in the literature or as Bowen disease after John T. Bowen, an American dermatologist who first described the condition in 1912. Flat cells, known as squamous cells, are located in the epidermis. They are responsible for the production of the keratin protein and affected by this condition.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Intraepidermal or squamous cell carcinoma in situ was first attributed to exposure of unprotected body parts to ionizing radiation in the year 1920. However, population studies today show that the most common cause of carcinoma is long-term exposure of the skin and dermal layers to sunlight. Ultraviolet radiation damages the skin cell nucleic acids, leading to the mutation and cloning of the p53 gene. The resulting exposure to ultraviolet UV radiation leads to a geometric growth of skin cells. Auto function cell repairs also are impeded by exposure to ultraviolet (UV) from sunlight. Diseases or drugs capable of suppressing immune responses to skin damage also can trigger the mutation of squamous cells. Other causatives attributed to intraepidermal squamous cell carcinoma include arsenic ingestion and some viral infections.[4][5]
Epidemiology
A Minnesota study of the disease's frequency in US population in 1991 reported the annual average case of squamous cell carcinoma (SCC) in situ to be 14.9 cases per 100,000 whites. In 1994, it was recorded that the frequency had multiplied by a geometric factor of 10. The disease is usually frequent and most reported in whites and rarely in people who have a dark-pigmented skin. The disease has an equal ratio of distribution across both genders and often can occur in middle-aged and elderly patients.
Pathophysiology
Squamous cell carcinoma (SCC) is a malignant form of keratinocyte skin cancer. It appears as pigmented or verrucous tumor forms and can progressively develop into squamous cell carcinoma. A common feature is the simultaneous occurrence of basal cell carcinoma in patients with conditions of squamous cell carcinoma.
Histopathology
Microscopic examination is of great importance, especially for the diagnosis of squamous cell carcinoma in situ. It considers the features of the specimen obtained via biopsy regarding invasion, differentiation, and depth. Note that biopsy specimens usually include samples of the normal tissue which would be used in spotting the differences; also, there is the need for a full thickness biopsy to determine the depth of lesion and invasion levels correctly. Histopathologically, hyperkeratosis, and parakeratosis is noted in the epidermis. Prominent acanthosis along with elongation and thickening of the rete ridges is usually observed. These change over highly atypical keratinocyte cells. The atypical cells span the full thickness of the epidermis and demonstrate mitotic activity, pleomorphism, and enlarged nuclei. In some cases, hair follicle involvement is observed. The upper epidermis cells might undergo vacuolization and show an abundant and strongly eosinophilic cytoplasm (see Image. Squamous Cell Carcinoma in Situ, Bowen Disease).[6][7][8]
History and Physical
Usually, squamous cell carcinoma in situ (SCCIS) affects sun-exposed areas on the skin of the head and neck, and there are also cases of it arising on the trunk. In the early stages of Bowen disease, virus lesions appear on the skin in the form of red, scaly patches, and as it progresses, it develops into nodules or plagues which are prone to ulceration.
Evaluation
Biopsy
The gold standard of diagnosis for carcinoma in situ is a skin biopsy; a shave or punch biopsy can be used. Biopsy samples should be taken from the suspected carcinoma in situ and its surrounding tissues and then sent to a dermatopathologist for adequate pathologic analysis.
Skin Examination
A complete skin examination is mandatory for patients with suspected squamous cell carcinoma in situ. The examination should be on both sun-exposed and non-exposed areas.
Treatment / Management
Histological mapping and local excision of the carcinoma is the standard form of treatment. Other treatment options prescribed by dermatologists for early lesions include the use of topical creams like imiquimod or 5-fluorouracil; these two drugs are topical immune response modifier, and topical antineoplastic agent respectively. X-ray or Grenz-ray radiation therapy also can be applied for patients with multiple lesions. Photodynamic therapy is another treatment option that has shown great success in the management of squamous cell carcinoma in situ (SCCIS) involves injecting a photosensitizing agent which is absorbed by the tumor. A light source is then used to stimulate the injected agent, and this triggers tumor destruction.[9][10][11](B2)
Differential Diagnosis
The symptoms of squamous cell carcinoma in situ are similar to those of other diseases or conditions, so it is important not to mistake its symptoms. Diseases that should be differentiated and ruled out to reach a conclusive diagnosis of squamous cell carcinoma in situ include atopic dermatitis, pyoderma gangrenosum, Bowenoid papulosis, atypical fibroxanthoma, melanoma in situ, and Paget disease.
Prognosis
The risk rate of the disease progressing to full, invasive squamous cell carcinoma is minimal and around 3% to 5%. A study of previous cases with mutually probable biases reported that of the 3% to 5% develop to invasive squamous cell carcinoma one-third could metastasize. For erythroplasia of Queyrat or genital Bowen disease, the risks are estimated to be higher. After surgical excision, if negative margins are not achieved, there is a risk of recurrence.
Pearls and Other Issues
In its early stages, it can be misdiagnosed as eczema, psoriasis, or even ringworm. It may develop into an invasive cancer if it is not treated early. The most common cause of squamous cell carcinoma in situ is undue exposure to the sun’s rays; therefore, in preventing one’s susceptibility to the disease, there should be a limit to sun exposure. The use of sunscreen, photoprotective clothing, and other means that could minimize exposure to sun rays are helpful prevention tips. Regular testing and screening are also important, especially in people at high risk for squamous cell carcinoma in situ. Early detection has a very good prognosis and prevents the development of squamous cell carcinoma.
Enhancing Healthcare Team Outcomes
Patients with skin lesions often present to the emergency department, primary care physician, nurse practitioner or the internist. However, if there is suspicion about cancer the patient is best referred to a dermatologist. Without a biopsy, it is impossible to make the diagnosis of early skin cancer. While the dermatologist will undertake definitive workup, the primary care provider, nurse practitioner and pharmacist should emphasize the importance of prevention by limiting sun exposure.
The use of sunscreen, photoprotective clothing, and other means that could minimize exposure to sun rays are helpful prevention tips. Regular testing and screening are also important, especially in people at high risk for squamous cell carcinoma in situ. Early detection has a very good prognosis and prevents the development of squamous cell carcinoma.[12]
Media
(Click Image to Enlarge)

(Click Image to Enlarge)
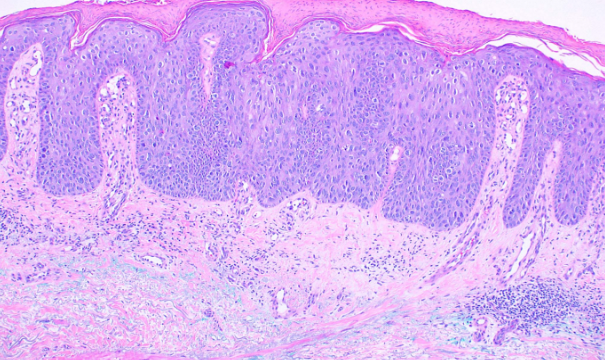
Squamous Cell Carcinoma in Situ, Bowen Disease
Contributed by Dipti Anand, MD
References
Scalvenzi M, Villani A, Mazzella C, Fabbrocini G, Costa C. Cutaneous Bowen's Disease: an Analysis of 182 Cases according To Age, Sex, and Anatomical Site from an Italian Center. Open access Macedonian journal of medical sciences. 2019 Feb 28:7(4):696-697. doi: 10.3889/oamjms.2019.123. Epub 2019 Feb 20 [PubMed PMID: 30894936]
Level 3 (low-level) evidenceFernández-Sánchez M, Charli-Joseph Y, Domínguez-Cherit J, Guzman-Herrera S, Reyes-Terán G. Acral and Multicentric Pigmented Bowen's Disease in HIV-Positive Patients: Report on Two Unusual Cases. Indian journal of dermatology. 2018 Nov-Dec:63(6):506-508. doi: 10.4103/ijd.IJD_47_17. Epub [PubMed PMID: 30504981]
Level 3 (low-level) evidenceWozniak-Rito AM, Rudnicka L. Bowen's Disease in Dermoscopy. Acta dermatovenerologica Croatica : ADC. 2018 Jun:26(2):157-161 [PubMed PMID: 29989873]
Jiyad Z, O'Rourke P, Soyer HP, Green AC. Clinical comparison of actinic changes preceding squamous cell carcinoma vs. intraepidermal carcinoma in renal transplant recipients. Clinical and experimental dermatology. 2017 Dec:42(8):895-897. doi: 10.1111/ced.13211. Epub 2017 Sep 19 [PubMed PMID: 28925042]
Fernandez Figueras MT. From actinic keratosis to squamous cell carcinoma: pathophysiology revisited. Journal of the European Academy of Dermatology and Venereology : JEADV. 2017 Mar:31 Suppl 2():5-7. doi: 10.1111/jdv.14151. Epub [PubMed PMID: 28263020]
Elbendary A, Xue R, Valdebran M, Torres KMT, Parikh K, Elattar I, Kwon EJ, Elston DM. Diagnostic Criteria in Intraepithelial Pagetoid Neoplasms: A Histopathologic Study and Evaluation of Select Features in Paget Disease, Bowen Disease, and Melanoma In Situ. The American Journal of dermatopathology. 2017 Jun:39(6):419-427. doi: 10.1097/DAD.0000000000000704. Epub [PubMed PMID: 28525420]
Majores M, Bierhoff E. [Actinic keratosis, Bowen's disease, keratoacanthoma and squamous cell carcinoma of the skin]. Der Pathologe. 2015 Feb:36(1):16-29. doi: 10.1007/s00292-014-2063-3. Epub [PubMed PMID: 25663185]
Zalaudek I, Argenziano G. Dermoscopy of actinic keratosis, intraepidermal carcinoma and squamous cell carcinoma. Current problems in dermatology. 2015:46():70-6. doi: 10.1159/000366539. Epub 2014 Dec 18 [PubMed PMID: 25561209]
Lazarevic D, Ramelyte E, Dummer R, Imhof L. Radiotherapy in Periocular Cutaneous Malignancies: A Retrospective Study. Dermatology (Basel, Switzerland). 2019:235(3):234-239. doi: 10.1159/000496539. Epub 2019 Apr 2 [PubMed PMID: 30939473]
Level 2 (mid-level) evidenceShimizu A, Kuriyama Y, Hasegawa M, Tamura A, Ishikawa O. Nail squamous cell carcinoma: A hidden high-risk human papillomavirus reservoir for sexually transmitted infections. Journal of the American Academy of Dermatology. 2019 Dec:81(6):1358-1370. doi: 10.1016/j.jaad.2019.03.070. Epub 2019 Mar 29 [PubMed PMID: 30930083]
Thorsness SL, Freites-Martinez A, Marchetti MA, Navarrete-Dechent C, Lacouture ME, Tonorezos ES. Nonmelanoma Skin Cancer in Childhood and Young Adult Cancer Survivors Previously Treated With Radiotherapy. Journal of the National Comprehensive Cancer Network : JNCCN. 2019 Mar 1:17(3):237-243. doi: 10.6004/jnccn.2018.7096. Epub [PubMed PMID: 30865918]
Zink A. [Non-melanoma skin cancer : Pathogenesis, prevalence and prevention]. Der Hautarzt; Zeitschrift fur Dermatologie, Venerologie, und verwandte Gebiete. 2017 Nov:68(11):919-928. doi: 10.1007/s00105-017-4058-5. Epub [PubMed PMID: 29018888]