Introduction
The sphenoid is just one of the twenty-two bones that form the skull and essentially helps to connect the neurocranium to the facial skeleton. It is a single bone in the midline of the cranial cavity situated posterior to the frontal bone but anterior to the occipital. Its name derives from the Greek 'sphenoeides,' which means wedge-shaped. It has several foramina and fissures present in its surface that allow the entry and exit of nerves and blood vessels to and from the cranial cavity. Shaped like a butterfly or a bat, it has a central body and two lateral wings on either side. It is one of the bones that make up the orbit, in particular, forming the posterior surface. The articulations of the sphenoid are with the frontal, parietal, ethmoid, zygomatic, temporal, occipital, palatine, and vomer bones. There may be several morphological variations in the relationship between the sphenoid, the ethmoid, and the frontal bone. Together, these give rigidity and stability to the skull making it the ideal place to house the brain.[1][2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Structure
The sphenoid broadly divides into the central body, the greater wings, the lesser wings, and the pterygoid process. The body of the sphenoid is the medial part of the bone, in between the two lateral greater wings. It contains a depression called the sella turcica, which has a central depression for the pituitary gland. The body also houses the sphenoidal sinuses. The two lesser wings of the sphenoid are present anterior to the body and are triangular. The two greater wings of the sphenoid are also triangular in shape and are lateral to the body. The pterygoid process is directed downwards and made up of two laminae.[3][4]
Ligaments
The sphenoid bone has several intrinsic ligaments, which may occasionally ossify. These are the pterygospinous, the interclinoid, and the caroticoclinoid ligaments.[5]
Openings
This cranial bone has several openings to allow the entry and exit of several nerves and blood vessels to move in and out of the cranial cavity. These include the optic canal, the superior orbital fissure, the foramen rotundum, the foramen lacerum, the foramen spinosum, and the foramen ovale. The foramen lacerum is between the sphenoid, the basilar part of the occipital, and the apex of the temporal bone and often contains connective tissue.[6]
Function
Sphenoid bone has many essential functions. It helps form the base and lateral sides of the skull in combination with the orbital floor. Its many articulations with other bones give the skull rigidity. It is an attachment site for many of the muscles of mastication. A portion of the sphenoid forms the facial skeleton. Also, several fissures and foramina exist in the sphenoid, which transports several blood vessels and nerves of the skull to the head and neck. The body of the sphenoid has a cavity with a sinus that communicates with the nasal cavity. These sphenoidal sinuses work to make the skull lightweight and to increase resonance.
Embryology
The sphenoid bone is a complicated structure in terms of its embryologic origin. This bone forms by the joining together of different primordia whose embryonic origins are dissimilar. The sphenoid bone has two distinct components. The cephalic mesoderm forms the basi-post-sphenoid and the orbitosphenoid, whereas the basi-pre-sphenoid and the alisphenoid have a neural crest cell origin. Several developmental diseases have links to the sphenoid bone, such as chordomas and trans-sphenoidal encephaloceles caused by the persistence of the craniopharyngeal canal. The first centers of ossification of the sphenoid appear in the eighth week of fetal life. These alae arise from the lateral walls of the skull. Later, the basisphenoid nuclei appear on the floor of the pituitary fossa while the lingulae appear between these two.[7]
Blood Supply and Lymphatics
The blood vessels pass through the foramina present in the wings of the sphenoid bone. The ophthalmic artery passes through the optic canal to enter the orbit. The ophthalmic veins pass out of the orbit through the superior orbital fissure. The accessory meningeal artery passes through the foramen ovale to enter the skull. The foramen spinosum allows passage for the middle meningeal artery and vein. Only some small meningeal arterial branches and veins pass through the foramen lacerum, though cartilage may close it off.
Nerves
Several nerves pass through the foramina, fissures, and canal in the sphenoid bone. The optic canal allows passage to the optic nerve (CN II). The superior orbital fissure transmits the superior and inferior divisions of the oculomotor nerve (CN III), the trochlear nerve (CN IV), the ophthalmic nerve (CN V1), the abducens nerve (CN VI), and the sympathetic fibers from the cavernous plexus. The foramen rotundum contains the maxillary division of the trigeminal nerve (CN V2). The foramen ovale allows passage to the mandibular division of the trigeminal nerve (CN V3), the motor root of the trigeminal nerve, and the lesser petrosal nerve. The mandibular nerve's meningeal branch passes through the foramen spinosum.[8]
Muscles
The temporalis muscle, which serves as one of the muscles of mastication, is attached to the temporal surface of the greater wing of the sphenoid. The upper fibers of the lateral pterygoid muscle attach to the infratemporal surface of the greater wing of the sphenoid as well as the infratemporal crest. The lateral pterygoid muscle attaches to the lateral aspect of the lateral plate of the pterygoid process while the medial pterygoid muscle is attached to the medial aspect of the lateral plate as well as the pterygoid fossa. The medial division of the pterygoid process, called the medial plate, serves as a site of attachment to the superior pharyngeal constrictor muscle.[9]
Surgical Considerations
Trans-sphenoidal surgery is the therapeutic choice in cases of pituitary tumors that require surgical removal. It involves accessing the pituitary gland by passing surgical instruments through the nose and sphenoidal sinuses to reach the sella turcica. This trans-sphenoidal approach may also be an access method to perform surgeries on other structures apart from the pituitary, like in the case of a craniopharyngioma.
Clinical Significance
Sphenoid Sinusitis:
The sphenoid sinuses can become infected, resulting in acute and chronic sinusitis. It is relatively uncommon for the sphenoid sinuses to be involved in isolation, usually occurring along with frontal and ethmoidal sinusitis. Symptoms will include fever, weakness, and a post-nasal drip. If not treated promptly, it can result in such devastating complications as meningitis, brain abscess, and involvement of cranial nerves.[10]
Sphenoid Fractures:
Fractures of the sphenoid occur in cases of trauma to the orbit or the base of the skull. These fractures may present with multiple neurological sequelae as the sphenoid is closely associated with numerous nerves that pass through it. Loss of vision and ocular damage is closely related to these fractures. Signs and symptoms include Battle sign, hemotympanum, and cranial nerve palsies, among others.
Sphenoid wing dysplasia:
Sphenoid wing dysplasia in patients with neurofibromatosis type 1 may result in challenging and significant changes, including, ultimately, vision loss.[11]
Media
(Click Image to Enlarge)
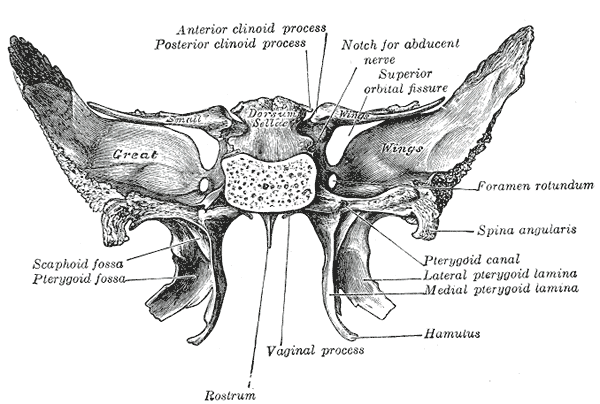
The Sphenoid bone; Upper and posterior surfaces
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Luibil N, Lopez MJ, Patel BC. Anatomy, Head and Neck, Orbit. StatPearls. 2023 Jan:(): [PubMed PMID: 30969665]
Kasai E, Kondo S, Kasai K. Morphological variation in the anterior cranial fossa. Clinical and experimental dental research. 2019 Apr:5(2):136-144. doi: 10.1002/cre2.163. Epub 2019 Jan 31 [PubMed PMID: 31049216]
Laleva L, Spiriev T, Dallan I, Prats-Galino A, Catapano G, Nakov V, de Notaris M. Pure Endoscopic Lateral Orbitotomy Approach to the Cavernous Sinus, Posterior, and Infratemporal Fossae: Anatomic Study. Journal of neurological surgery. Part B, Skull base. 2019 Jun:80(3):295-305. doi: 10.1055/s-0038-1669937. Epub 2018 Sep 6 [PubMed PMID: 31143574]
Kandyba DV, Babichev KN, Stanishevskiy AV, Abramyan AA, Svistov DV. Dural arteriovenous fistula in the sphenoid bone lesser wing region: Endovascular adjuvant techniques of treatment and literature review. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2018 Oct:24(5):559-566. doi: 10.1177/1591019918777233. Epub 2018 May 31 [PubMed PMID: 29848145]
Natsis K, Piagkou M, Lazaridis N, Totlis T, Anastasopoulos N, Constantinidis J. Incidence and morphometry of sellar bridges and related foramina in dry skulls: Their significance in middle cranial fossa surgery. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2018 Apr:46(4):635-644. doi: 10.1016/j.jcms.2018.01.008. Epub 2018 Feb 10 [PubMed PMID: 29534911]
De Rosa A, Pineda J, Cavallo LM, Di Somma A, Romano A, Topczewski TE, Somma T, Solari D, Enseñat J, Cappabianca P, Prats-Galino A. Endoscopic endo- and extra-orbital corridors for spheno-orbital region: anatomic study with illustrative case. Acta neurochirurgica. 2019 Aug:161(8):1633-1646. doi: 10.1007/s00701-019-03939-9. Epub 2019 Jun 7 [PubMed PMID: 31175456]
Level 3 (low-level) evidenceYamamoto M, Ho Cho K, Murakami G, Abe S, Rodríguez-Vázquez JF. Early Fetal Development of the Otic and Pterygopalatine Ganglia with Special Reference to the Topographical Relationship with the Developing Sphenoid Bone. Anatomical record (Hoboken, N.J. : 2007). 2018 Aug:301(8):1442-1453. doi: 10.1002/ar.23833. Epub 2018 May 4 [PubMed PMID: 29669195]
Bazroon AA, Singh P. Anatomy, Head and Neck: Foramen Lacerum. StatPearls. 2023 Jan:(): [PubMed PMID: 31082070]
Antonopoulou M, Iatrou I, Paraschos A, Anagnostopoulou S. Variations of the attachment of the superior head of human lateral pterygoid muscle. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2013 Sep:41(6):e91-7. doi: 10.1016/j.jcms.2012.11.021. Epub 2012 Dec 20 [PubMed PMID: 23265808]
Dolapsakis C, Kranidioti E, Katsila S, Samarkos M. Cavernous sinus thrombosis due to ipsilateral sphenoid sinusitis. BMJ case reports. 2019 Jan 29:12(1):. doi: 10.1136/bcr-2018-227302. Epub 2019 Jan 29 [PubMed PMID: 30700458]
Level 3 (low-level) evidenceNaran S, Swanson JW, Ligh CA, Shubinets V, Taylor JA, Bartlett SP. Sphenoid Dysplasia in Neurofibromatosis: Patterns of Presentation and Outcomes of Treatment. Plastic and reconstructive surgery. 2018 Oct:142(4):518e-526e. doi: 10.1097/PRS.0000000000004779. Epub [PubMed PMID: 30020238]