 Anatomy, Shoulder and Upper Limb, Proximal Radio-Ulnar Joint
Anatomy, Shoulder and Upper Limb, Proximal Radio-Ulnar Joint
Introduction
The proximal radio-ulnar joint (PRUJ) along with the humeroulnar and humeroradial joints form the articulating elements of the elbow.[1] The PRUJ is located in the proximal forearm and coordinates with the distal radio-ulnar joint (DRUJ) to facilitate the pronation and supination motions of the forearm.[2] The PRUJ helps facilitate these movements through static and dynamic stabilizing elements in the form of ligaments and muscles crossing the joint. A complex formation of neurovascular bundles supplies the muscles, bones, and joint capsule. Clinically, the PRUJ can be disrupted either through congenital or acquired (i.e., fractures, dislocations) conditions.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The radial notch of the ulna articulates with the medial side of the radial head to form the PRUJ.[2] Multiple ligaments also stabilize the PRUJ during movement.
The annular ligament attaches anteriorly to the radial notch, courses around the radial head, and attaches posteriorly to the radial notch, stabilizing the joint during rotation.[3] This stabilization allows the PRUJ to work in conjunction with the DRUJ during pronation and supination of the forearm.[4] The annular ligament tightens anteriorly during supination and posteriorly during pronation, due to translation of the radial head during rotation.[2][5]
The lateral collateral ligamentous (LCL) complex consists of the annular ligament in addition to the radial- and ulnar-components of the LCL complex. The LCL complex has contiguous fibers that also insert and become confluent with the annular ligament. The LCL complex originates on the lateral humeral epicondyle near the axis of elbow rotation. The LUCL attaches distally to the supinator crest.[6]
The quadrate ligament limits the rotation of the radial head by attaching the radial neck to the inferior portion of the radial notch. There is also a minimal limitation of supination from the oblique cord, a cord of fibrous tissue that runs from the ulnar tuberosity to just inferior of the bicipital tuberosity.
Embryology
The upper limb bud starts forming 26 days after fertilization and is regulated by the secretion of Shh by the notochord.[7]
The lateral plate mesoderm of the bud forms the components of the joint (bone, cartilage, tendon). The mesenchyme then condenses into a blastema in the limb bud core, and these cells differentiate into chondrocytes and osteoblasts. At 36 days, the chondrification of the upper limb starts proximally. At sites of future joints, chondrification becomes repressed. Research has found that these interzones to express proteins WNT1, WNT14, and GDF5. The proximal radioulnar joint interzone and annular ligament form 51 days after fertilization.[8] The articular cavity begins to form at 56 days after fertilization. The elbow begins to take its adult form during week 11. At week 12, the quadrate ligament and annular ligament become clearly defined.
Blood Supply and Lymphatics
The brachial artery supplies blood to the upper extremity and bifurcates into the radial and ulnar arteries at the proximal cubital fossa.[9] Branches from the brachial, radial, and ulnar arteries form medial, lateral, and posterior arcades around the elbow.[10] Of these arcades, the lateral arcade supplies the proximal radioulnar joint.
The radial and middle collateral arteries, from the profunda brachii artery, anastomose with the radial recurrent artery and the interosseous recurrent artery to form the lateral arcade.[11] The radial and interosseous recurrent arteries perfuse the radial head and neck, whereas the proximal ulna receives blood from the intraosseous branch of the ulnar artery.
The deep lymphatic vessels of the forearm, the radial and ulnar lymphatic vessels (RLV, ULV), drain lymph from deep lymphatic vessels in the palm.[12] As the ULV continues proximally towards the cubital fossa, the anterior interosseous lymphatic vessel, originating from the pronator quadratus, drains into it. Upon entering the cubital fossa, the lymph from the RLV and ULV drains into the cubital lymph nodes and then continues into the brachial lymphatic vessel (BLV). The BLV continues proximally, where it enters into the axillary lymph nodes.
Nerves
As the PRUJ shares a joint capsule with the humeroulnar and humeroradial joints, it also shares their innervations. The innervation of the elbow capsule divides into an anterior and posterior capsule.
A small branch of the musculocutaneous nerve travels through the brachialis muscle to the central portion of the anterior capsule.[13] As the branch goes medially and laterally, there are areas of overlap with the medial and radial nerves, respectively. Before it passes the pronator teres, the median nerve gives off small branches that innervate the medial portion of the anterior capsule. There is also the possibility of a branch arising from the median nerve just proximal to the elbow and traveling down to the anterior capsule. The lateral portion of the anterior capsule receives innervation from the branch of the radial nerve that also innervates the posterior capsule.
The lateral portion of the posterior capsule receives innervation from a branch of the radial nerve as it travels down the lateral head of the triceps. It then travels through the supinator muscle to also innervate the anterior capsule. Joint branches of the ulnar nerve arise just above the cubital tunnel and innervate the medial portion of the posterior capsule around the medial epicondyle and olecranon. Overlapping innervation from the radial and ulnar nerves supply the central portion of the posterior capsule.
Muscles
The primary movements of the PRUJ are pronation and supination, which occur in conjunction with the distal radioulnar joint.
The primary pronators of the forearm are the pronator teres and the pronator quadratus.[5] The pronator teres has a humeral head that originates on the medial epicondyle and an ulnar head that originates on the coronoid process. These heads combine and then insert on the lateral surface of the mid radius. The pronator quadratus attaches to the distal one-fourth of the anterior ulna and the lateral radius. The pronator teres and quadratus are both innervated by the median nerve from levels C6-7 and C8-T1, respectively.
The biceps brachii and supinator muscles are the primary supinators of the forearm. The biceps brachii covers two joints with the long head and short head originating from the supraglenoid tubercle and coracoid process, respectively. The heads then insert onto the anterior capsule and the medial portion of the radial tuberosity through the bicipital aponeurosis and distal biceps tendon, respectively.[14] These attachments allow the biceps to flex the elbow as well as supinate the forearm. The biceps muscle receives innervation from the musculocutaneous nerve from nerve root levels C5-6. The supinator originates from the lateral epicondyle, anterior proximal ulna, RCL, and the annular ligament. It then wraps around the radius and inserts on the dorsolateral proximal radius. It receives innervation from the radial nerve, nerve root level C6.
Clinical Significance
Dislocation of the radial head with a concurrent fracture of the ulna is known as a Monteggia fracture.[15] While these fracture patterns are most common in children between the ages of 4 and 10 years, they can also occur in adults. Traditionally, the ulnar fracture occurs distal to the olecranon, and the dislocation involves the PRUJ as well as the radiocapitellar joint, although olecranon fracture-dislocation and radial head fracture-dislocation variant patterns are also recognized.
Monteggia fractures classify into four types. The injury commonly occurs through forced pronation of the forearm, such as falling on an extended and pronated upper limb.[2] The most common is type I, where the radial head dislocates anteriorly with a diaphyseal fracture of the ulna. Posterior dislocation of the radial head is in the type II category and commonly demonstrate a concurrent radial head fracture. Type II most often occurs in children with a metaphyseal fracture of the ulna and either a lateral or anterolateral radial dislocation. Lastly, an anterior dislocation with a diaphyseal fracture of the ulna and fracture of the proximal one-third of the radius is a type IV. Principle treatment with open reduction and internal fixation (ORIF) can achieve restoration of motion.[2]
Dislocation of the radial head without a concurrent fracture, nursemaid’s elbow, can also occur and is also seen in children.[16] This subluxation of the radial head commonly occurs when the forearm gets pulled in an axial direction, which causes the radial head to sublux outside the annular ligament, with the latter becoming interposed between the radial head and capitellum.[6] In children over five years of age, isolated radial head subluxation becomes much less common as the annular ligament becomes stronger and thicker in its structural integrity.
Classically, pediatric patients will present with the arm held in slight flexion and slight pronation. Reduction techniques include either the supination and hyperflexion maneuver with the thumb reduction force applied over the radial head or the hyperpronation technique. Recurrence is uncommon but can occur, especially in patients younger than three years of age. Immobilization is not necessary for first-time events. If recurrence is noted multiple times within a short period, cast immobilization merits consideration with the arm held in flexion and neutral to slight forearm supination position.
Media
(Click Image to Enlarge)
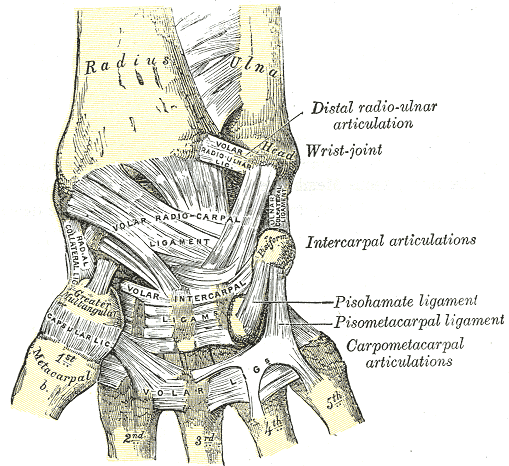
Wrist Ligaments, Anterior View of Radius, Ulna, Distal radio-ulnar articulation, Wrist joint, Volar radioulnar ligament, Volar radiocarpal ligament, Metacarpal, Intercarpal articulations, Pisohamate ligament, pisometacarpal ligament, carpometacarpal articulations, Volar, Greater Trapezium, Capsular ligament, Radial Collateral ligament, Pisiform,
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
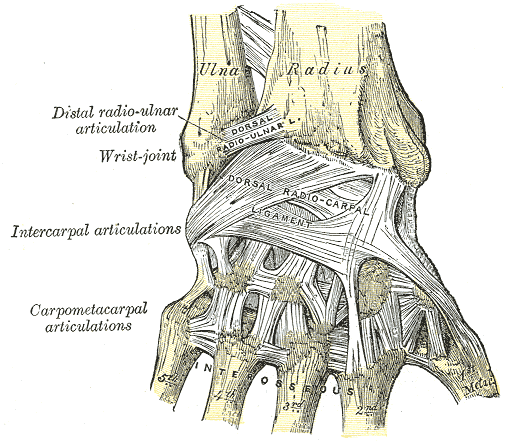
Wrist Ligaments. This posterior-view image shows the anatomic relationships between the ulna, radius, distal radioulnar articulation, wrist joint, intercarpal articulations, carpometacarpal articulations, dorsal radioulnar ligament, dorsal radiocarpal ligament, interossei attachment sites, and metacarpals 1 to 5.
Henry Vandyke Carter, Public domain, via Wikimedia Commons
References
Xiao K, Zhang J, Li T, Dong YL, Weng XS. Anatomy, definition, and treatment of the "terrible triad of the elbow" and contemplation of the rationality of this designation. Orthopaedic surgery. 2015 Feb:7(1):13-8. doi: 10.1111/os.12149. Epub [PubMed PMID: 25708030]
LaStayo PC, Lee MJ. The forearm complex: anatomy, biomechanics and clinical considerations. Journal of hand therapy : official journal of the American Society of Hand Therapists. 2006 Apr-Jun:19(2):137-44 [PubMed PMID: 16713861]
Fliegel BE, Ekblad J, Varacallo M. Anatomy, Shoulder and Upper Limb, Elbow Annular Ligament. StatPearls. 2023 Jan:(): [PubMed PMID: 30860729]
Arias DG, Varacallo M. Anatomy, Shoulder and Upper Limb, Distal Radio-Ulnar Joint. StatPearls. 2023 Jan:(): [PubMed PMID: 31613500]
Stroyan M, Wilk KE. The functional anatomy of the elbow complex. The Journal of orthopaedic and sports physical therapy. 1993 Jun:17(6):279-88 [PubMed PMID: 8343787]
Patel M, Varacallo M. Anatomy, Shoulder and Upper Limb, Forearm Bones. StatPearls. 2023 Jan:(): [PubMed PMID: 31424844]
Al-Qattan MM, Yang Y, Kozin SH. Embryology of the upper limb. The Journal of hand surgery. 2009 Sep:34(7):1340-50. doi: 10.1016/j.jhsa.2009.06.013. Epub [PubMed PMID: 19700076]
Mérida-Velasco JA, Sánchez-Montesinos I, Espín-Ferra J, Mérida-Velasco JR, Rodríguez-Vázquez JF, Jiménez-Collado J. Development of the human elbow joint. The Anatomical record. 2000 Feb 1:258(2):166-75 [PubMed PMID: 10645964]
Yang XH, Wei C, Li GP, Wang JJ, Zhao HT, Shi LT, Cao XY, Zhang YZ. Anatomical study of the anterior neurovascular interval approach to the elbow: observation of the neurovascular interval and relevant branches. Folia morphologica. 2020:79(2):387-394. doi: 10.5603/FM.a2019.0093. Epub 2019 Aug 26 [PubMed PMID: 31448401]
Yamaguchi K, Sweet FA, Bindra R, Morrey BF, Gelberman RH. The extraosseous and intraosseous arterial anatomy of the adult elbow. The Journal of bone and joint surgery. American volume. 1997 Nov:79(11):1653-62 [PubMed PMID: 9384425]
Nagpal P, Maller V, Garg G, Hedgire S, Khandelwal A, Kalva S, Steigner ML, Saboo SS. Upper Extremity Runoff: Pearls and Pitfalls in Computed Tomography Angiography and Magnetic Resonance Angiography. Current problems in diagnostic radiology. 2017 Mar-Apr:46(2):115-129. doi: 10.1067/j.cpradiol.2016.01.002. Epub 2016 Jan 27 [PubMed PMID: 26949062]
Ma CX, Pan WR, Liu ZA, Zeng FQ, Qiu ZQ, Liu MY. Deep lymphatic anatomy of the upper limb: An anatomical study and clinical implications. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2019 May:223():32-42. doi: 10.1016/j.aanat.2019.01.005. Epub 2019 Feb 1 [PubMed PMID: 30716466]
Level 2 (mid-level) evidenceCavalheiro CS, Filho MR, Rozas J, Wey J, de Andrade AM, Caetano EB. Anatomical study on the innervation of the elbow capsule. Revista brasileira de ortopedia. 2015 Nov-Dec:50(6):673-9. doi: 10.1016/j.rboe.2015.10.001. Epub 2015 Oct 19 [PubMed PMID: 27218079]
Tagliafico AS, Bignotti B, Martinoli C. Elbow US: Anatomy, Variants, and Scanning Technique. Radiology. 2015 Jun:275(3):636-50. doi: 10.1148/radiol.2015141950. Epub [PubMed PMID: 25997130]
Adams JE. Forearm Instability: Anatomy, Biomechanics, and Treatment Options. The Journal of hand surgery. 2017 Jan:42(1):47-52. doi: 10.1016/j.jhsa.2016.10.017. Epub [PubMed PMID: 28052828]
Webb AL, Slome MC, Walker A, Ganti L. Radial Head Dislocation with Elbow Subluxation in an Adult. Cureus. 2019 Sep 5:11(9):e5570. doi: 10.7759/cureus.5570. Epub 2019 Sep 5 [PubMed PMID: 31695989]