 Anatomy, Shoulder and Upper Limb, Distal Radio-Ulnar Joint
Anatomy, Shoulder and Upper Limb, Distal Radio-Ulnar Joint
Introduction
The distal radioulnar joint (DRUJ) maintains the integrity of the articulation between the distal radial and ulnar regions (see Image. Wrist Ligaments). This pivot joint is critical to forearm supination, pronation, and anteroposterior translational stability. The DRUJ helps maintain the forearm ring—the region the DRUJ forms with the radius, ulna, and proximal radioulnar joint (PRUJ) essential to forearm movements and is stabilized by the interosseous membrane (IOM), annular ligament, and triangular fibrocartilage complex (TFCC). Pathologies affecting the DRUJ can impact hand, wrist, and elbow function.[1]
The DRUJ is susceptible to acute injuries and chronic posttraumatic degeneration. Conditions affecting this joint can cause significant wrist pain, dysfunction, degeneration, and instability. Understanding this structure's anatomy, function, and clinical importance is crucial to managing upper limb disorders.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Osteology
The distal ulna bears the ulnar styloid process and head, separated by a depression called the "fovea." The disc-like ulnar head articulates with the radial bone's sigmoid (ulnar) notch. The styloid process is an attachment site for the radioulnar ligaments (RULs) (see Image. Forearm Bone Markings).[2] The fovea, the sulcus for the extensor carpi ulnaris (ECU) tendon, the styloid process, and the cartilage surface define the shape of the distal ulna.
An anatomical study demonstrated that the length of the sigmoid notch increased from volar to dorsal. Ulnar length varied significantly and showed a negative correlation with the midcoronal length of the sigmoid notch. The study also identified a correlation between DRUJ obliquity and ulnar variance, a measure of the relative length disparity between the radius and ulna.[3] Patients with typical negative ulnar variance, where the ulna is shorter than the radius, had a sigmoid notch angled in a proximal-ulnar direction. This angle decreased and, in some cases, reversed as ulnar variance became more positive or when the ulna extended beyond the radius.
Although substantial variability existed between specimens, each displayed consistent bilateral anatomy. This finding supports comparing extremities within the same individual but warrants caution when comparing different individuals.[4]
Distal Radioulnar Joint Anatomy and Function
The DRUJ is an incongruent synovial, diarthrodial articulation between the distal radius and ulna, crucial for forearm pronation and supination. The DRUJ's normal motion range is 150° to 180°, with an additional 30° through the radiocarpal joint. DRUJ motion is primarily rotational but includes axial and translational components.
Typically, 80% of the force at the wrist is transmitted through the radius, with the remainder transmitted through the ulna. This amount varies with ulnar and radial deviation. Extreme pronation and supination may result in minimal articular contact, affecting less than 10% of the joint surface area.
Approximately 20% of the DRUJ's stability comes from its bony architecture, with the remainder provided by the surrounding soft tissues. The restraints to the joint's movement come from the TFCC, joint capsule, IOM, and musculotendinous units like the pronator quadratus and ECU.[5]
Triangular Fibrocartilage Complex
The TFCC is the DRUJ's main passive stabilizer (see Image. Triangular Fibrocartilage Complex).[6] This ligamentous complex is comprised of the articular disc, volar and dorsal RULs, the ulnocarpal ligaments, the ulnar collateral ligament (UCL), the ECU tendon sheath, the capsule, and the meniscus homologue.[7]
The TFCC has superficial and deep components. The superficial portion connects with the UCL. The deep segment, known as the triangular ligament or ligamentum subcruentum, attaches to the ulnar fovea via volar and dorsal limbs, forming the volar and dorsal distal RULs. Previous anatomical and biomechanical research suggests that the TFCC's deep component contributes more significantly to DRUJ stability than its superficial counterpart.[8] TFCC disruption can produce ulnar variance alterations, evident on an axial-loaded wrist radiograph.[9]
The TFCC primarily extends the articular surface from the distal radius to the ulnar head, transmitting axial force across the ulnocarpal joint. This complex fibrous structure serves as a robust yet flexible connection between the distal radius and ulna, supporting the ulnar carpal region.
Articular disc
The triangular-shaped articular disc (triangular fibrocartilage proper or TFC proper) is a peripherally thickened fibrocartilaginous structure arising from the cartilage, covering the distal radius and inserting onto the fovea. Fibrous tissues connect the articular disc to the ECU tendon subsheath. The disc is surrounded by the palmar and dorsal radioulnar ligaments.[10] The articular disc is divided into the proximal and distal laminae at its ulnar side by the triangular ligament.[11] The TFC proper functions as a static stabilizer of the DRUJ.[12]
Radioulnar ligaments
The volar and dorsal RULs are proximal condensations of the TFCC that contribute the most to DRUJ stabilization. Superficial RULs connect with the ulnar styloid process, while deep RULs attach to the fovea's articular surface. The deep dorsal and superficial volar fibers resist the ulna's dorsal subluxation during maximum supination, while the deep volar and superficial dorsal fibers become taut during pronation, providing stability to the DRUJ.[13] The RULs support the DRUJ under dynamic loading, while the articular disc separates the DRUJ from the wrist joint cavity.[14]
The RULs significantly contribute to DRUJ stabilization. Evidence suggests that the dorsal RUL tightens while the volar RUL relaxes during pronation. The reverse happens during supination.[15] Several studies also found that the dorsal RUL is crucial for dorsal translational stability during pronation, while the volar RUL is important for volar translational stability during supination. Ward et al's biomechanical study showed that RUL disruption increased the rotational range of motion, underscoring these ligaments' importance in DRUJ rotational stability.[16]
Ulnocarpal ligaments
The ulnocarpal ligament complex consists of the ulnocapitate, ulnolunate, and ulnotriquetral ligaments. These fibrous structures are macroscopically confluent and indistinguishable without joint fluid or contrast material. The volar fibers of the ulnolunate and ulnotriquetral ligaments arise from the volar radioulnar ligament at the fovea and ulnar styloid base and extend distally to insert at the volar lunate and triquetrum. These ligaments are part of the deep extrinsic wrist ligaments contributing to both DRUJ and ulnocarpal stability.
Ulnar Collateral Ligament
The existence of the UCL is highly debated. However, Turker et al's 2019 study using high-resolution ultrasound, dissection, and histologic examination confirmed the anatomic location of this ligament. The UCL arises from the tip of the ulnar styloid process and inserts onto the ulnar aspect of the triquetrum. The UCL occupies the floor of the 6th extensor compartment. This ligament provides static stability to the DRUJ and wrist joint.[17]
Meniscus homologue
The meniscus homologue (ulnocarpal meniscus or ulnomeniscal homologue) is composed of synovial tissue and has 4 compartments: styloid, distal, collateral, and radioulnar, with the styloid being the main component. The meniscus homologue reinforces the medial-sided joint capsule along with the ECU subsheath and UCL, serving as the wrist's "functional ulnar collateral ligament." The meniscus homologue acts as a shock absorber rather than a direct stabilizer.
Joint capsule
The radioulnar joint cavity resembles an "L" shape, enclosed by a fibrous band forming the radioulnar joint capsule. This capsule has a sack-shaped recess to accommodate twisting during pronation. The IOM, joint capsule, and articular disc have recognized roles in stabilizing the DRUJ, particularly during pronation and supination.[18] However, variability exists in how these structures contribute to stability, and their correlation with gross joint instability has not been consistently demonstrated across studies.[19] While biomechanical sectioning sequences include these structures, their specific contributions under different conditions remain a topic of investigation.[20]
Interosseous Membrane
The forearm IOM is the fibrous connective tissue sheet bridging the radius and ulna (see Image. Radioulnar Joints). As mentioned, this membrane stabilizes the forearm ring. This fibrous structure also supports the DRUJ during supination and enhances the forearm's longitudinal stability. The forearm IOM is divided into the central, proximal, and distal bundles.[21] The radial bone's axial stability during proximal radial head fractures depends on both the IOM's central band and the TFCC. DRUJ fracture instability can manifest in various directions: anterior, posterior, or intermediate directional instability.[22]
Embryology
Although extensive embryological research focuses on the TFCC, studies examining other wrist ligaments are scarce. Findings indicate that ligamentous structures begin to develop in O’Rahilly stage 23 embryos and are fully formed by week 14 of gestation. The appearance of the interzone within the condensed mesenchyme marks the initiation of wrist joint formation. The interzone comprises 3 layers, with the intermediate layer considered crucial for wrist ligament formation.[23]
Blood Supply and Lymphatics
The DRUJ's arterial supply primarily derives from the palmar and dorsal branches of the anterior interosseous artery. These arteries branch at the proximal border of the pronator quadratus and form an anastomotic complex around the joint. Other arteries contributing to this network include the posterior (dorsal) interosseous artery connecting to the anterior interosseous artery's dorsal branch, ulnar artery joining the anterior interosseous artery's palmar branch, and collateral vessels from dorsal and palmar carpal arches.[24][25][26]
The lymphatic pathways of the upper extremity have been poorly described, but various routes have been observed, including perforators accessing the wrist compartment. These pathways typically drain from distal to proximal and show little consistency in flow direction, whether from deep to superficial or superficial to deep. Primary lymph nodes in the upper extremity are typically found in the cubital and axillary regions.[27]
Nerves
The DRUJ receives innervation from the anterior interosseous nerve, a median nerve branch, and the posterior interosseous nerve, a radial nerve branch.[28][29][30] These nerves form articular branches that supply the region distal to the proximal border of the pronator quadratus.[31]
Muscles
Muscles around the wrist, hand, and fingers further stabilize the DRUJ. The pronator quadratus is particularly important, as biomechanical analysis shows that this muscle tightens the DRUJ capsule to prevent excessive pouching within the joint during forearm rotation. Both the deep and superficial heads of the pronator quadratus originate from the dorsoulnar aspect of the ulna and attach to the palmar side of the radius. The muscle's orientation prevents capsule interposition and joint diastasis.[32]
Physiologic Variants
As mentioned, ulnar length exhibits greater physiological variability than radial length, leading to significant variability in sigmoid notch shape. This variation should be taken into account when evaluating patients with forearm fractures or wrist pain.
Surgical Considerations
TFCC tears may be treated using either an arthroscopic or an open surgical approach. One repair technique uses the palmaris longus tendon.[33] Surgery is indicated for patients with isolated or associated injuries producing significant DRUJ instability.
DRUJ surgery is contraindicated in patients with other evident pathology, including radial and ulnar length discrepancies, DRUJ arthritis, sigmoid notch incompetence, ECU tendon subluxation, and conditions that cause wrist pain, such as ulnar impaction syndrome. TFCC and DRUJ reconstruction often do not restore stability to the joint. Patients must thus be screened carefully and informed that these procedures are primarily adjunctive for pain management. Various surgical reconstruction procedures exist in the literature, including RUL reconstruction, extrinsic radioulnar tether placement, and radiocarpal sling or tenodesis procedure. These interventions have inherent limitations but have been found to help control symptoms.[34]
Wrist arthroscopy is part of the diagnostic process for pain on the ulnar side of the wrist, which is frequently misdiagnosed as a TFCC injury. Other recommended imaging tools include radiography and magnetic resonance imaging (MRI).[35]
Distal radial fractures can lead to DRUJ instability and TFCC tears. These conditions may be treated with an intramedullary nail.[36] Fractures of the distal radius or radial head may present with acute DRUJ dislocations, ulnocarpal abutment, ECU tendonitis, and ulnotriquetral ligament tears. Distal radial fracture malunion can cause DRUJ instability. Distal radial fractures may be repaired using a fixed-angle volar locking plate.[37]
Ulnar styloid process fractures can complicate distal radial fractures. However, Zyluk et al's study showed that an unrepaired ulnar styloid fracture associated with a distal radial fracture did not affect the outcomes after augmented Kirschner wire fixation.[38]
Clinical Significance
Distal Radioulnar Joint Instability
Acute traumatic injury and chronic degeneration may give rise to DRUJ instability. However, these conditions have distinct treatment considerations. Chronic tears more commonly affect older patients, whereas acute ones typically result from upper extremity trauma, which can occur at any age. Traumatic distal radial and ulnar styloid fractures often contribute to acute DRUJ instability. The clinical significance of these injuries is contentious, with functional outcomes likely more influenced by repairing the radial fracture rather than the ligamentous or ulnar styloid fracture. DRUJ instability evaluation should include a comprehensive history and physical examination alongside the appropriate diagnostic tests.[39]
Subluxation-related ulnar neuropathy syndrome is a possible complication of chronic DRUJ instability. The ulnar nerve may be compressed within the Guyon canal, potentially producing numbness and tingling of the 4th and 5th digits and intrinsic hand muscle weakness in more advanced cases. Evaluation of ulnar neuropathy symptoms should include stressing the DRUJ to verify the condition's etiology.[40]
Diagnosis of distal radioulnar joint instability and triangular fibrocartilage complex tears
DRUJ instability and TFCC tears are often diagnosed clinically. Computed tomography (CT) and MRI may be performed in supination and pronation to help diagnose these conditions. DRUJ instability should be suspected if the distance between the radius and ulna is more than 6 mm on CT. Radiographs are useful for identifying possibly associated lesions, such as ulnar styloid pseudoarthrosis, osteoarthritis, distal radial malunion, ulnocarpal impaction, and ulnocarpal abutment.
Ulnar pain is usually seen in DRUJ instability. A click is appreciated in more severe cases due to a positional dislocation or relocation of the ulnar head.[41] Pain with pronation and supination against resistance may indicate TFCC damage.
Physical maneuvers
Physical maneuvers that can help identify DRUJ instability and TFCC tears include the following, which must be performed on both the affected and unaffected limbs:
- Piano key sign: The examiner dorsally positions the head of the ulna (as if beginning to play the piano) while the forearm is pronated, then applies a volar force on the ulnar head. The test is positive if increased translation is observed.
- Press test: The patient rises from a seated position by pressing their hands on the chair's armrests. The presence of ulnar pain indicates a TFCC tear.
- Grind test: The examiner stabilizes the patient's distal forearm while holding the wrist with the other hand, supinating the limb in ulnar deviation. This action compresses the carpus against the TFCC, eliciting a response.[42]
- Fovea sign: The examiner compresses the interval between the styloid process and the ECU tendon. Tenderness suggests a DRUJ lesion.
- DRUJ ballottement test: The examiner stabilizes the radiocarpal joint with one hand while moving the ulna anteroposteriorly with the other hand. Pain or increased displacement indicates DRUJ instability. The test is conducted in both supination and pronation.
Potential complications and other key diagnostic considerations
DRUJ instability may result in weakness, pain, and degenerative arthritis, often from untreated distal forearm injuries. Tears isolated to the DRUJ, caused by falls onto outstretched hands, may be misdiagnosed as wrist sprains. Inflammatory arthritis can also contribute to DRUJ instability. TFCC disruption may result in ulnocarpal abutment, characterized by significant pain localized to the ulnar head impacted within the ulnar carpus.
Media
(Click Image to Enlarge)
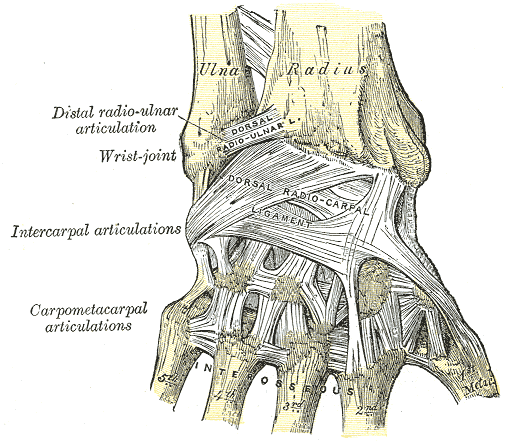
Wrist Ligaments. This posterior-view image shows the anatomic relationships between the ulna, radius, distal radioulnar articulation, wrist joint, intercarpal articulations, carpometacarpal articulations, dorsal radioulnar ligament, dorsal radiocarpal ligament, interossei attachment sites, and metacarpals 1 to 5.
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
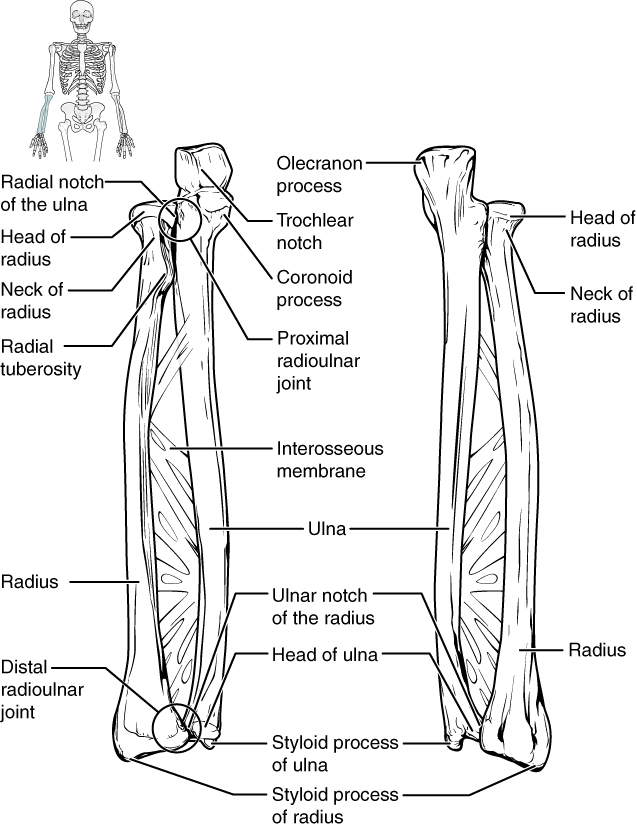
Radioulnar Joints. The radius and ulna connect at various points, including the proximal and distal radioulnar joints and the interosseous membrane.
OpenStax College, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
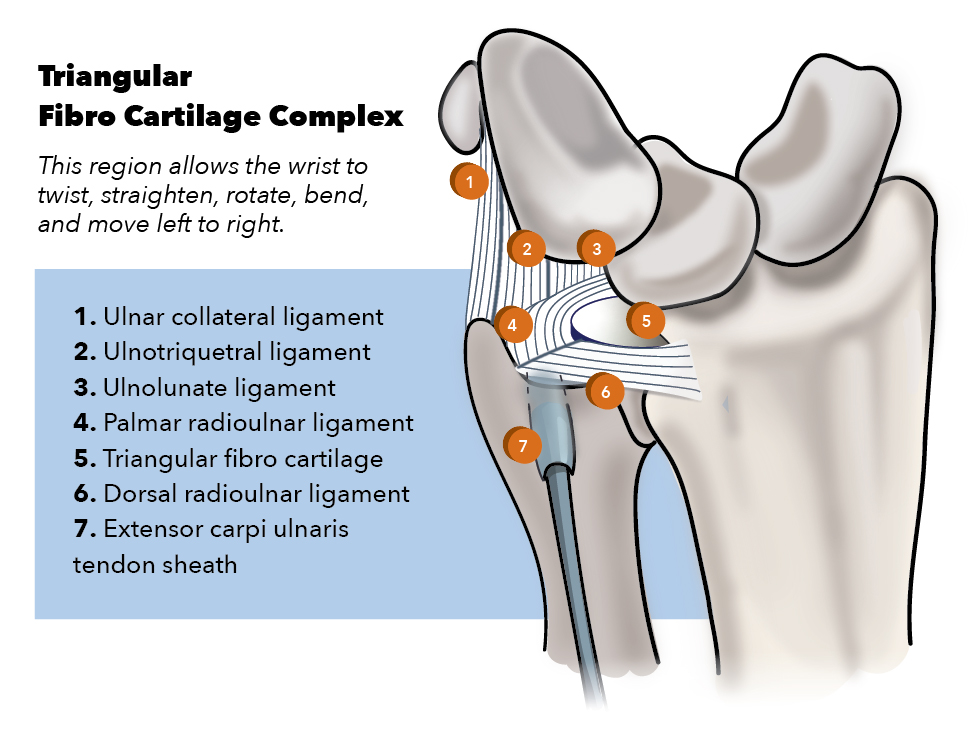
Triangular Fibrocartilage Complex. Parts of the complex include the ulnar collateral ligament, ulnotriquetral ligament, ulnolunate ligament, palmar (volar) and dorsal radioulnar ligaments, triangular fibrocartilage proper (articular disc), and extensor carpi ulnaris tendon sheath.
Contributed by K Humphreys
(Click Image to Enlarge)
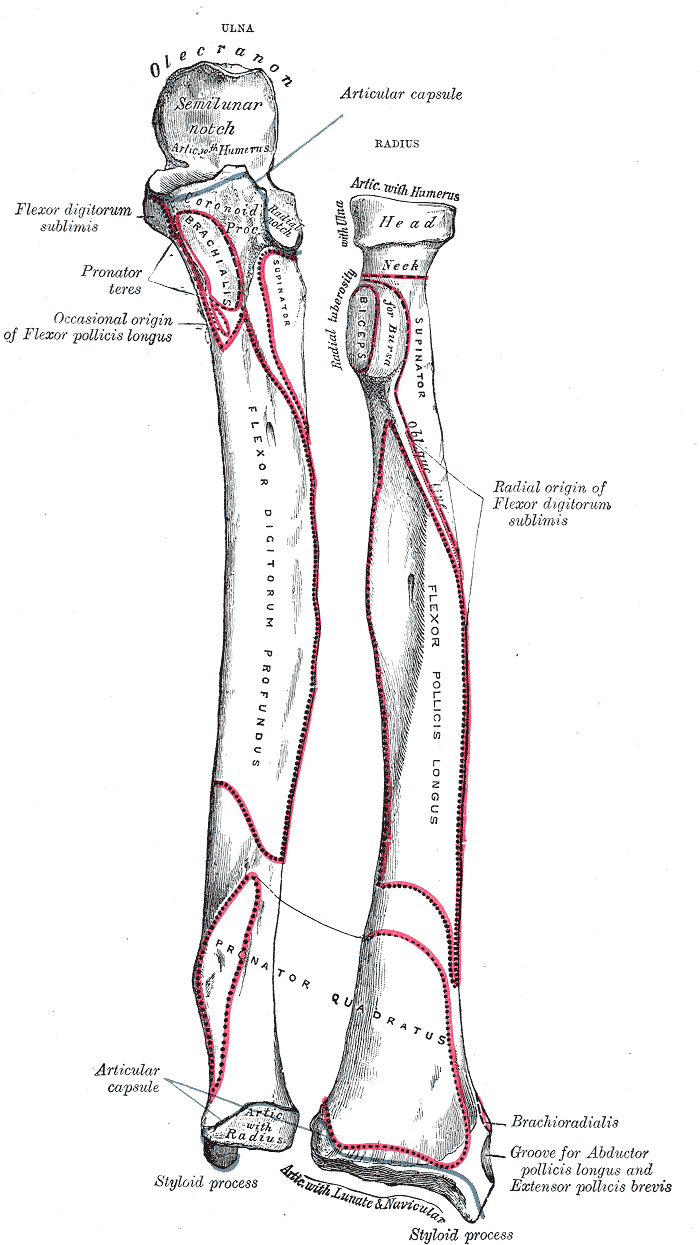
Forearm Bone Markings. Anatomy includes ulna, radius, forearm, articular capsule, olecranon, semilunar notch, flexor digitorum sublimis, flexor, digitorum, pronator teres, brachialis, flexor pollicis longus, pollicis longus, supinator, radial notch, radial tuberosity, biceps, oblique line, flexor digitorum profundus, flexor pollicis longus, radial origin, flexor digitorum sublimis, pronator quadratus, styloid process, brachioradialis, abductor, abductor pollicis longus, and extensor pollicis brevis.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Elzinga K, Chung K. Evolution of the Ring Concept for the Forearm and Its Implication on Treatment: From Galeazzi, Monteggia, Essex-Lopresti, and Darrach to the Current Era. The journal of hand surgery Asian-Pacific volume. 2019 Sep:24(3):251-257. doi: 10.1142/S2424835519300019. Epub [PubMed PMID: 31438785]
Horiuchi S, Nimura A, Tsutsumi M, Suzuki S, Fujita K, Nozaki T, Akita K. Anatomical relationship between the morphology of the styloid process of the ulna and the attachment of the radioulnar ligaments. Journal of anatomy. 2020 Dec:237(6):1032-1039. doi: 10.1111/joa.13275. Epub 2020 Jul 12 [PubMed PMID: 32654121]
Kox LS, Jens S, Lauf K, Smithuis FF, van Rijn RR, Maas M. Well-founded practice or personal preference: a comparison of established techniques for measuring ulnar variance in healthy children and adolescents. European radiology. 2020 Jan:30(1):151-162. doi: 10.1007/s00330-019-06354-x. Epub 2019 Aug 7 [PubMed PMID: 31392482]
Daneshvar P, Willing R, Pahuta M, Grewal R, King GJ. Osseous Anatomy of the Distal Radioulnar Joint: An Assessment Using 3-Dimensional Modeling and Clinical Implications. The Journal of hand surgery. 2016 Nov:41(11):1071-1079. doi: 10.1016/j.jhsa.2016.08.012. Epub 2016 Sep 20 [PubMed PMID: 27663051]
Qazi S, Graham D, Regal S, Tang P, Hammarstedt JE. Distal Radioulnar Joint Instability and Associated Injuries: A Literature Review. Journal of hand and microsurgery. 2021 Jul:13(3):123-131. doi: 10.1055/s-0041-1730886. Epub 2021 Jun 19 [PubMed PMID: 34539128]
Herzberg G, Burnier M, Nakamura T. Arthroscopic Anatomy of the TFCC with Relevance to Function and Pathology. Journal of wrist surgery. 2021 Dec:10(6):558-564. doi: 10.1055/s-0041-1732416. Epub 2021 Jul 26 [PubMed PMID: 34881114]
Yamazaki T, Matsuura Y, Suzuki T, Ohtori S. Measurement of the Material Properties of the Triangular Fibrocartilage Complex. Journal of hand surgery global online. 2020 Mar:2(2):90-93. doi: 10.1016/j.jhsg.2020.01.002. Epub 2020 Feb 25 [PubMed PMID: 35415484]
Liu EH, Suen K, Tham SK, Ek ET. Surgical Repair of Triangular Fibrocartilage Complex Tears: A Systematic Review. Journal of wrist surgery. 2021 Feb:10(1):70-83. doi: 10.1055/s-0040-1718913. Epub 2020 Nov 4 [PubMed PMID: 33552699]
Level 1 (high-level) evidenceZhu AF, Burns G, Siljander B, Waljee JF, Ozer K. The Role of Triangular Fibrocartilage Complex in Axial Stability of the Forearm. Journal of wrist surgery. 2018 Nov:7(5):404-408. doi: 10.1055/s-0038-1666977. Epub 2018 Jul 9 [PubMed PMID: 30349754]
Wu WT, Chang KV, Mezian K, Naňka O, Yang YC, Hsu YC, Hsu PC, Özçakar L. Ulnar Wrist Pain Revisited: Ultrasound Diagnosis and Guided Injection for Triangular Fibrocartilage Complex Injuries. Journal of clinical medicine. 2019 Sep 25:8(10):. doi: 10.3390/jcm8101540. Epub 2019 Sep 25 [PubMed PMID: 31557886]
von Borstel D, Wang M, Small K, Nozaki T, Yoshioka H. High-Resolution 3T MR Imaging of the Triangular Fibrocartilage Complex. Magnetic resonance in medical sciences : MRMS : an official journal of Japan Society of Magnetic Resonance in Medicine. 2017 Jan 10:16(1):3-15. doi: 10.2463/mrms.rev.2016-0011. Epub 2016 Aug 16 [PubMed PMID: 27535592]
Shinohara I, Inui A, Mifune Y, Nishimoto H, Yamaura K, Mukohara S, Yoshikawa T, Kato T, Furukawa T, Hoshino Y, Matsushita T, Kuroda R. Motion Analysis of Triangular Fibrocartilage Complex by Using Ultrasonography Images: Preliminary Analysis. Sensors (Basel, Switzerland). 2022 Jan 4:22(1):. doi: 10.3390/s22010345. Epub 2022 Jan 4 [PubMed PMID: 35009887]
Rodríguez-Merchán EC, Shojaie B, Kachooei AR. Distal Radioulnar Joint Instability: Diagnosis and Treatment. The archives of bone and joint surgery. 2022 Jan:10(1):3-16. doi: 10.22038/ABJS.2021.57194.2833. Epub [PubMed PMID: 35291239]
Haugstvedt JR, Langer MF, Berger RA. Distal radioulnar joint: functional anatomy, including pathomechanics. The Journal of hand surgery, European volume. 2017 May:42(4):338-345. doi: 10.1177/1753193417693170. Epub 2017 Feb 1 [PubMed PMID: 28399788]
Hayami N, Omokawa S, Kira T, Hojo J, Mahakkanukrauh P, Tanaka Y. Biomechanical analysis of simultaneous distal and proximal radio-ulnar joint instability. Clinical biomechanics (Bristol, Avon). 2020 Aug:78():105074. doi: 10.1016/j.clinbiomech.2020.105074. Epub 2020 Jun 7 [PubMed PMID: 32562881]
Ward LD, Ambrose CG, Masson MV, Levaro F. The role of the distal radioulnar ligaments, interosseous membrane, and joint capsule in distal radioulnar joint stability. The Journal of hand surgery. 2000 Mar:25(2):341-51 [PubMed PMID: 10722827]
Türker T, Sheppard JE, Klauser AS, Johnston SS, Amerongen H, Taljanovic MS. The radial and ulnar collateral ligaments of the wrist are true ligaments. Diagnostic and interventional radiology (Ankara, Turkey). 2019 Nov:25(6):473-479. doi: 10.5152/dir.2019.19036. Epub [PubMed PMID: 31650971]
Wijffels M, Brink P, Schipper I. Clinical and non-clinical aspects of distal radioulnar joint instability. The open orthopaedics journal. 2012:6():204-10. doi: 10.2174/1874325001206010204. Epub 2012 May 30 [PubMed PMID: 22675411]
Omokawa S,Iida A,Kawamura K,Nakanishi Y,Shimizu T,Kira T,Onishi T,Hayami N,Tanaka Y, A Biomechanical Perspective on Distal Radioulnar Joint Instability. Journal of wrist surgery. 2017 May; [PubMed PMID: 28428909]
Level 3 (low-level) evidenceDmour A, Tirnovanu SD, Popescu DC, Forna N, Pinteala T, Dmour BA, Savin L, Veliceasa B, Filip A, Carp AC, Sirbu PD, Alexa O. Advancements in Diagnosis and Management of Distal Radioulnar Joint Instability: A Comprehensive Review Including a New Classification for DRUJ Injuries. Journal of personalized medicine. 2024 Sep 5:14(9):. doi: 10.3390/jpm14090943. Epub 2024 Sep 5 [PubMed PMID: 39338197]
Zhang N, Fang JH. Forearm Interosseous Membrane Maintains the Stability of Proximal Radioulnar Joint. Orthopaedic surgery. 2021 Feb:13(1):168-174. doi: 10.1111/os.12859. Epub 2020 Dec 21 [PubMed PMID: 33345369]
Werner FW, LeVasseur MR, Harley BJ, Anderson A. Role of the Interosseous Membrane in Preventing Distal Radioulnar Gapping. Journal of wrist surgery. 2017 May:6(2):97-101. doi: 10.1055/s-0036-1584545. Epub 2016 Jun 20 [PubMed PMID: 28428910]
Hita-Contreras F, Martínez-Amat A, Ortiz R, Caba O, Alvarez P, Prados JC, Lomas-Vega R, Aránega A, Sánchez-Montesinos I, Mérida-Velasco JA. Development and morphogenesis of human wrist joint during embryonic and early fetal period. Journal of anatomy. 2012 Jun:220(6):580-90. doi: 10.1111/j.1469-7580.2012.01496.x. Epub 2012 Mar 19 [PubMed PMID: 22428933]
Mikić Z. The blood supply of the human distal radioulnar joint and the microvasculature of its articular disk. Clinical orthopaedics and related research. 1992 Feb:(275):19-28 [PubMed PMID: 1735212]
Epperson TN, Varacallo MA. Anatomy, Shoulder and Upper Limb, Brachial Artery. StatPearls. 2025 Jan:(): [PubMed PMID: 30725830]
Kong AC, Varacallo MA. Anatomy, Shoulder and Upper Limb, Hand Volar Arch Arteries. StatPearls. 2025 Jan:(): [PubMed PMID: 31430092]
Ma CX, Pan WR, Liu ZA, Zeng FQ, Qiu ZQ, Liu MY. Deep lymphatic anatomy of the upper limb: An anatomical study and clinical implications. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2019 May:223():32-42. doi: 10.1016/j.aanat.2019.01.005. Epub 2019 Feb 1 [PubMed PMID: 30716466]
Level 2 (mid-level) evidenceAkhondi H, Varacallo MA. Anterior Interosseous Syndrome. StatPearls. 2025 Jan:(): [PubMed PMID: 30247831]
Buchanan BK, Maini K, Varacallo MA. Radial Nerve Entrapment. StatPearls. 2025 Jan:(): [PubMed PMID: 28613749]
Gragossian A, Varacallo MA. Radial Nerve Injury. StatPearls. 2025 Jan:(): [PubMed PMID: 30725989]
Hohenberger GM, Maier MJ, Dolcet C, Weiglein AH, Schwarz A, Matzi V. Sensory nerve supply of the distal radio-ulnar joint with regard to wrist denervation. The Journal of hand surgery, European volume. 2017 Jul:42(6):586-591. doi: 10.1177/1753193416677699. Epub 2016 Nov 15 [PubMed PMID: 27852665]
Flores DV, Umpire DF, Rakhra KS, Jibri Z, Belmar GAS. Distal Radioulnar Joint: Normal Anatomy, Imaging of Common Disorders, and Injury Classification. Radiographics : a review publication of the Radiological Society of North America, Inc. 2023 Jan:43(1):e220109. doi: 10.1148/rg.220109. Epub [PubMed PMID: 36399415]
Zyluk A, Piotuch B. Distal radioulnar joint instability: a review of literature. Polish orthopedics and traumatology. 2013 Mar 14:78():77-84 [PubMed PMID: 23493197]
Lawler E, Adams BD. Reconstruction for DRUJ instability. Hand (New York, N.Y.). 2007 Sep:2(3):123-6. doi: 10.1007/s11552-007-9034-6. Epub 2007 Mar 30 [PubMed PMID: 18780072]
Jain DKA, Wahegaonkar AL. Ulnar-Side Wrist Pain Management Guidelines: All That Hurts is Not the TFCC! Indian journal of orthopaedics. 2021 Apr:55(2):310-317. doi: 10.1007/s43465-020-00319-9. Epub 2021 Jan 1 [PubMed PMID: 33927808]
Nishiwaki M, Tazaki K, Ilyas AM. Treatment of Distal Radial Fractures with an Intramedullary Nail. JBJS essential surgical techniques. 2011 Oct:1(3):e14. doi: 10.2106/JBJS.ST.K.00018. Epub 2011 Oct 26 [PubMed PMID: 31321119]
Nishiwaki M, Terasaka Y, Kiyota Y, Inaba N, Koyanagi T, Horiuchi Y. A Prospective Randomized Comparison of Variable-Angle and Fixed-Angle Volar Locking Plating for Intra-Articular Distal Radius Fractures. The Journal of hand surgery. 2021 Jul:46(7):584-593. doi: 10.1016/j.jhsa.2021.03.014. Epub 2021 May 5 [PubMed PMID: 33965295]
Level 1 (high-level) evidenceZyluk A, Mazur A, Puchalski P. A comparison of outcomes after K-wire fixation of distal radius fractures with and without associated ulnar styloid fracture. Handchirurgie, Mikrochirurgie, plastische Chirurgie : Organ der Deutschsprachigen Arbeitsgemeinschaft fur Handchirurgie : Organ der Deutschsprachigen Arbeitsgemeinschaft fur Mikrochirurgie der Peripheren Nerven und Gefasse : Organ der V.... 2014 Feb:46(1):7-11. doi: 10.1055/s-0034-1366997. Epub 2014 Feb 26 [PubMed PMID: 24573824]
Kakar S, Carlsen BT, Moran SL, Berger RA. The management of chronic distal radioulnar instability. Hand clinics. 2010 Nov:26(4):517-28. doi: 10.1016/j.hcl.2010.05.010. Epub [PubMed PMID: 20951901]
Malone PS, Hutchinson CE, Kalson NS, Twining CJ, Terenghi G, Lees VC. Subluxation-related ulnar neuropathy (SUN) syndrome related to distal radioulnar joint instability. The Journal of hand surgery, European volume. 2012 Sep:37(7):652-64. doi: 10.1177/1753193411432707. Epub 2011 Dec 22 [PubMed PMID: 22193951]
Carr LW, Adams B. Chronic Distal Radioulnar Joint Instability. Hand clinics. 2020 Nov:36(4):443-453. doi: 10.1016/j.hcl.2020.07.004. Epub 2020 Sep 2 [PubMed PMID: 33040956]
Casadei K, Kiel J. Triangular Fibrocartilage Complex. StatPearls. 2025 Jan:(): [PubMed PMID: 30725740]