 Anatomy, Abdomen and Pelvis: Female External Genitalia
Anatomy, Abdomen and Pelvis: Female External Genitalia
Introduction
The female external genitalia include structures associated with both the urinary and reproductive systems, collectively known as the vulva (see Image. Female External Genitalia). This illustration shows the anatomic relationships between the clitoris, vulvar vestibule, external urethral orifice, vaginal orifice, hymen, labia majora, and labia minora. The labia minora have been drawn apart. The term "vulva" originates from the Latin word meaning "covering" or "wrapping." When observed externally, the vulva appears covered or wrapped by folds of skin called the "labia majora" and "labia minora," both of which are integral components of the vulva.
The components of the vulva are the mons pubis, labia majora, labia minora, clitoris, urethra, vulva vestibule, vestibular bulbs, Bartholin glands, Skene glands, and vaginal opening. Together, these structures play essential roles in reproduction and urination.[1]
Understanding the vulva's structure and function is essential for diagnosing and treating conditions such as infections, cysts, and vulvar cancers. Precise knowledge of vulvar anatomy is vital for episiotomies, reconstructive surgeries, and trauma management. Additionally, the vulva's role in sexual health, urinary function, and childbirth underscores its importance in medical care and patient education.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
"Vulva" is the global term that describes all of the structures that make the female external genitalia. The components of the vulva are the mons pubis, labia majora, labia minora, clitoris, vestibular bulbs, vulva vestibule, Bartholin glands, Skene glands, urethra, and vaginal opening, which are described below.
Mons Pubis
The mons pubis is a tissue mound made up of fat located directly anterior to the pubic bones. This mound of tissue is prominent in females and is usually covered in pubic hair. The mons pubis functions as a cushion during sexual intercourse. The mons pubis also contains sebaceous glands that secrete pheromones to induce sexual attraction.[2]
Labia Majora
The term "labia majora" means "larger lips." The labia majora are a prominent pair of cutaneous skin folds that form the lateral longitudinal borders of the vulval clefts. The labia majora comprises the folds that cover the labia minora, clitoris, vulva vestibule, vestibular bulbs, Bartholin glands, Skene glands, urethra, and vaginal opening. The anterior folds of the labia majora meet to form the anterior labial commissure, located posterior to the mons pubis when viewed inferiorly. Similarly, the posterior folds of the labia majora converge to form the posterior labial commissure. The labia majora engorge with blood and appear edematous during sexual arousal.
Labia Minora
The term "labia minora" means "smaller lips." The labia minora are a pair of small cutaneous folds that begin at the clitoris and extend posteriorly. The anterior folds of the labia minora encircle the clitoris, forming the clitoral hood and frenulum. The labia minora then proceed obliquely and posteriorly, forming the borders of the vulvar vestibule. The posterior ends of the labia minora terminate as they become linked together by a skin fold, the frenulum of the labia minora. The labia minora encircle the vulvar vestibule, terminating between the labia majora and the vestibule. The labia minora become engorged with blood and appear edematous during sexual arousal.
Clitoris
The clitoris, homologous to the glans penis in male individuals, is a female sex organ with a primarily sensory function. This structure may be divided into the glans clitoris and the clitoral body. The underlying tissue of the clitoris is the corpus cavernosum, a type of erectile tissue that converges and protrudes externally as the glans clitoris. Proximally, the tissue splits to form the crura (or "legs") of the clitoris and the body. The glans clitoris is the only visible portion of this organ and is richly innervated, containing approximately 8,000 nerve endings. The clitoris is also highly vascularized, which causes it to become erect and engorged with blood during sexual arousal and stimulation.
Vestibular Bulbs
The vestibular bulbs, homologous to the bulb of the penis in male individuals, are structures composed of corpus spongiosum tissue, a type of erectile tissue closely related to that of the clitoris. These bulbs are located near the inferior side of the clitoral body and extend toward the urethra and vagina along the medial edges of the crura of the clitoris. The vestibular bulbs eventually split, surrounding the lateral borders of the urethra and vagina. The vestibular bulbs are believed to function closely with the clitoris. During sexual arousal, the vestibular bulbs become engorged with blood, which, in turn, exerts pressure on the corpus cavernosum and the crura of the clitoris. This pressure is thought to contribute to the pleasurable sensations experienced during arousal.
Vulvar Vestibule
The area between the labia minora is known as the vulvar vestibule. This smooth surface extends anteriorly, just posterior to the clitoris, and posteriorly to the posterior commissure of the labia minora. The vulvar vestibule contains the openings of the urethra and vagina. The edges of the labia minora form the borders of the vulvar vestibule. A distinct line, known as the Hart line, marks the boundary between the vulvar vestibule and the labia minora. This demarcation represents the transition from the smoother skin of the vestibule to the more textured appearance of the labia minora.
Bartholin Glands
The Bartholin glands, also known as the greater vestibular glands, are homologous to the bulbourethral glands in male individuals. These pea-sized glands are located slightly lateral and posterior to the vaginal opening. The Bartholin glands secrete a mucus-like substance that lubricates the vagina and the area within the labia minora. This mucus functions to reduce friction during intercourse and acts as a moisturizer for the vulva.
Skene Glands
The Skene glands, also known as the lesser vestibular glands, are homologous to the prostate glands in the male body. This pair of glands is located on either side of the urethra. The Skene glands are believed to secrete a substance that lubricates the urethral opening and may also have antimicrobial properties, helping to prevent urinary tract infections. The exact function of the Skene glands is not fully understood, but they are thought to be the source of female ejaculation during sexual arousal.[3]
Urethra
The urethra is a tube that extends from the bladder to the outside of the body, with the primary function of excreting urine. In female individuals, the urethra opens within the vulvar vestibule, located posterior to the clitoris and anterior to the vaginal opening.
Vagina
The vagina is an elastic, muscular tube that connects to the cervix at its proximal end and extends to the external surface through the vulvar vestibule (see Image. Uterine Tubal Anatomy and Ligaments). The distal opening of the vagina is typically partially covered by a membrane called the "hymen." This opening is located posterior to the urethral opening. The primary functions of the vagina are sexual intercourse and childbirth. During intercourse, the vagina serves as a reservoir for semen, allowing it to collect before sperm cells ascend into the cervix and travel toward the uterus and fallopian tubes. The vagina also functions as an outflow tract for menstrual blood.[4]
Embryology
During the embryonic stage, the fetus begins with undifferentiated gonads, which later develop into either testes or ovaries. The presence of the SRY gene influences the gonads to develop into testes. In the absence of this gene, the gonads default to becoming ovaries. The ovaries are the primary reproductive organs in female individuals, responsible for producing and secreting sex hormones. The theca and granulosa cells within the growing ovarian follicles produce these hormones. The theca interna cells generate androgens, which are then converted into estrogen by the granulosa cells using the enzyme aromatase. Estrogen is the primary hormone influencing the development of the female external genitalia.[5]
The female external genitalia develop from several default structures, including the genital tubercle, urogenital sinus, urogenital folds, and labioscrotal swellings. In the female body, the genital tubercle differentiates into the glans clitoris and the vestibular bulbs. In the male body, the genital tubercle forms the glans penis, corpus cavernosum, and corpus spongiosum. The urogenital sinus develops into the Bartholin and Skene glands, as well as the urethra in female individuals. In male individuals, this sinus forms the bulbourethral glands and the prostate. The labia majora arise from the labioscrotal folds in the female body, whereas they form the scrotum in the male body. The urogenital folds become the labia minora in female individuals and the ventral shaft of the penis in male individuals.
The embryological development of the vagina involves contributions from both the Müllerian ducts and the urogenital sinus, starting around the 6th week of embryogenesis. The Müllerian ducts, which originate from the intermediate mesoderm, form the upper 2/3 of the vagina, along with the uterus and fallopian tubes. Meanwhile, the lower 3rd of the vagina develops from the urogenital sinus, which arises from the endoderm and starts interacting with the Müllerian ducts between the 7th and 8th weeks. The caudal ends of the Müllerian ducts fuse to form the uterovaginal canal, which later becomes the uterus and the vagina's superior portion. At the same time, the vaginal plate—a proliferation of endodermal cells at the junction with the urogenital sinus—forms the template for the vaginal lumen. By the 12th week, the vaginal plate undergoes canalization through programmed cell death, creating the definitive vaginal lumen.
The differentiation of the vagina reflects its dual embryological origin. The upper 2/3 is derived from the Müllerian ducts, while the lower 3rd emerges from the sinovaginal bulbs, with the hymen marking the junction. Proper vaginal development depends on maternal and fetal hormonal influences, particularly estrogen, which aids in the maturation of the vaginal epithelium. Abnormalities such as vaginal agenesis, transverse vaginal septum, and double vagina can result from disruptions in these processes. This dual-origin development highlights the coordinated interaction between mesodermal and endodermal tissues in forming the vagina.[6]
The differentiation of these default structures into female rather than male external genitalia is influenced by estrogen. If these structures were exposed to testosterone, they would develop into male external genitalia.[7]
Blood Supply and Lymphatics
Arterial Supply
The internal pudendal artery perfuses the majority of the external female genitalia. The internal pudendal artery is a branch of the internal iliac artery. Once the pudendal artery branches from the internal iliac artery, it descends toward the external genitalia. The internal pudendal artery then becomes the dominant blood supply to the female external genitalia. The labia majora also receive blood from the superficial external pudendal artery. The superficial external pudendal artery is a tributary of the femoral artery.
Venous Drainage
The external female genitalia drain via the external and internal pudendal veins. The external pudendal vein empties into the great saphenous vein, which drains into the femoral vein. As the femoral vein ascends past the inguinal ligament, it becomes the external iliac vein. The internal pudendal vein, on the other hand, drains into the internal iliac vein. Both the external and internal iliac veins continue to ascend and merge to form the common iliac veins. The common iliac veins from both sides of the body ascend to approximately the level of the 4th lumbar vertebra. At this level, the common iliac veins merge to drain venous blood into the inferior vena cava. The inferior vena cava then ascends toward the heart, where it empties its venous blood into the right atrium.
Lymphatic Circulation
Lymph from the external female genitalia drains into the superficial inguinal lymph nodes, except for the clitoris. Lymph from the clitoris drains into the deep inguinal lymph nodes. Lymph from both the superficial and deep inguinal lymph nodes then ascends toward the common iliac lymph nodes. From there, lymph travels toward the cisterna chyli, a distant part of the thoracic duct. Once at the cisterna chyli, the lymph enters the thoracic duct and ascends toward the angle formed by the left subclavian vein and the left internal jugular vein. Ultimately, all lymph from the external female genitalia returns to the central circulation via the thoracic duct.[8]
Nerves
The motor and sensory innervation of the external female genitalia comes from the pudendal nerve. In contrast, the sympathetic outflow to the female external genitalia originates from the thoracolumbar region of the spinal cord, specifically the T10-to-L2 spinal segments. Preganglionic neurons in the intermediolateral cell column in these segments send axons through the ventral roots to the sympathetic trunk, where they synapse in the inferior mesenteric ganglia or pelvic ganglia of the inferior hypogastric plexus. Postganglionic fibers then travel via the pudendal nerve and branches of the pelvic plexus to innervate structures such as the clitoris, labia, and perineum.
The pudendal nerve originates from the S2, S3, and S4 spinal roots. This nerve enters the pelvis through the lesser sciatic foramen and then travels through the pudendal canal toward the ischial spines. After passing the lesser sciatic foramen, the pudendal nerve encircles the ischial spine and forms branches that innervate the perineum and external genitalia. The nerve branches into 3 main divisions: the dorsal nerve of the clitoris, the perineal nerve, and the inferior rectal nerve.
The dorsal nerve of the clitoris is responsible for the afferent component of clitoral erection. The cavernous tissue of the clitoris is innervated by the cavernous nerves from the uterovaginal plexus. The perineal nerve provides sensory information to the external genitalia via the posterior labial nerves. This nerve also gives off a branch that innervates the external urethral sphincter and motor nerve branches to the muscles of the perineum, which include the bulbospongiosus, ischiocavernosus, levator ani (iliococcygeus, pubococcygeus, and puborectalis), and pubovaginalis muscles.
The inferior rectal nerve supplies innervation to the perianal skin and the external anal sphincter. Additionally, the labia majora receives extra innervation from the anterior labial nerves, which are branches of the ilioinguinal nerve. The mons pubis also receives sensory innervation from the genitofemoral nerve.[9]
Anesthesia of the pudendal nerve during childbirth is common. The ischial spines serve as the landmark for anesthetic injection. The physician palpates the ischial spine from within the vaginal canal, then injects the anesthetic toward the spine to block the sensory territory of the pudendal nerve. This procedure may be performed to reduce pain during childbirth, numb the perineum before an episiotomy, or provide relief for chronic pelvic pain syndromes.[10]
Muscles
Many muscles act on the external female genitalia, forming and supporting the perineum or the pelvic floor. These muscles include the following:
- Bulbospongiosus
- Ischiocavernosus
- Deep transverse perineal muscle
- Superficial transverse perineal muscle
- Levator ani
- Iliococcygeus
- Pubococcygeus
- Puborectalis
- Pubovaginalis
- Coccygeus
- External anal sphincter
- External urethral sphincter
The perineal body is a central fibromuscular structure located in the perineum, serving as an important attachment point for various pelvic floor muscles and connective tissues. This structure supports the pelvic organs and maintains the integrity of the pelvic floor.[11]
Physiologic Variants
The female external genitalia exhibit considerable variation. The shape, size, and color of the mons pubis, clitoris, labia majora, labia minora, and vaginal orifice differ individually. These variations result from the amount of estrogenic influence during development. Higher estrogen levels tend to make these structures larger and thicker, while lower estrogen levels can lead to smaller and thinner external genitalia. For example, the mons pubis, which is heavily influenced by estrogen, appears more prominent in individuals with higher estrogen levels. The labia majora and labia minora show the most variation, with differences in size, color, and length across individuals. Some may have more prominent labial folds, while others may have a larger, more visually prominent clitoris and clitoral hood. Despite these variations, the functionality of these structures remains unchanged.[12]
Variations in the female external genitalia may also result from aging and a decrease in estrogen levels. During menopause, the production of estrogen decreases, leading to atrophy of the female external genitalia.[13][14]
Surgical Considerations
In surgery, understanding the anatomy of the female external genitalia is essential for repairing, reconstructing, and preventing defects. Common procedures involving the female external genitalia include episiotomy, labioplasty, and vaginoplasty.
Episiotomy
An episiotomy involves enlarging the vaginal opening through an incision made either midline or laterally during childbirth to reduce the risk of spontaneous tearing and damage to the vaginal opening. A midline incision targets the perineal body, while a lateral incision targets the transverse perineal muscle. Episiotomies are performed because the surgical site can be easily repaired and generally has a shorter healing time than spontaneous tears that may involve the perineal muscles or the rectum. Repairing a torn vaginal opening following the delivery of a large child typically requires a longer recovery. Episiotomies are performed to facilitate the vaginal delivery of large babies and prevent tearing into surrounding perineal structures.[15][16]
Perineal Tears
Similar to episiotomies, natural tearing of the vagina can occur during childbirth. These tears can range from minor lacerations in the vaginal mucosa to more severe injuries, such as damage extending from the vagina through the rectum. Common causes of these injuries include a 1st childbirth (up to 90% of individuals experience tears during their 1st delivery), uncoordinated contractions and pushing, a large fetal head diameter compared to the vaginal opening, and epidurals.[17][18] Tears are graded from I to IV, as follows:
- Grade I: Tearing of the vaginal mucosa
- Grade II: Vaginal mucosal tear that extends toward the perineal muscles
- Grade III: Vaginal mucosal tear that extends through the perineal muscles and involves the anal sphincter
- Grade IV: Vaginal mucosal tear that extends through the rectal sphincter into the bowel
The severity of these injuries varies, and recognizing them is crucial. A colorectal surgery referral is warranted when the bowels are involved. Close follow-up is essential, as these injuries can lead to complications, such as bowel incontinence, neuropathic pain, and fistula formation.
Labiaplasty
Labiaplasty is a surgical procedure aimed at altering the size and shape of the labia majora and minora. Indications for labiaplasty include congenital disabilities, aging, cancers, and cosmetic concerns. The procedure focuses on achieving a more aesthetically pleasing appearance of the labial folds.[19][20]
Vaginoplasty
Vaginoplasty is a surgical procedure used to reconstruct the vagina or create one. Vaginoplasties are performed for various reasons, including pelvic organ prolapse, congenital disabilities, neoplasms, sex reassignment, and cosmetic purposes. The goal of this procedure is to surgically create a vagina that meets the patient's needs and preferences.[21][22]
Clinical Significance
Understanding the anatomy of the female external genitalia holds critical importance in clinical practice. This knowledge aids in diagnosing various diseases and lesions affecting the genitals and is essential for performing procedures in the vulvar area.
Common Urinary Tract Issues
One common procedure routinely performed in healthcare is the catheterization of the female urethra. This procedure involves the introduction of a flexible tube into the urethra and securing it with a saline-filled balloon. Urethral catheterization helps collect urine from the bladder for excretion and gathering specimens for urine studies, including urine output monitoring and composition analysis.[23]
Meanwhile, one pathology that commonly involves the urethra is urinary tract infection (UTI). Patients with this condition classically complain of painful urination (dysuria), along with changes in urination, such as increased frequency, foul odor, and cloudy appearance. UTI commonly affects female individuals due to their shorter urethrae, which allow bacteria to ascend more easily than in male individuals. The anatomical proximity of the urethra, vagina, and anus also increases the risk of cross-contamination between vaginal and anal bacteria entering the urethra. The primary bacterial etiology of UTIs is gram-negative rods, with Escherichia coli being the most frequent pathogen.[24]
Sexually Transmitted Infections
Infections of the vulvar region can present as rashes or ulcer-like lesions. Haemophilus ducreyi causes chancroid, which is characterized by painful ulcers with irregular, jagged borders and exudative drainage. This condition is often accompanied by inguinal adenopathy or swollen lymph nodes in the groin. Treatment typically involves antibiotics, including 3rd-generation cephalosporins, macrolides, and fluoroquinolones.[25]
Klebsiella granulomatis can cause ulcerative lesions similar to those produced by Haemophilus ducreyi. However, these lesions are painless, have a beefy red appearance, and bleed upon contact. Unlike Haemophilus ducreyi, inguinal adenopathy is absent in this condition. Management of Klebsiella granulomatis infections involves the use of macrolides, tetracyclines, fluoroquinolones, or Bactrim for treatment.
Chlamydia trachomatis infection is a common sexually transmitted condition that is often asymptomatic. However, some individuals may present with cervicitis, urethritis, and vaginal discharge. The most concerning complications in women are pelvic inflammatory disease and perihepatitis. Chlamydia is frequently coinfected with Neisseria gonorrhoeae. Consequently, chlamydia and gonorrhea are often treated together, with tetracyclines or macrolides addressing chlamydia and 3rd-generation cephalosporins combating gonorrhea.[26]
Neisseria gonorrhoeae infection often mirrors chlamydia. This condition is also typically asymptomatic but may also present with urethritis, cervicitis, and creamy, purulent vaginal discharge. Like chlamydia, the primary complications of gonorrhea include pelvic inflammatory disease and perihepatitis. As mentioned, chlamydia and gonorrhea often occur together, so treatment includes a combination of drugs targeting both.
Syphilis is caused by Treponema pallidum and typically presents with a painless chancre in the primary stage. If left untreated, the infection can progress to the secondary stage, which is characterized by fever, widespread maculopapular skin rashes involving the palms and soles, lymphadenopathy (with the epitrochlear node being pathognomonic), and genital lesions resembling genital warts. These genital lesions are known as condylomata lata, which have a rounder surface compared to condylomata acuminata. If still untreated at this stage, the infection can advance to the tertiary stage, which can cause necrotic lesions called "gummas," as well as neurological symptoms that include tabes dorsalis, Argyll-Robertson pupils, and general paresis. Cardiac manifestations of this stage include potentially fatal aortitis. Syphilis is treated with penicillin.
Genital herpes is caused by herpes simplex virus types 1 (HSV 1) and 2 (HSV 2), with the latter being more common in the genital region. HSV 2 infection manifests as painful vesicular lesions that may be accompanied by constitutional symptoms. Although genital herpes is chronic and incurable, antiviral medications like acyclovir can help reduce flare-ups and lower the viral shedding load.
Genital warts, or condylomata acuminata, are cauliflower-like lesions in the genital area caused by the human papillomavirus (HPV). HPV has many strains, with HPV 6 and HPV 11 being primarily responsible for genital warts. A defining feature of these lesions is the presence of koilocytes in histopathology specimens. Genital warts are typically self-limiting and resolve on their own. However, the immune system fails to clear the virus properly in some individuals, leading to chronic genital warts. Infection with high-risk strains, particularly HPV-16 and HPV-18, may lead to cancer in the anogenital area.
Human immunodeficiency virus (HIV) infection is transmitted through unprotected intercourse or exposure to infected blood products. Initially asymptomatic, HIV gradually destroys T-helper lymphocytes. Once the T-helper lymphocyte count drops below 200 cells/mm³, the disease progresses to acquired immunodeficiency syndrome (AIDS). AIDS presents with various opportunistic infections due to profound immune weakness. Although HIV/AIDS has no cure, maintenance medications are available to slow the disease's progression.
Hepatitis is the inflammation of the liver. Hepatitis B and C are viruses that may be transmitted during intercourse. Most individuals remain asymptomatic. The primary concern with these infections is their potential progression to liver cirrhosis and hepatocellular carcinoma. Hepatitis B is preventable through vaccination, but no vaccine exists for hepatitis C. The only preventive measure for hepatitis C infection is using barrier protection during intercourse and avoiding exposure to infected blood products. Treatments are available for both hepatitis B and C, but they only typically slow disease progression. No definitive cure exists for either condition.
Benign Vulvar Pathology
The Bartholin glands produce secretions that lubricate the vulva and vagina. These glands can become obstructed, leading to the formation of a cyst filled with accumulated lubricant. Infection of a Bartholin cyst can lead to an abscess. Bartholin abscesses typically affect female individuals of reproductive age. Bartholin cysts and abscesses present as swelling located posterolaterally to the vaginal orifice. Escherichia coli, Chlamydia trachomatis, and Neisseria gonorrhoeae may cause Bartholin gland infection.
The vulva is sensitive and may be prone to irritation. Chronic irritation associated with lichen sclerosis leads to severe itching. Repeated scratching causes trauma, which, over time, leads to lichenification (thickening) of the vulvar skin. Lichen sclerosus involves thinning of the epidermis and thickening or fibrosis of the dermis, producing white, parchment-like lesions. This condition affects prepubertal and postmenopausal female individuals and increases the risk of vulvar cancer. Treatment typically involves topical steroids.
In lichen simplex chronicus, the vulvar region undergoes epithelial hyperplasia due to chronic scratching and rubbing. This condition makes the vulvar skin thick and leathery, but it is not associated with an increased risk of cancer.
Primary amenorrhea occurs in pubertal girls who reach menarche but do not have menstrual periods. One cause of primary amenorrhea is an imperforate hymen. These female adolescents typically experience monthly pain and pressure in the lower abdomen without observing menstruation. On physical examination, a blue or brown, round, bulging mass may be seen protruding from the vagina. This mass is a collection of menstrual products trapped due to the imperforate hymen. Treatment involves incision and drainage of the mass.[27]
Vulvar Malignancies
Vulvar cancer is rare, with squamous cell carcinoma being the most common type. This malignancy can develop from leukoplakia or an infection with HPV 16 or HPV 18. Lichen sclerosus may also progress to vulvar cancer. A biopsy is required to confirm the diagnosis.[28]
Paget disease of the vulva is typically a form of carcinoma in situ. This condition presents with scaling plaques, crusting, pruritus, ulcers, and erythema. While vulvar Paget disease involves abnormal cell growth, it does not pose an immediate risk of spreading to deeper tissues or becoming invasive.[29]
Other Issues
Since hormones influence the development of the female external genitalia, the vulva may be affected by endocrine-related conditions. The endocrine system regulates hormone secretions, and any defects in this system can lead to atypical genital development. One example is androgen insensitivity syndrome (AIS), where androgen receptors are unresponsive to androgens. Consequently, the external genitalia default to developing as female despite the presence of male chromosomes.[30]
Meanwhile, female individuals may experience virilization if they have excessive blood androgen levels, as seen in congenital adrenal hyperplasia (CAH). In congenital adrenal hyperplasia, a defect in the adrenal production of aldosterone and cortisol causes the precursors of these hormones to be diverted toward androgen production. The excess androgens can masculinize the female external genitalia, resulting in a larger clitoris (clitoromegaly) and fusion of the labia majora, making them appear more scrotal-like.[31]
Media
(Click Image to Enlarge)
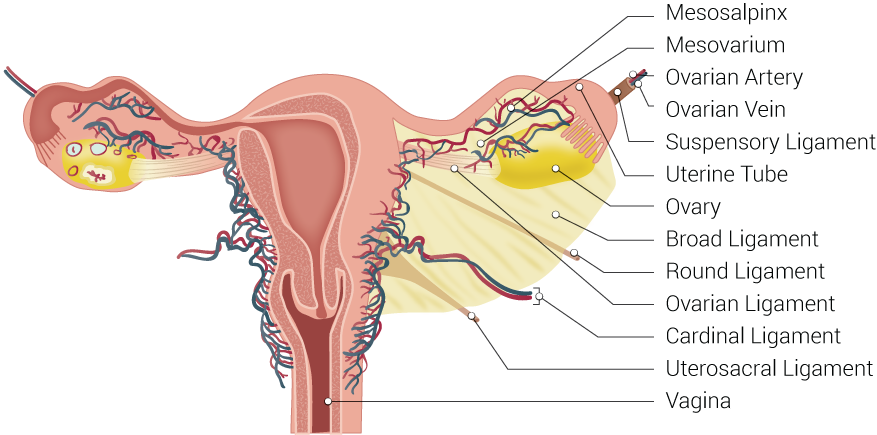
Uterine Tubal Anatomy and Ligaments. Shown in this illustration are anatomical structures surrounding the uterus and fallopian or uterine tubes, including the mesosalpinx, mesovarium, ovarian artery, ovarian vein, suspensory ligament, uterine tube, ovary, broad ligament, round ligament, ovarian ligament, cardinal ligament, uterosacral ligament, and vagina.
Contributed by B Palmer
(Click Image to Enlarge)
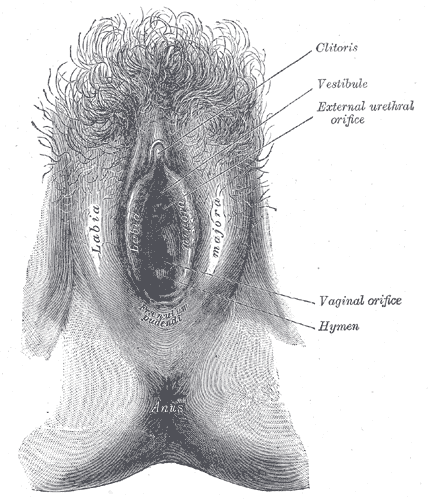
Female External Genitalia. This illustration shows the anatomic relationships between the clitoris, vulvar vestibule, external urethral orifice, vaginal orifice, hymen, labia majora, and labia minora. The labia minora have been drawn apart.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Stelmar J, Zaliznyak M, Sandhu S, Isaacson D, Duralde E, Smith SM, Knudson GA, Garcia MM. Anatomic maps of erogenous and aversive sensation zones of the breasts, vulva, and vagina: a questionnaire-based study. The journal of sexual medicine. 2025 Jan 3:22(1):7-13. doi: 10.1093/jsxmed/qdae143. Epub [PubMed PMID: 39566929]
Seleem M, Osman OM, Kashmar SG, Lotfy R. The effect of cesarean section on the dimensions and ratios of mons pubis. BMC pregnancy and childbirth. 2024 Jul 23:24(1):496. doi: 10.1186/s12884-024-06667-w. Epub 2024 Jul 23 [PubMed PMID: 39044134]
Trikhacheva A, Dengler K, Murdock TA, Gruber D. Vaginal Bulge is not Always Prolapse. Journal of minimally invasive gynecology. 2024 Nov 17:():. pii: S1553-4650(24)01524-3. doi: 10.1016/j.jmig.2024.11.008. Epub 2024 Nov 17 [PubMed PMID: 39551438]
Hoare BS, Khan YS. Anatomy, Abdomen and Pelvis: Female Internal Genitals. StatPearls. 2025 Jan:(): [PubMed PMID: 32119488]
Parker CR Jr, Bruneteau DW, Greenblatt RB, Mahesh VB. Peripheral, ovarian, and adrenal vein steroids in hirsute women: acute effects of human chorionic gonadotropin and adrenocorticotrophic hormone. Fertility and sterility. 1975 Sep:26(9):877-88 [PubMed PMID: 126875]
Etskovitz H, Nandivada P, Hsi Dickie B. Mullerian and vaginal anomalies. Current opinion in pediatrics. 2024 Dec 1:36(6):710-719. doi: 10.1097/MOP.0000000000001409. Epub 2024 Oct 3 [PubMed PMID: 39509255]
Level 3 (low-level) evidenceAsanidze E, Kristesashvili J, Asanidze A, Jibladze A, Gaphrindashvili G, Asanidze B, Bhatia R. Complexities of complete androgen insensitivity syndrome: insights from a case report and literature review. The Journal of international medical research. 2024 Nov:52(11):3000605241300058. doi: 10.1177/03000605241300058. Epub [PubMed PMID: 39600030]
Level 3 (low-level) evidenceCurry SL, Wharton JT, Rutledge F. Positive lymph nodes in vulvar squamous carcinoma. Gynecologic oncology. 1980 Feb:9(1):63-7 [PubMed PMID: 7353802]
Fischerova D, Culcasi C, Gatti E, Ng Z, Burgetova A, Szabó G. Ultrasound assessment of the pelvic sidewall: methodological consensus opinion. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2025 Jan:65(1):94-105. doi: 10.1002/uog.29122. Epub 2024 Nov 5 [PubMed PMID: 39499650]
Level 3 (low-level) evidenceMoir DD, Davidson S. Postpartum complications of forceps delivery performed under epidural and pudenal nerve block. British journal of anaesthesia. 1972 Nov:44(11):1197-9 [PubMed PMID: 4265052]
Leitão ACR, Lira SOR, Viana ESR. Electromyographic parameters for treatment of pelvic floor disorders in pregnant and postpartum women: A review protocol. PloS one. 2024:19(11):e0309822. doi: 10.1371/journal.pone.0309822. Epub 2024 Nov 4 [PubMed PMID: 39495733]
McQuillan SK, Jayasinghe Y, Grover SR. Audit of referrals for concern regarding labial appearance at the Royal Children's Hospital: 2000-2012. Journal of paediatrics and child health. 2018 Apr:54(4):439-442. doi: 10.1111/jpc.13819. Epub 2018 Jan 13 [PubMed PMID: 29330890]
Patni R. Genitourinary Syndrome of Menopause. Journal of mid-life health. 2019 Jul-Sep:10(3):111-113. doi: 10.4103/jmh.JMH_125_19. Epub [PubMed PMID: 31579156]
. . :(): [PubMed PMID: 31576044]
Barjon K, Vadakekut ES, Mahdy H. Episiotomy. StatPearls. 2025 Jan:(): [PubMed PMID: 31536281]
Borrman MJ, Davis D, Porteous A, Lim B. The effects of a severe perineal trauma prevention program in an Australian tertiary hospital: An observational study. Women and birth : journal of the Australian College of Midwives. 2020 Jul:33(4):e371-e376. doi: 10.1016/j.wombi.2019.07.301. Epub 2019 Sep 17 [PubMed PMID: 31537498]
Level 2 (mid-level) evidenceDwan K, Fox T, Lutje V, Lavender T, Mills TA. Perineal techniques during the second stage of labour for reducing perineal trauma and postpartum complications. The Cochrane database of systematic reviews. 2024 Oct 28:10(10):CD016148. doi: 10.1002/14651858.CD016148. Epub 2024 Oct 28 [PubMed PMID: 39465967]
Level 1 (high-level) evidenceHong CX, Fairchild PS, Schmidt PC, Triebwasser JE. Predictors and Unexplained Variability of Obstetric Anal Sphincter Injuries: A Population-Based Cross-Sectional Analysis. International urogynecology journal. 2025 Jan:36(1):87-92. doi: 10.1007/s00192-024-05967-1. Epub 2024 Nov 1 [PubMed PMID: 39485526]
Level 2 (mid-level) evidenceOranges CM, Sisti A, Sisti G. Labia minora reduction techniques: a comprehensive literature review. Aesthetic surgery journal. 2015 May:35(4):419-31. doi: 10.1093/asj/sjv023. Epub [PubMed PMID: 25908699]
Hersant B, Jabbour S, Noel W, Benadiba L, La Padula S, SidAhmed-Mezi M, Meningaud JP. Labia Majora Augmentation Combined With Minimal Labia Minora Resection: A Safe and Global Approach to the External Female Genitalia. Annals of plastic surgery. 2018 Apr:80(4):323-327. doi: 10.1097/SAP.0000000000001435. Epub [PubMed PMID: 29461295]
Acimi S, Bessahraoui M, Acimi MA, Abderrahmane N, Debbous L. Vaginoplasty and creating labia minora in children with disorders of sex development. International urology and nephrology. 2019 Mar:51(3):395-399. doi: 10.1007/s11255-018-2058-8. Epub 2018 Dec 13 [PubMed PMID: 30547360]
Learner HI, Creighton SM, Wood D. Augmentation vaginoplasty with buccal mucosa for the surgical revision of postreconstructive vaginal stenosis: a case series. Journal of pediatric urology. 2019 Aug:15(4):402.e1-402.e7. doi: 10.1016/j.jpurol.2019.05.019. Epub 2019 May 25 [PubMed PMID: 31351946]
Level 2 (mid-level) evidenceDrake MJ, Clavica F, Murphy C, Fader MJ. Innovating Indwelling Catheter Design to Counteract Urinary Tract Infection. European urology focus. 2024 Sep:10(5):713-719. doi: 10.1016/j.euf.2024.09.015. Epub 2024 Sep 28 [PubMed PMID: 39341718]
Patel D. Intravesical Therapies for Recurrent Urinary Tract Infections: A Systematic Review. Cureus. 2024 Oct:16(10):e72175. doi: 10.7759/cureus.72175. Epub 2024 Oct 23 [PubMed PMID: 39507191]
Level 1 (high-level) evidenceAl-Tawfiq JA, Spinola SM. Infections caused by Haemophilus ducreyi: one organism, two stories. Clinical microbiology reviews. 2024 Dec 10:37(4):e0013524. doi: 10.1128/cmr.00135-24. Epub 2024 Sep 17 [PubMed PMID: 39287406]
Tao G, Patel CG, Stanford KA. Low sexually transmitted infection (STI) screening and presumptive treatment and high STI positivity among United States females visiting the emergency department after sexual assault. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2024 Dec 3:():. doi: 10.1111/acem.15058. Epub 2024 Dec 3 [PubMed PMID: 39627651]
Imfeld C, Godfroy M. [Hymenal imperforation]. La Revue du praticien. 2024 Oct:74(8):875 [PubMed PMID: 39439330]
Obermair HM, Elhindi J, Brand A, Herbst U. Vulvar squamous cell carcinoma: The role of p53 and p16 immunohistochemistry. Gynecologic oncology reports. 2024 Dec:56():101544. doi: 10.1016/j.gore.2024.101544. Epub 2024 Nov 8 [PubMed PMID: 39624202]
Nishimura Y, Oki Y, Nonomura D, Matsuzaki K, Nishimura K. [A Case of Secondary Extramammary Paget's Disease Developed at 11 Years after Cystectomy]. Hinyokika kiyo. Acta urologica Japonica. 2024 Oct:70(10):335-341. doi: 10.14989/ActaUrolJap_70_10_335. Epub [PubMed PMID: 39632583]
Level 3 (low-level) evidenceNegussie D. Androgen insensitivity syndrome: a case report. Ethiopian medical journal. 2007 Jul:45(3):307-12 [PubMed PMID: 18330332]
Level 3 (low-level) evidenceChormanski D, Muzio MR. 17-Hydroxylase Deficiency. StatPearls. 2025 Jan:(): [PubMed PMID: 31536251]