Introduction
The prevertebral muscles of the head and neck include the rectus capitis anterior, rectus capitis lateralis, longus capitis, and longus colli muscles. The prevertebral muscles are posterior to the prevertebral fascia, the posterior border of the retropharyngeal space, and anterior to the cervical vertebral column.[1] The prevertebral muscles constitute a part of the prevertebral or deep layer of the deep cervical fascia of the neck.[2] The principle function of the prevertebral muscles is to span the vertebrae, acting with and antagonizing the deep muscles of the upper back.
This article will briefly discuss some of the features of these muscles, including their origin, insertion, blood supply, innervation, embryology, and surgical and clinical significance.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The prevertebral muscles are located anterior to the cervical column and primarily function in motions of the head and neck at the craniocervical junction.
The longus capitis extends from the occipital bone to the inferior cervical vertebrae from C1-C6.[3] The muscle origins at the anterior tubercles and transverse processes of C3-6 and inserts on the basilar part of the occipital bone. It functions to flex the head at the craniocervical junction.[4]
The longus colli consists of a long, flat muscle that sits on the anterior surface of the spine. It functions to connect the cervical vertebral bodies to associated transverse processes. The longus colli spans multiple cervical motion segments.[4] It consists of three segments: the superior oblique, inferior oblique, and a vertical portion. The superior oblique portion of the longus colli originates on the transverse processes and anterior tubercles of C3-C5 and inserts onto the transverse process and anterior tubercle of C1. The inferior oblique portion originates on the anterior aspect of the T1-T3 vertebral bodies and inserts onto the transverse processes and anterior tubercles of C5-C6.[5] The longus colli muscle acts bilaterally to flex the head and unilaterally to tilt the head at the craniocervical junction.
The rectus capitis lateralis and rectus capitis anterior function to connect the occipital and atlas bones. They originate over the transverse process of C1 and insert onto the jugular process of the occipital bone.[6] They function to flex the head at the atlantooccipital joint when engaged bilaterally and laterally flex the head when engaged on one side.
The prevertebral muscles are enveloped by the prevertebral fascia, which invests in the carotid sheath along with the pretracheal and investing fascia.[2]
Embryology
The muscles of the prevertebral region show their embryonic origin from the dermatomyotome of the somites. The belief is that all the margins of the dermatomyotome help in myotome formation. These finally develop into prevertebral muscles of the neck and back. Some studies demonstrate interesting findings that the myotome develops asymmetrically, with the muscles in the ventral region growing faster compared to those in the dorsal region. By 3D reconstruction and remodeling growth analysis, researchers found that at around the eighth week of fetal life, the medial cervical muscles differentiate into spade-like dorsomedial and rod-like ventrolateral portions.[7]
Blood Supply and Lymphatics
The longus capitis and longus colli receive their blood supply from the ascending cervical branch of the inferior thyroid artery, the ascending pharyngeal artery, a branch of the external carotid artery, and the vertebral artery.[3] The rectus capitis anterior receives blood flow from the ascending pharyngeal artery. It drains into the venous plexus of the vertebral vein along with the rectus capitis lateralis. The rectus capitis lateralis is supplied by branches of the vertebral, occipital, and ascending pharyngeal arteries.[8]
Nerves
The prevertebral muscles are innervated by the dorsal rami of the spinal nerves.[9] The longus capitis receives innervation by direct branches from C1-C3 of the ventromedial branches of the cervical ventral rami. The longus colli is innervated by ventromedial branches from C2-C6 of the cervical ventral rami. The rectus capitis anterior and rectus capitis lateralis are both innervated by dorsolateral branches of the anterior ramus of C1.[10]
Some research suggests that the hypoglossal nerve partially innervates the rectus capitis anterior and lateralis as well.[11]
Muscles
There are four prevertebral muscles of the head and neck. They are
- Rectus capitis anterior muscle
- Rectus capitis lateralis muscle
- Longus capitis muscle and
- Longus colli muscle.
Their origin, insertion, blood supply, nerve supply, and actions have already been explained earlier in this article.
Physiologic Variants
Researchers found a rare case of the levator scapulae bypassing its typical insertion point on the C1 transverse process and fusing with the inferior attachment of the rectus capitis lateralis muscle through cadaveric findings.[7]
Surgical Considerations
The prevertebral muscles have been considered in developing muscular flaps for reconstructive procedures. The longus capitis is the more commonly utilized prevertebral muscle in these cases. The longus capitis is near the cervical sympathetic trunk, superior cervical ganglion, and carotid sheath. With its close spatial relationship to important structures, the longus capitis can be a pedicled flap for head and neck defect repairs with negligible morbidity.[3] These pedicled flaps can be developed cranially or caudally. The longus capitis has been used for flap reconstruction of the soft palate following squamous cell carcinoma of the tonsils.[12]
Transoral surgical resection of oropharyngeal tumors rarely results in exposure of the internal carotid artery. This exposed internal carotid artery can result in a very rare but catastrophic complication of rupture and severe bleeding. This complication is preventable by using prevertebral muscle flaps around the internal carotid artery.[13] In advanced stages, the oropharyngeal or hypopharyngeal squamous cell carcinomas are more at risk of prevertebral muscle invasion.[14]
The anterior surface of the longus colli communicates with the prevertebral fascia, pharynx, esophagus, the cervical sympathetic trunk, the carotid sheath, the inferior thyroid artery, and the recurrent laryngeal nerve. The posterior surface of the longus colli communicates with the cervical spine. The medial border of the longus colli can be used as a landmark to expose the cervical disc spaces and the uncinate process of the cervical spine during a cervical discectomy or corpectomy procedure as a means to avoid injury to the sympathetic trunk.[15] The longus colli muscle has also been used as an anatomical landmark for ultrasound-guided stellate ganglion blocks to prevent spread along the carotid sheath.[16]
The rectus capitis lateralis communicates with the internal jugular vein, the vertebral artery, the occipital artery, and the suboccipital nerve. The rectus capitis lateralis can serve as a surgical landmark in a skull base approach for safe exposure of the jugular foramen.[6]
Clinical Significance
Longus colli tendonitis frequently contributes to neck pain and has been investigated as a cause of cervical vertigo.[17] Longus colli tendonitis is diagnosed with MRI or CT imaging and should be suspected in patients who present with rapid onset of neck pain without an obvious discernable cause.[18] Acute calcific tendinitis of the longus colli occurs secondary to calcium deposition within the tissue resulting in an aseptic inflammatory response.[19] It can present clinically with symptoms of fever, acute cervical pain or neck stiffness, globus sensation, and dysphagia. Longus colli tendonitis may present with a modest elevation in C-reactive protein levels and normal white blood cell counts, which can help with the differential of a deep cervical abscess. It is easily misdiagnosed as a retropharyngeal abscess due to the overlap in symptomology.[20]
Muscle invasion of the prevertebral muscle group has been seen in p16+ oropharyngeal squamous cell carcinoma and has been used to evaluate local and regional recurrence rates.[21]
Furthermore, there is a case example of a severe pyomyositis infection of the prevertebral muscles following acupuncture treatment, presenting with pain in the posterior cervical region, torticollis, and high fever.[22]
Other Issues
The prevertebral muscles sometimes undergo an inflammatory process resulting in prevertebral tendinitis. Even though rare, when present, they are more commonly found in the cervicothoracic region and are usually misdiagnosed as an abscess. They show prevertebral cervical effusion and undergo amorphous calcifications within the prevertebral muscle tendons. MRI is best to detect this condition even though the visualization of the calcifications is better with CT. They also show a slight elevation of CRP, but the WBC count is usually within normal limits.[23]
Media
(Click Image to Enlarge)
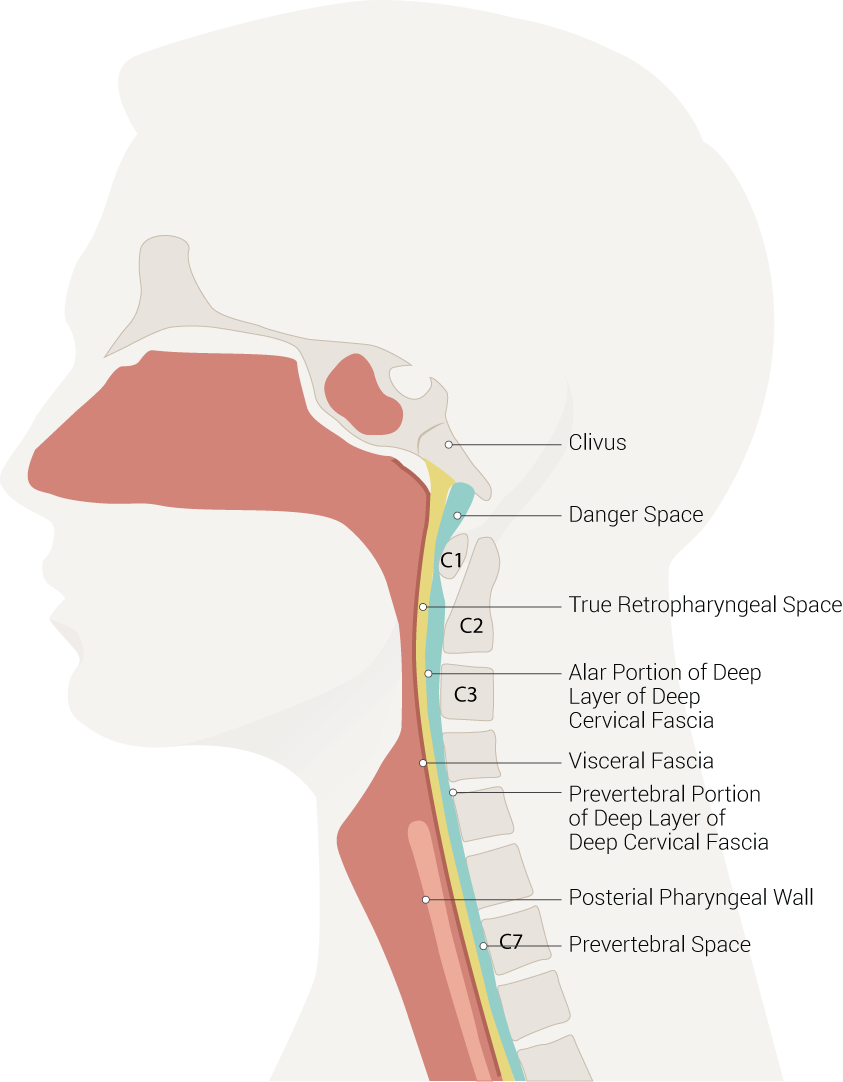
Neck Spaces Pertinent to Retropharyngeal Abscess. The illustration of neck spaces shows the danger space, clivus, true retropharyngeal space, an alar portion of the deep layer of deep cervical fascia, visceral fascia, a prevertebral portion of the deep layer of deep cervical fascia, posterior pharyngeal wall, and prevertebral space.
Contributed by B Palmer
(Click Image to Enlarge)
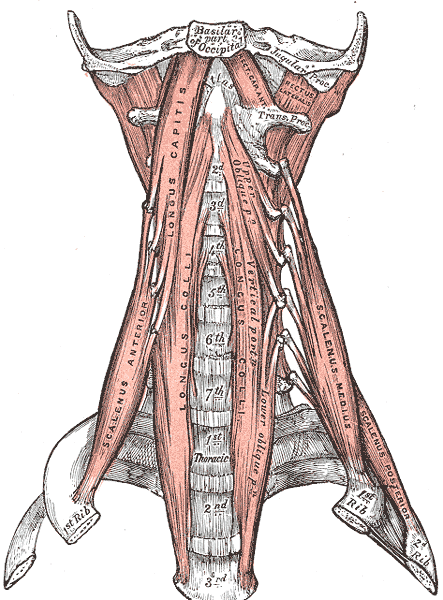
Anterior Muscles of the Neck. Anterior muscles of the neck include the basilar part of the occipital, jugular process, scalenus anterior, longus capitis, longus colli, scalenus medius and posterior, atlas, thoracic vertebrae, and cervical vertebrae.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

Posterior neck muscles Image courtesy S Bhimji MD
(Click Image to Enlarge)
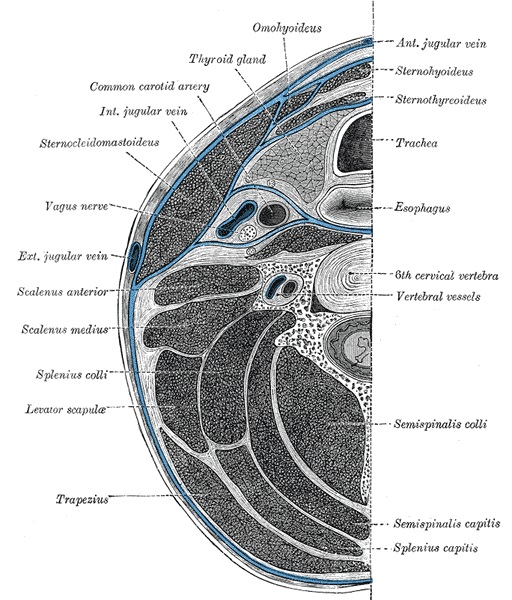
Deep Cervical Fascia of the Neck. The deep cervical fascia of the neck, which is located at the level of the sixth cervical vertebra, is highlighted in blue.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Mnatsakanian A, Minutello K, Black AC, Bordoni B. Anatomy, Head and Neck, Retropharyngeal Space. StatPearls. 2025 Jan:(): [PubMed PMID: 30725729]
Garner DH, Kortz MW, Baker S. Anatomy, Head and Neck: Carotid Sheath. StatPearls. 2025 Jan:(): [PubMed PMID: 30137861]
Zhang XY, Ma TT, Liu L, Yin NB, Zhao ZM. Anatomic study of the musculus longus capitis flap. Surgical and radiologic anatomy : SRA. 2017 Mar:39(3):271-279. doi: 10.1007/s00276-016-1708-8. Epub 2016 Jun 11 [PubMed PMID: 27289229]
Kennedy E, Albert M, Nicholson H. Do longus capitis and colli really stabilise the cervical spine? A study of their fascicular anatomy and peak force capabilities. Musculoskeletal science & practice. 2017 Dec:32():104-113. doi: 10.1016/j.msksp.2017.10.005. Epub 2017 Oct 16 [PubMed PMID: 29107220]
Boyd-Clark LC, Briggs CA, Galea MP. Muscle spindle distribution, morphology, and density in longus colli and multifidus muscles of the cervical spine. Spine. 2002 Apr 1:27(7):694-701 [PubMed PMID: 11923661]
Cohen MA, Evins AI, Lapadula G, Arko L, Stieg PE, Bernardo A. The rectus capitis lateralis and the condylar triangle: important landmarks in posterior and lateral approaches to the jugular foramen. Journal of neurosurgery. 2017 Dec:127(6):1398-1406. doi: 10.3171/2016.9.JNS16723. Epub 2017 Jan 27 [PubMed PMID: 28128694]
Gonzales JR, Iwanaga J, Oskouian RJ, Tubbs RS. Variant Prevertebral Muscle: Unique Cadaveric Findings. Cureus. 2017 Jul 25:9(7):e1515. doi: 10.7759/cureus.1515. Epub 2017 Jul 25 [PubMed PMID: 28959510]
Matsushima K, Funaki T, Komune N, Kiyosue H, Kawashima M, Rhoton AL Jr. Microsurgical anatomy of the lateral condylar vein and its clinical significance. Neurosurgery. 2015 Mar:11 Suppl 2():135-45; discussion 145-6. doi: 10.1227/NEU.0000000000000570. Epub [PubMed PMID: 25255257]
Bogduk N. Functional anatomy of the spine. Handbook of clinical neurology. 2016:136():675-88. doi: 10.1016/B978-0-444-53486-6.00032-6. Epub [PubMed PMID: 27430435]
Sakamoto Y. Spatial relationships between the morphologies and innervations of the scalene and anterior vertebral muscles. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2012 Jul:194(4):381-8. doi: 10.1016/j.aanat.2011.11.004. Epub 2011 Dec 8 [PubMed PMID: 22209543]
Iwanaga J, Fisahn C, Alonso F, DiLorenzo D, Grunert P, Kline MT, Watanabe K, Oskouian RJ, Spinner RJ, Tubbs RS. Microsurgical Anatomy of the Hypoglossal and C1 Nerves: Description of a Previously Undescribed Branch to the Atlanto-Occipital Joint. World neurosurgery. 2017 Apr:100():590-593. doi: 10.1016/j.wneu.2017.01.038. Epub 2017 Jan 19 [PubMed PMID: 28109859]
Gross JH, Zenga J, Sharon JD, Jackson RS, Pipkorn P. Longus Capitis Reconstruction of the Soft Palate. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2019 Sep:161(3):536-538. doi: 10.1177/0194599819849031. Epub 2019 May 14 [PubMed PMID: 31084255]
Day AT, Haughey BH, Rich JT. Prevertebral muscle flap for internal carotid artery coverage during oropharyngeal transoral surgery. The Laryngoscope. 2017 Oct:127(10):2256-2259. doi: 10.1002/lary.26542. Epub 2017 Apr 13 [PubMed PMID: 28407255]
Righi PD, Kelley DJ, Ernst R, Deutsch MD, Gaskill-Shipley M, Wilson KM, Gluckman JL. Evaluation of prevertebral muscle invasion by squamous cell carcinoma. Can computed tomography replace open neck exploration? Archives of otolaryngology--head & neck surgery. 1996 Jun:122(6):660-3 [PubMed PMID: 8639300]
Level 2 (mid-level) evidencePark MS, Moon SH, Kim TH, Oh JK, Kim HJ, Park KT, Riew KD. Surgical Anatomy of the Longus Colli Muscle and Uncinate Process in the Cervical Spine. Yonsei medical journal. 2016 Jul:57(4):968-72. doi: 10.3349/ymj.2016.57.4.968. Epub [PubMed PMID: 27189293]
Narouze S. Ultrasound-guided stellate ganglion block: safety and efficacy. Current pain and headache reports. 2014 Jun:18(6):424. doi: 10.1007/s11916-014-0424-5. Epub [PubMed PMID: 24760493]
Shen Y, Zhou Q, Zhu X, Qiu Z, Jia Y, Liu Z, Li S. Vertigo caused by longus colli tendonitis: A case report and literature review. Medicine. 2018 Nov:97(45):e13130. doi: 10.1097/MD.0000000000013130. Epub [PubMed PMID: 30407336]
Level 2 (mid-level) evidenceBoardman J, Kanal E, Aldred P, Boonsiri J, Nworgu C, Zhang F. Frequency of acute longus colli tendinitis on CT examinations. Emergency radiology. 2017 Dec:24(6):645-651. doi: 10.1007/s10140-017-1537-z. Epub 2017 Jul 25 [PubMed PMID: 28744692]
Raggio BS, Ficenec SC, Pou J, Moore B. Acute Calcific Tendonitis of the Longus Colli. Ochsner journal. 2018 Spring:18(1):98-100 [PubMed PMID: 29559880]
Naik PP, Savery N, Kuruvilla L, Nayakar G, Raghul T. Longus Colli Tendinitis: The Lost Twin of Retropharyngeal Abscess. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2019 Oct:71(Suppl 1):771-775. doi: 10.1007/s12070-018-1541-y. Epub 2018 Nov 30 [PubMed PMID: 31742062]
Farzal Z, Du E, Yim E, Mazul A, Zevallos JP, Huang BY, Hackman TG. Radiographic muscle invasion not a recurrence predictor in HPV-associated oropharyngeal squamous cell carcinoma. The Laryngoscope. 2019 Apr:129(4):871-876. doi: 10.1002/lary.27351. Epub 2018 Oct 16 [PubMed PMID: 30325502]
Tucciarone M, Taliente S, Gómez-Blasi Camacho R, Souviron Encabo R, González-Orús Álvarez-Morujo R. Extensive pyomyositis of prevertebral muscles after acupuncture: Case report. Turkish journal of emergency medicine. 2019 Jul:19(3):113-114. doi: 10.1016/j.tjem.2019.03.003. Epub 2019 Apr 4 [PubMed PMID: 31321345]
Level 3 (low-level) evidenceVollmann R, Hammer G, Simbrunner J. Pathways in the diagnosis of prevertebral tendinitis. European journal of radiology. 2012 Jan:81(1):114-7. doi: 10.1016/j.ejrad.2011.02.061. Epub 2011 Mar 24 [PubMed PMID: 21439752]
Level 3 (low-level) evidence