 Anatomy, Head and Neck, Posterior Auricular Nerve
Anatomy, Head and Neck, Posterior Auricular Nerve
Introduction
The posterior auricular nerve is an extracranial branch of the facial nerve, cranial nerve VII, that supplies relatively small muscles of the head and neck. It sometimes receives consideration during head and neck surgery as a potential source of iatrogenic injury, and it has been proposed to be a possible candidate for utilization as a nerve graft donor.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The posterior auricular nerve branches off of the facial nerve close to the stylomastoid foramen, the location in which the facial nerve exits the cranium. The stylomastoid foramen is on the undersurface of the skull, between the styloid and mastoid processes. Upon branching from the facial nerve, the posterior auricular nerve ascends along the mastoid posterior to the external auditory meatus, where it again divides into two separate branches. The auricular branch supplies the auricularis posterior muscle as well as some of the intrinsic muscles of the ear and the interscutularis muscle. The second branch, the occipital branch, proceeds posteriorly to supply the occipitalis muscle, running along the superior nuchal line. The occipitalis muscle, supplied by the occipital branch of the posterior auricular nerve, connects to the frontalis muscle by the epicranial aponeurosis, and thus may also be considered to be one muscle, occipitofrontalis.
As the posterior auricular nerve ascends superiorly between the mastoid and the external auditory meatus, it joins with the posterior branch of the great auricular nerve and the lesser occipital nerve, which provide sensation to the skin overlying the mastoid, parotid gland, and posterior pinna. The posterior auricular nerve also joins with part of the auricular branch of the vagus nerve, known eponymously as Arnold’s nerve, which may be involved in Arnold nerve cough reflex, Ramsay Hunt syndrome, and Hitselberger sign.[1][2]
Embryology
The posterior auricular nerve, as a branch of the facial nerve, develops from the second branchial arch, which also has associations with the supplied muscular structures including the muscles of facial expression, the auricularis muscles, and the occipitofrontalis.
Blood Supply and Lymphatics
The posterior auricular artery, which is a tributary of the external carotid artery, runs with the posterior auricular nerve in its course along the mastoid and superior nuchal line. The facial nerve trunk crosses it inferior to the stylomastoid foramen.[3] The vein responsible for draining the surrounding areas is known as the posterior auricular vein, which drains into the external jugular vein.[4]
Muscles
The posterior auricular nerve supplies the occipitalis muscle, part of the occipitofrontalis muscle, as well as the auricularis posterior (a vestigial muscle in humans), interscutularis, and intrinsic ear muscles.
Physiologic Variants
Although the posterior auricular nerve is thought to always run posteriorly to the external auditory meatus as it ascends the mastoid, a case report in a 2013 issue of British Journal of Oral and Maxillofacial Surgery by Colbert et al. demonstrated an anatomical variant in which the nerve ran anterior to the external auditory meatus. The authors confirmed that the nerve in question was the posterior auricular nerve via intraoperative nerve stimulation during a Warthin tumor removal from the parotid gland. They found that when the nerve in question was stimulated, there was a resultant contraction of the posterior occipitalis and auricular musculature. The authors determined that this was a previously unreported anatomical variation of the posterior auricular nerve, arguing that surgeons utilize every landmark available when considering the anatomy of the facial nerve intraoperatively.[5]
Surgical Considerations
During a parotidectomy, there have been demonstrable improvements in outcomes with sparing of the posterior branch of the great auricular nerve, which runs with the posterior auricular nerve. This allows a higher likelihood for patients to retain the sensation of their lobule and antitragus, thus improving patient outcomes as demonstrated in a 2017 prospective controlled trial by Grosheva et al.[6]
Additionally, a 2019 cadaveric study by Kikuta et al. proposed that utilizing the posterior auricular nerve as a nerve graft for in cases of facial nerve paralysis. They found the nerve to have adequate length and diameter to be used for such a purpose.[7]
The posterior auricular nerve may also serve as a suitable landmark to use to find the facial nerve trunk, as published by Blau et al. in a 2019 cadaveric dissection study. The posterior auricular nerve was found to be a consistent anatomical landmark, which could be traced to the facial nerve trunk without the worry of compromise of the supplied structures, as the auricularis posterior is a vestigial structure. Using this method, there is theoretically less risk of harming the facial nerve trunk. The authors also state that this method could be useful in revision operations as the normal anatomy will have changed, leading to a higher risk of iatrogenic facial nerve injury.[8] Clinical trials would be necessary to determine if this would have clinical utility.
In a May 2019 study published in the Annals of Anatomy, by Leckenby et al., the authors demonstrated that the motor function of the interscutularis muscle could be reliably utilized to help determine outcomes of facial nerve surgery using a rodent model. The authors noted that excision of the posterior auricular nerve during surgery led to no significant recovery of the interscutularis muscle compared with a crush injury and a sham group. In the crushed nerve group, recovery of the function of the interscutularis muscle typically occurred by post-operative day 30 compared with complete recovery by post-operative day 5 in the sham group. The validity of these results pertinent to usage for measurements of outcome in human surgical patients is unlikely to be applied due to the somewhat vestigial nature of the interscutularis muscle.[9]
The posterior branches of the great auricular nerve, which also contribute to the posterior auricular nerve, are potentially prone to damage during face and neck lift surgeries. These posterior branches have been shown to be less at-risk during the procedure if the posterior auricular sulcus skin flap gets elevated above the auricularis posterior muscle.[10]
Clinical Significance
If damage occurs to the posterior auricular nerve alone, either intentionally as part of a potential nerve graft or unintentionally as a complication of surgery, the patient will likely complain of difficulty moving the muscles with which it is associated. As these muscles are mostly vestigial and unessential to quality of life, it is unlikely that it will impact the patient to any significant degree. As a branch of cranial nerve VII, the fibers of the posterior auricular nerve may also become paralyzed as part of greater facial nerve paralysis, such as in the case of Bell palsy.
Media
(Click Image to Enlarge)
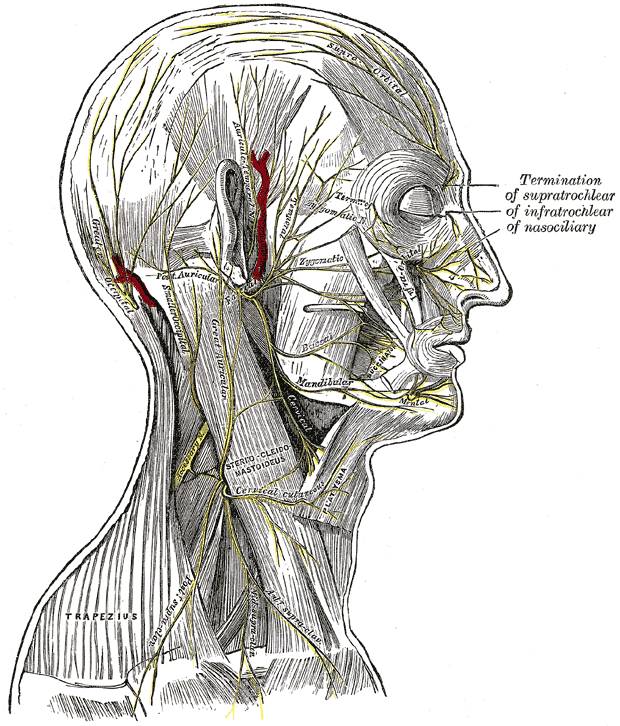
Superficial nerves of the head and neck
Henry Vandyke Carter, (plate 790), Public Domain, via Wikimedia Commons
References
Mulazimoglu S, Flury R, Kapila S, Linder T. Effects of a sensory branch to the posterior external ear canal: coughing, pain, Ramsay Hunt's syndrome and Hitselberger's sign. The Journal of laryngology and otology. 2017 Apr:131(4):329-333. doi: 10.1017/S0022215117000160. Epub 2017 Feb 8 [PubMed PMID: 28173896]
Takezawa K, Townsend G, Ghabriel M. The facial nerve: anatomy and associated disorders for oral health professionals. Odontology. 2018 Apr:106(2):103-116. doi: 10.1007/s10266-017-0330-5. Epub 2017 Dec 14 [PubMed PMID: 29243182]
Liu M, Wang SJ, Benet A, Meybodi AT, Tabani H, Ei-Sayed IH. Posterior auricular artery as a novel anatomic landmark for identification of the facial nerve: A cadaveric study. Head & neck. 2018 Jul:40(7):1461-1465. doi: 10.1002/hed.25127. Epub 2018 Mar 22 [PubMed PMID: 29566447]
Germann AM, Jamal Z, Al Khalili Y. Anatomy, Head and Neck, Scalp Veins. StatPearls. 2024 Jan:(): [PubMed PMID: 31082005]
Colbert SD,Davies J,Aldridge T,Brennan PA, Posterior auricular nerve found anterior to the cartilage of the external auditory meatus--a previously unreported variant. The British journal of oral & maxillofacial surgery. 2013 Jul [PubMed PMID: 23159194]
Level 3 (low-level) evidenceSensation loss after superficial parotidectomy: A prospective controlled multicenter trial., Grosheva M,Shabli S,Volk GF,Sommer B,Ludwig L,Finkensieper M,Wittekindt C,Klussmann JP,Guntinas-Lichius O,Beutner D,, Head & neck, 2017 Mar [PubMed PMID: 28067982]
Level 1 (high-level) evidenceKikuta S, Iwanaga J, Watanabe K, Kusukawa J, Tubbs RS. The Feasibility of Using the Posterior Auricular Branch of the Facial Nerve as a Donor for Facial Nerve Reanimation Procedures: A Cadaveric Study. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2019 Jul:77(7):1470.e1-1470.e8. doi: 10.1016/j.joms.2019.02.043. Epub 2019 Mar 13 [PubMed PMID: 30959011]
Level 2 (mid-level) evidenceBlau I,Vaisbuch Y,Marom A, A new method for tracing the facial nerve trunk using the posterior auricular nerve. Clinical anatomy (New York, N.Y.). 2019 Apr [PubMed PMID: 30664254]
Leckenby JI, Chacon MA, Rolfe K, Lichtman JW, Grobbelaar AO. Development of the interscutularis model as an outcome measure for facial nerve surgery. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2019 May:223():127-135. doi: 10.1016/j.aanat.2019.03.001. Epub 2019 Mar 22 [PubMed PMID: 30910682]
Lee JH,Oh TS,Park SW,Kim JH,Tansatit T, Temple and Postauricular Dissection in Face and Neck Lift Surgery. Archives of plastic surgery. 2017 Jul [PubMed PMID: 28728320]