 Anatomy, Bony Pelvis and Lower Limb: Popliteal Region
Anatomy, Bony Pelvis and Lower Limb: Popliteal Region
Introduction
The popliteal fossa is a shallow depression located posterior to the knee joint. This area is often referred to as the knee "pit" and may develop vascular, nervous, lymphatic, and adipose issues as well as swelling and masses.[1] The fossa houses several important structures that are essential for lower extremity function. Anatomic boundaries of the popliteal fossa include the following:
- Superomedially, the semimembranosus, and semitendinosus muscles
- Superolaterally, the biceps femoris muscle (short and long heads)
- Inferomedial and inferolateral, the medial and lateral heads of the gastrocnemius muscle contribute to the lower border, respectively.
- The plantaris muscle also runs deep to the gastrocnemius to form the inferolateral border.
- The roof of the fossa, proceeding from most superficial to deep, consists of the skin, superficial fascia, and deep (popliteal) fascia.
- The floor of the fossa includes the popliteal surface of the femur, the capsule of the knee joint, popliteal ligament, and fascia encasing the popliteus muscle.
It is important to understand the involved anatomy of the popliteal fossa because patients could present with posterior knee pain due to multiple etiologies. One of the more common issues involving the posterior knee is a Baker cyst; it has a fluid-filled bursa, which is usually secondary to friction or irritation. Other causes of posterior knee pain could be a popliteal artery aneurysm, lymphadenopathy, thrombophlebitis, and very rarely, sarcomas.[2] Proper diagnosis is essential for effective treatment and management.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The function of the popliteal fossa is closely associated with the critical anatomic structures it contains. The fossa is a diamond-shaped region directly posterior to the knee and clinically appears as a soft impression behind the knee. It is an important area serving as a transition point/conduit for nerve tissue, vasculature, lymphatic tissue, and musculoskeletal structures, which are discussed at length below.
Embryology
Limb bud development of the lower extremity develops beginning in the fourth week of gestation. It follows upper extremity bud development by a few days. The lower extremity continues to lengthen into week 5 and undergoes a series of rotations and regional morphological development into the thigh, leg, and foot regions. Somites give rise to dermatomes, sclerotomes, and myotomes which allow for full development of the structures within these extremities.[3]
Blood Supply and Lymphatics
Popliteal Artery
The predominant arterial supply in the popliteal fossa is the popliteal artery. The artery represents the distal continuation of the femoral artery after passing through the adductor hiatus of the adductor magnus muscle. The popliteal artery then ends at the lower border of the popliteus muscle before further dividing into the anterior tibial artery and the common trunk of the posterior tibial and peroneal arteries.[4] Five genicular branches of the popliteal artery provide blood to the capsular structures and ligaments of the knee: superior lateral, superior medial, middle, inferior lateral, and inferior medial genicular arteries. The genicular arteries form a collateral network between the femoral artery and the popliteal artery. This dense vascular network allows for an alternative pathway for blood to flow from the femoral to popliteal arteries. [5]
- Medial superior genicular artery: branch of the popliteal artery that runs anterior to the semimembranosus and semitendinosus. Anastomoses with lateral superior genicular artery.
- Lateral superior genicular artery: branch of the popliteal artery that passes above lateral femoral condyle. Anastomoses with medial superior genicular artery, lateral femoral circumflex, and lateral inferior genicular arteries.
- Medial inferior genicular artery: arises from the popliteal artery and descends with popliteus muscle, then passes the medial tibial condyle. Anastomoses with lateral inferior and medial superior genicular arteries.
- Lateral inferior genicular artery: arises from the popliteal artery and passes under the gastrocnemius. Anastomoses with inferior medial genicular, superior lateral genicular, and anterior recurrent tibial artery.
- Middle genicular artery: branch of the popliteal artery that supplies the ligaments and synovial membrane of the knee joint. [6]
Popliteal Vein
The popliteal vein is superficial to the popliteal artery in the fossa. The popliteal vein receives venous circulation from several tributaries. The anterior tibial vein, posterior tibial vein, and the peroneal vein merge at the popliteus muscle to make the popliteal vein. Within the popliteal fossa, the small saphenous vein feeds into the popliteal vein and is located more superficially, but transverses the deep fascia in between both gastrocnemius heads. Similarly to the popliteal artery, the popliteal vein extends superiorly through the adductor hiatus before transitioning into the femoral vein.[7]
Popliteal lymph nodes can be found in the fossa, as well. Several are located in the fat embedded in the fossa. There are also nodes found beneath the popliteal fascia as well as along the popliteal vessels. These nodes' efferent path mostly follows the femoral vessels and drains into the deep inguinal lymph tissue. Some popliteal nodes may also be located near the great saphenous vein and travel more to the superficial inguinal lymph tissue.[8][9]
Nerves
The sciatic nerve branches into the tibial and common peroneal nerve just anterior to the popliteal fossa. The tibial nerve then enters the posterior legs between the heads of the gastrocnemius. The common peroneal nerve passes around the neck of the fibula.
Tibial Nerve
The tibial nerve is a branch of the sciatic nerve consisting of nerve roots L4-S3. It is superficial to the popliteal vessels and travels laterally to medially from the superior angle to the inferior angle of the popliteal fossa, respectively. The tibial nerve contains muscular, articular, and cutaneous branches. Muscular branches in the distal portion of the fossa supply the medial and lateral heads of the gastrocnemius, soleus, plantaris, and popliteal muscles.
The sural nerve is the cutaneous branch of the tibial nerve and extends from the middle of the popliteal fossa, providing innervation of the lower posterior half of the lower leg and lateral foot. The three articular branches arise from the superior portion of the fossa. The superior medial genicular is found at the medial femoral condyle, and the middle genicular nerve pierces the posterior capsule of the knee joint innervating intercondylar structures and the inferior genicular nerve which travels to the medial tibial condyle.[10][11]
Common Peroneal Nerve
The common peroneal nerve also referred to as the common fibular nerve, consists of nerve roots L4-S2 and arises from the sciatic nerve as well. It branches approximately at the superior angle of the popliteal fossa and travels to the lateral angle where it wraps around the fibular head, splitting off into the deep and superficial peroneal nerves and innervating the anterior and lateral compartments of the lower leg, respectively. It also has cutaneous and articulating branches but no direct motor branches as these are provided by the deep and superficial peroneal nerves. The cutaneous nerves are the lateral sural cutaneous, which provides sensation to the lateral proximal two-thirds of the calf, and the peroneal communicating nerve, which joins with the sural nerve providing sensation to the posterolateral calf. The articulating branches are the superior lateral genicular, inferior lateral genicular, and recurrent genicular nerves. The superior lateral genicular nerve lies over the lateral femoral condyle, and the inferior lateral genicular nerve lies over the fibular head. The recurrent genicular nerve ascends anteriorly close to the division of the common fibular nerve and supplies the knee joint as well as the tibialis anterior muscle.[11][12]
Muscles
The musculoskeletal structures found in the popliteal fossa form its boundaries. The fossa has the shape of a rhombus or diamond and is made up of the following musculoskeletal structures.
- Superomedial: The semimembranosus and semitendinosus muscles form the superomedial aspect of the fossa. The semimembranosus is the most medial of the hamstring muscles and functions to extend the hip and flex the knee as well as assist in medial rotation of the knee. The semitendinosus muscle is superficial to the semimembranosus and is the middle of the three hamstring muscles. Not surprisingly, it gets its name because of the long tendinous nature of its structure and assists in the same mechanism as the semimembranosus muscle.[13]
- Superolateral: The biceps femoris forms the superolateral portion of the popliteal fossa and has two functioning heads. The long head is part of the hamstring muscles while the short head is not included in this description. Both structures participate in knee flexion, while the long head additionally assists in hip extension.[13]
- Inferomedial: The medial head of the gastrocnemius forms the inferomedial border of the fossa. It assists the lower leg in plantarflexion at the ankle and knee flexion when contracted. Along with the lateral head of the gastrocnemius and soleus, it forms the calf muscle.[14]
- Inferolateral: The lateral head of the gastrocnemius and the plantaris muscle forms the inferolateral border of the popliteal fossa. Both contribute to plantarflexion of the ankle. The lateral gastrocnemius head also contributes to knee flexion. The plantaris muscle is notably the longest tendon in the body and is not found in every human being.[14]
Physiologic Variants
Physiologic variants in the popliteal fossa are a common finding and are seen most commonly in the branches of the popliteal artery and sciatic nerve. Studies have revealed seven major branching variances in decreasing order of frequency: aplastic or hypoplastic posterior tibial artery; hypoplastic or aplastic anterior tibial artery; trifurcation; high origin of the anterior tibial artery; hypoplastic or aplastic posterior tibial and anterior tibial arteries; high origin of the posterior tibial branch; and anterior tibioperoneal trunk. Also of note, when a variant is discovered on either extremity, the probability of a variant being found in the contralateral extremity is approximately 28%. If one side has normal vascular anatomy, the probability of a physiologic variant in the contralateral extremity is close to 13%.[15]
Usually, the sciatic nerve divides into the tibial nerve and common peroneal nerve at the level of the superior angle of the popliteal fossa. However, the most common variant branching pattern of the sciatic nerve division is found superior to this landmark. Divisions as high as in the pelvis have been seen, however, the majority of the sciatic nerve divisions into tibial and peroneal components are most often seen outside of the pelvis.[16]
Surgical Considerations
A posterior surgical approach to the knee is valuable when treating certain etiologies of the knee and depends on the surgeon's knowledge of anatomy as well as the step-by-step process to ensure success. Multiple knee pathologies may be addressed with this approach, including (but not limited to) the following:
- Baker's cyst excision
- Medial meniscus posterior horn repair
- Tibial inlay technique for posterior cruciate ligament (PCL) reconstruction
- Tibial plateau fracture fixation (ORIF)
Several factors should be kept in mind with a posteromedial approach to the knee in evaluating the popliteal fossa. To avoid skin necrosis, the surgeon should avoid making sharp angles when transitioning from a vertical to a transverse incision and should include adequate subcutaneous tissue of the skin flap. Also, using blunt dissection when handling the neurovascular bundle is important to avoid injury to these structures. Careful closure of the fascia is also important to keep from injuring the tibial nerve which is the most superficial structure of the bundle. Being aware of anatomic variations in patients is vital to avoid damaging nearby structures and is a common issue clinicians face.[17]
There are benefits and risks with any surgical approach. Regarding the posteromedial approach, specifically, using a transverse incision provides a clear view of the femoral condyles, musculature, and ligamentous structures of the knee as well as potential pathology (i.e., Baker cyst). This is the preferred approach for posterior cruciate ligament avulsions, malignancies, and posterior tibial plateau fractures to name a few. Additionally, this incision is cosmetically preferred as it is well hidden in the popliteal fold. One of the concerns with the posteromedial approach is the possibility of a flexion contracture of the knee secondary to inadequate closure of the incision. Anesthesia-related complications may also be seen due to the prone positioning of the patient during the operation.[17]
Clinical Significance
Posterior Circulation
The popliteal pulse can be evaluated to assess peripheral circulatory status in the same way one may examine radial or posterior tibial arterial pulses. A patient with significant peripheral arterial disease or diabetes may have poor circulation and difficulty ascertaining dorsalis pedal or posterior tibial pulses. The physician may then need to continue to move more proximally to gain a better clinical picture of the patient's arterial flow and can accomplish this by palpating the popliteal pulse. The most efficient way to appreciate this on the physical exam is flexing the knee slightly while gripping the extremity with both hands. The physician's thumbs should be over the patella with both fingertips of each hand in the fossa. It can be difficult to assess the popliteal pulse and is more challenging than those typically evaluated at the ankle and dorsum of the foot.
Popliteal Artery Aneurysms
Popliteal artery aneurysms are the most common true peripheral arterial aneurysm and are only second in prevalence to abdominal aortic aneurysms.[18] Aneurysm diagnosis is made when vessel size is 50% greater relative to the vessel's typical diameter.[19] Multiple causes for this pathology include but are not limited to inflammation, genetics, immunologic, and mechanical factors. Men are more commonly affected than women and present younger.[20] Sixty percent of patients with this diagnosis have a pulsatile mass posterior at or superior to the knee joint. First-line imaging modality for diagnosis is duplex ultrasonography, but CT or MR angiography may also be used if ultrasound is not available.[21] Conservative management may be a reasonable approach. depending on the size of the aneurysm, typically less than 2 cm. Clinical presentation is an important factor, as well, although management is somewhat under debate, particularly if a thrombus is present. Indications for repair include symptomatic patients presenting with acute limb ischemia regardless of aneurysm size. Patent aneurysms greater than or equal to 2 cm are also recommended to be repaired due to the high risk of ischemic complications and subsequent limb loss.[22]
Baker's Cyst
A popliteal cyst, more commonly called a Baker's cyst, is an enlargement of the gastrocnemius-semimembranosus bursa which communicates with the knee joint in adults. Baker cysts are usually secondary to underlying internal derangement of the knee, whether it be inflammatory, degenerative, or injury. Diagnosis is usually made on clinical grounds and is very apparent on palpation of the extended knee while others are diagnosed by visual evidence of MRI or CT scan. Careful evaluation is needed to rule out other significant pathologies such as a popliteal aneurysm or deep vein thrombosis (DVT), and duplex ultrasonography is suggested to rule these out. These cysts can be uncomfortable due to mass effect and compression of surrounding structures. They may enlarge, dissect, or rupture which may provide temporary relief. Treatment may also involve arthrocentesis in addition to intra-articular steroid injections to reduce inflammation. However, recurrence is and addressing the underlying pathology surgically may be warranted as the cyst is a secondary effect.[23]
Peroneal Neuropathy
As discussed, the peroneal nerve is a branch of the sciatic nerve that travels in the popliteal fossa before transferring the laterally around the neck of the fibula. Based on its anatomic location, the nerve is susceptible to injury. Peroneal neuropathy is the most common mononeuropathy of the lower limb. Classically, this neuropathy presents with foot drop and sensory changes over the lower limb. The peroneal nerve is likely to be injured by a fibular neck fracture, tibiofibular fracture, or tibial plateau fracture. [24]
Media
(Click Image to Enlarge)
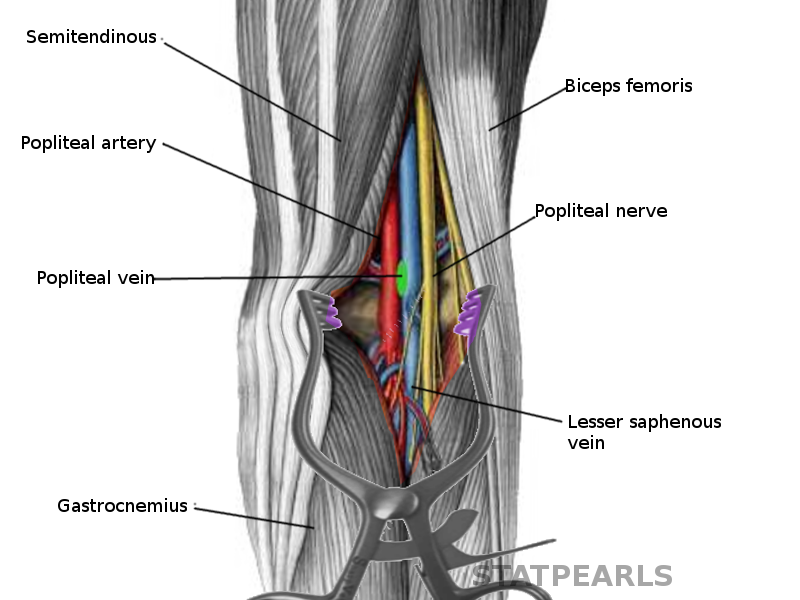
Popliteal fossa Image courtesy S Bhimji MD
References
Dagur G, Gandhi J, Smith N, Khan SA. Anatomical Approach to Clinical Problems of Popliteal Fossa. Current rheumatology reviews. 2017:13(2):126-138. doi: 10.2174/1573397112666161128102959. Epub [PubMed PMID: 27894238]
Saavedra MÁ, Navarro-Zarza JE, Villaseñor-Ovies P, Canoso JJ, Vargas A, Chiapas-Gasca K, Hernández-Díaz C, Kalish RA. Clinical anatomy of the knee. Reumatologia clinica. 2012 Dec-2013 Jan:8 Suppl 2():39-45. doi: 10.1016/j.reuma.2012.10.002. Epub 2012 Dec 6 [PubMed PMID: 23219082]
Guidera KJ, Ganey TM, Keneally CR, Ogden JA. The embryology of lower-extremity torsion. Clinical orthopaedics and related research. 1994 May:(302):17-21 [PubMed PMID: 8168296]
Tomaszewski KA, Popieluszko P, Graves MJ, Pękala PA, Henry BM, Roy J, Hsieh WC, Walocha JA. The evidence-based surgical anatomy of the popliteal artery and the variations in its branching patterns. Journal of vascular surgery. 2017 Feb:65(2):521-529.e6. doi: 10.1016/j.jvs.2016.01.043. Epub 2016 Mar 16 [PubMed PMID: 26994952]
Shahid S, Saghir N, Cawley O, Saujani S. A Cadaveric Study of the Branching Pattern and Diameter of the Genicular Arteries: A Focus on the Middle Genicular Artery. The journal of knee surgery. 2015 Oct:28(5):417-24. doi: 10.1055/s-0035-1549021. Epub 2015 Apr 18 [PubMed PMID: 25892007]
Hirtler L, Lübbers A, Rath C. Vascular coverage of the anterior knee region - an anatomical study. Journal of anatomy. 2019 Aug:235(2):289-298. doi: 10.1111/joa.13004. Epub 2019 May 9 [PubMed PMID: 31070789]
Ma J, Ma T, Zhao X, Li YM, Wang R, Lü X. [The application of popliteal vein anatomy study and valve construction procedure]. Zhonghua wai ke za zhi [Chinese journal of surgery]. 2013 May 1:51(5):403-6 [PubMed PMID: 23958161]
Pan WR, Wang DG, Levy SM, Chen Y. Superficial lymphatic drainage of the lower extremity: anatomical study and clinical implications. Plastic and reconstructive surgery. 2013 Sep:132(3):696-707. doi: 10.1097/PRS.0b013e31829ad12e. Epub [PubMed PMID: 23985641]
Yamazaki S, Suami H, Imanishi N, Aiso S, Yamada M, Jinzaki M, Kuribayashi S, Chang DW, Kishi K. Three-dimensional demonstration of the lymphatic system in the lower extremities with multi-detector-row computed tomography: a study in a cadaver model. Clinical anatomy (New York, N.Y.). 2013 Mar:26(2):258-66. doi: 10.1002/ca.22179. Epub 2013 Jan 22 [PubMed PMID: 23339085]
Level 3 (low-level) evidenceNorzana AG, Farihah HS, Fairus A, Teoh SL, Nur AK, Faizah O, Das S. Higher division of the tibial nerve in the leg: gross anatomical study with clinical implications. La Clinica terapeutica. 2013:164(1):1-3. doi: 10.7417/CT.2013.1501. Epub [PubMed PMID: 23455733]
Giuffre BA, Black AC, Jeanmonod R. Anatomy, Sciatic Nerve. StatPearls. 2023 Jan:(): [PubMed PMID: 29494038]
Watt T, Hariharan AR, Brzezinski DW, Caird MS, Zeller JL. Branching patterns and localization of the common fibular (peroneal) nerve: an anatomical basis for planning safe surgical approaches. Surgical and radiologic anatomy : SRA. 2014 Oct:36(8):821-8. doi: 10.1007/s00276-013-1242-x. Epub 2013 Nov 30 [PubMed PMID: 24292499]
Attum B, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Thigh Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 29494052]
Binstead JT, Munjal A, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Calf. StatPearls. 2023 Jan:(): [PubMed PMID: 29083629]
Kil SW, Jung GS. Anatomical variations of the popliteal artery and its tibial branches: analysis in 1242 extremities. Cardiovascular and interventional radiology. 2009 Mar:32(2):233-40. doi: 10.1007/s00270-008-9460-z. Epub 2008 Nov 4 [PubMed PMID: 18982387]
Level 2 (mid-level) evidenceAdibatti M, V S. Study on variant anatomy of sciatic nerve. Journal of clinical and diagnostic research : JCDR. 2014 Aug:8(8):AC07-9. doi: 10.7860/JCDR/2014/9116.4725. Epub 2014 Aug 20 [PubMed PMID: 25302181]
Faucett SC, Gannon J, Chahla J, Ferrari MB, LaPrade RF. Posterior Surgical Approach to the Knee. Arthroscopy techniques. 2017 Apr:6(2):e391-e395. doi: 10.1016/j.eats.2016.10.013. Epub 2017 Apr 3 [PubMed PMID: 28580257]
Ravn H, Wanhainen A, Björck M. Risk of new aneurysms after surgery for popliteal artery aneurysm. The British journal of surgery. 2008 May:95(5):571-5. doi: 10.1002/bjs.6074. Epub [PubMed PMID: 18306151]
Johnston KW, Rutherford RB, Tilson MD, Shah DM, Hollier L, Stanley JC. Suggested standards for reporting on arterial aneurysms. Subcommittee on Reporting Standards for Arterial Aneurysms, Ad Hoc Committee on Reporting Standards, Society for Vascular Surgery and North American Chapter, International Society for Cardiovascular Surgery. Journal of vascular surgery. 1991 Mar:13(3):452-8 [PubMed PMID: 1999868]
Level 1 (high-level) evidenceLawrence PF, Lorenzo-Rivero S, Lyon JL. The incidence of iliac, femoral, and popliteal artery aneurysms in hospitalized patients. Journal of vascular surgery. 1995 Oct:22(4):409-15; discussion 415-6 [PubMed PMID: 7563401]
Martelli E, Ippoliti A, Ventoruzzo G, De Vivo G, Ascoli Marchetti A, Pistolese GR. Popliteal artery aneurysms. Factors associated with thromboembolism and graft failure. International angiology : a journal of the International Union of Angiology. 2004 Mar:23(1):54-65 [PubMed PMID: 15156131]
Level 2 (mid-level) evidenceAscher E, Markevich N, Schutzer RW, Kallakuri S, Jacob T, Hingorani AP. Small popliteal artery aneurysms: are they clinically significant? Journal of vascular surgery. 2003 Apr:37(4):755-60 [PubMed PMID: 12663974]
Level 2 (mid-level) evidenceHandy JR. Popliteal cysts in adults: a review. Seminars in arthritis and rheumatism. 2001 Oct:31(2):108-18 [PubMed PMID: 11590580]
Kim YC, Jung TD. Peroneal neuropathy after tibio-fibular fracture. Annals of rehabilitation medicine. 2011 Oct:35(5):648-57. doi: 10.5535/arm.2011.35.5.648. Epub 2011 Oct 31 [PubMed PMID: 22506187]