Introduction
Cartilage has many functions, including the ability to resist compressive forces, enhance bone resilience, and provide support in bony areas where flexibility is needed (see Image. Cartilage and Bone Illustration). The primary cell that makes cartilage is the chondrocyte, which resides within the lacunae. The cartilage matrix consists of fibrous tissue and various combinations of proteoglycans and glycosaminoglycans. Cartilage, once synthesized, lacks lymphatic or blood supply, and the movement of waste and nutrition is chiefly done via diffusion to and from adjacent tissues. Cartilage, like bone, is surrounded by a perichondrium-like fibrous membrane. This layer is not efficient at regenerating cartilage. Hence, its recovery is slow after injury. The lack of active blood flow is the major reason any injury to cartilage takes a long time to heal. Cartilage has no nerve innervation; hence, there is no sensation when injured or damaged. When cartilage is calcified, the chondrocytes die. This is followed by the replacement of cartilage with bone-like tissue. Unlike bone, cartilage does not have calcium in the matrix. Instead, it contains high amounts of chondroitin, which is the material that provides elasticity and flexibility.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Several types of cartilage are found in the human body, and their structure and relevant function depend on this variation.
Hyaline Cartilage
Hyaline cartilage is the most copious type of cartilage in the human body.[1] It is pale blue-white and smooth to the touch. It is primarily composed of type II collagen and proteoglycans. The surface is usually moist, but the cartilage becomes dry, thinner, and more yellow with age. Hyaline cartilage is usually found in the trachea, nose, epiphyseal growth plate, sternum, and ventral segments of the ribs. Hyaline cartilage produces a resilient surface with minimal friction. It also has an excellent ability to resist compressive forces at sites of bone articulation.[2]
Elastic Cartilage
This cartilage appears a dull yellow and is most commonly found in the larynx, ear, epiglottis, and eustachian tube. A perichondrium-like layer also surrounds it. It provides flexibility and is resilient to pressure.[3]
Fibrocartilage
This is abundant in type 1 collagen and contains significantly less proteoglycan than hyaline cartilage. It can resist high degrees of tension and compression. It is commonly found in tendons, ligaments, intervertebral discs, some bones' articular surfaces, and menisci (see Image. Triangular Fibrocartilage Complex). Unlike other cartilages, it has no perichondrium).[4]
Embryology
Cartilage is formed from the mesoderm germ layer by the process known as chondrogenesis.[5] Mesenchyme differentiates into chondroblasts, which are the cells that secrete the major components of the extracellular matrix—the most important components for cartilage formation are aggrecan and type II collagen (see Image. Cartilage). Once initial chondrification occurs, the immature cartilage grows mainly by developing into a more mature state since it cannot grow by mitosis. There is minimal cell division in cartilage; therefore, the size and mass of cartilage do not change significantly after initial chondrification.
Blood Supply and Lymphatics
Cartilage is avascular. This characteristic of cartilage is paramount during the discussion and management of diseases affecting cartilage. Since there is no direct blood supply, chondrocytes receive nourishment via diffusion from the surrounding environment. The compressive forces that regularly act on cartilage also increase the diffusion of nutrients. This indirect process of receiving nutrients is a major factor in the slow turnover of the extracellular matrix and the lack of repair seen in cartilage.
Nerves
Cartilage does not contain nerves; it is aneural (see Image. Cartilage and Nerves).[6] If any pain is associated with a pathology involving cartilage, it is most commonly due to irritation of surrounding structures, such as inflammation of the joint and bone in osteoarthritis.
Muscles
Fibrocartilage is a major component of entheses, defined as the connective tissue between muscle tendon or ligament and bone. The fibrocartilaginous enthesis consists of 4 transition zones as it progresses from tendon to bone.[7] These transition zones are listed in order of progression from muscle to bone.
- Longitudinal fibroblasts and a parallel arrangement of collagen fibers are found in the tendinous area.
- A fibrocartilaginous region where the main type of cells present transitions from fibroblast to chondrocytes
- A region called the "blue line" or "tide mark" due to an abrupt transition from cartilaginous to calcified fibrocartilage.
- Bone
Physiologic Variants
Literature shows many anatomical variants of cartilage, and in many cases, this can affect the pathology associated with it. For example, a study showed a significant correlation between novel genetic variants in cartilage thickness and the incidence of hip osteoarthritis.[8]
Clinical Significance
An immense variety of clinical pathologies exist involving cartilage, such as osteoarthritis, spinal disc herniation, traumatic rupture/detachment, achondroplasia, costochondritis, neoplasm, and many others. These result from a variety of degenerative, inflammatory, and congenital causes.
Osteoarthritis is a disease affecting the whole joint; however, the articular cartilage (a subset of hyaline cartilage) within the joint is the most affected tissue. Osteoarthritis is known as a "wear and tear" phenomenon because it mainly affects joints under higher amounts of stress. It results in articular cartilage being thinned and wearing away. This ultimately results in a decreased range of motion, "bone against bone" contact within the joint, and pain. The initial clinical treatment is with anti-inflammatories and corticosteroid injections intraarticularly. Both therapies function to reduce the inflammatory reaction caused by the degenerative cartilage's release of cytokines. Patients may also show improvement by losing weight, exercising, and making efforts to decrease joint stress with rest and the use of a cane. Eventually, however, many patients will develop pain and symptoms that interfere with daily life. At this point, joint replacement or resurfacing may be recommended. Arthroscopic surgery is no longer recommended as it does not improve outcomes in knee osteoarthritis and can cause harm.
Another common degenerative disease of cartilage is spinal disc herniation. It is due to degenerative changes in the outer ring of the intervertebral disc, called the annulus fibrosus. The annulus fibrosus is composed of fibrocartilage. Trauma, straining, and lifting injuries are also implicated in the weakening of the annulus fibrosis predisposing to disc herniation. When there is structural damage to the annulus fibrosus, the nucleus pulposus within the disc may herniate into the spinal canal, causing impingement of 1 or multiple nerves and inducing inflammatory changes due to the damaged fibrocartilage.[9] History, symptoms, and physical examination make diagnosis. At some point in the evaluation, imaging studies are usually conducted to rule out other causes, such as tumors, spondylolisthesis, and space-occupying lesions. Although some patients warrant surgery due to the severity of symptoms, most cases do not require surgical intervention as they resolve with conservative measures such as anti-inflammatories and lifestyle changes for the patient.
In contrast to the degenerative diseases of cartilage, Achondroplasia is a genetic disorder of cartilage formation and is the most common cause of dwarfism. The pathology seen is due to a mutation on chromosome 4 affect the fibroblast growth factor receptor 3 (FGFR3) gene, which normally functions as a negative regulator of bone and cartilage growth. The mutation in achondroplasia results in a truncated dysfunctional protein that is constitutively active. These dysfunctional proteins impede cartilage growth and development by suppressing chondrocyte proliferation and calcification.[10] The diagnosis of achondroplasia is usually during pregnancy via prenatal ultrasound. There is currently no known cure for achondroplasia as it is not affected by a hormone pathway that can be pharmacologically manipulated, and corrective surgery is controversial.[11]
Media
(Click Image to Enlarge)
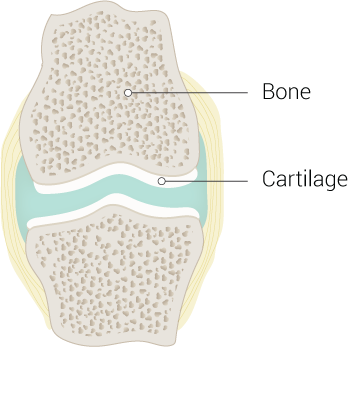
Cartilage and Bone Illustration
Contributed by B Palmer
(Click Image to Enlarge)
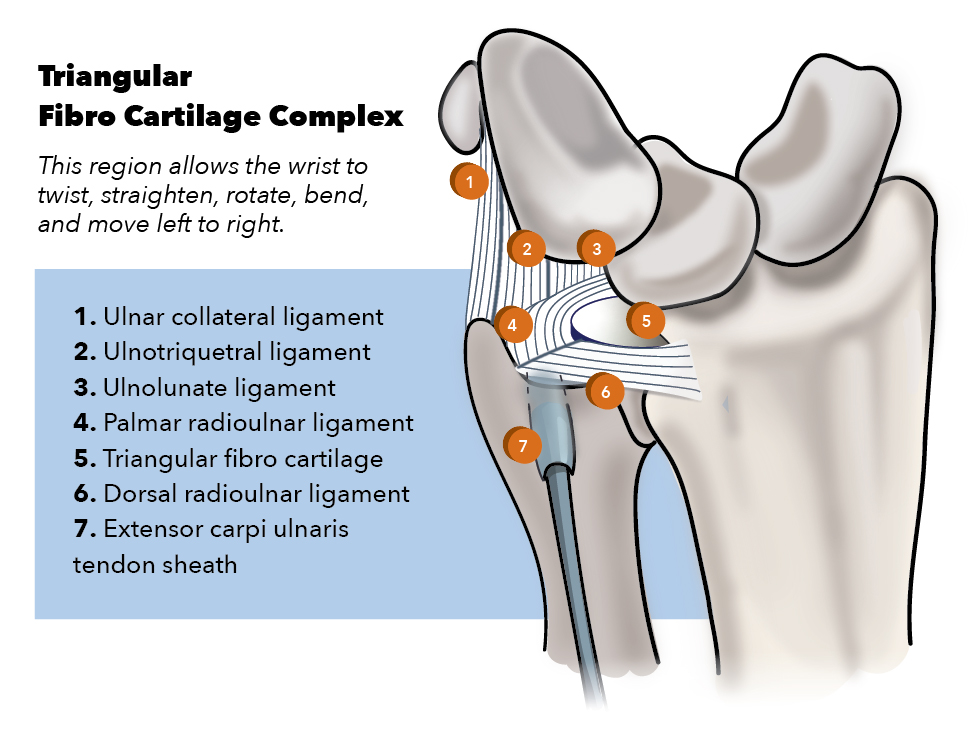
Triangular Fibrocartilage Complex. Parts of the complex include the ulnar collateral ligament, ulnotriquetral ligament, ulnolunate ligament, palmar (volar) and dorsal radioulnar ligaments, triangular fibrocartilage proper (articular disc), and extensor carpi ulnaris tendon sheath.
Contributed by K Humphreys
(Click Image to Enlarge)
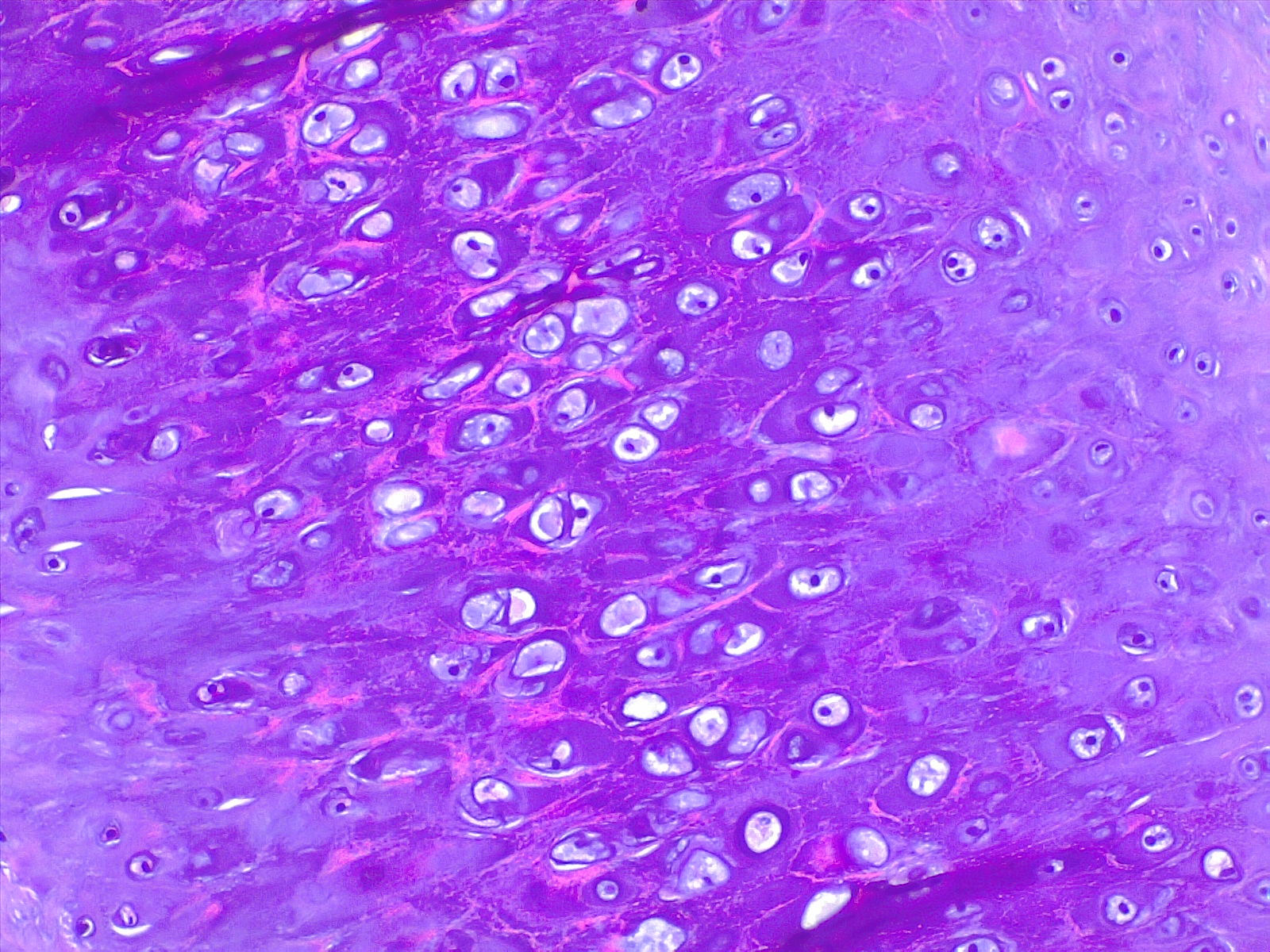
Cartilage. H/E 20× magnification.
Contributed by F Farci, MD
(Click Image to Enlarge)
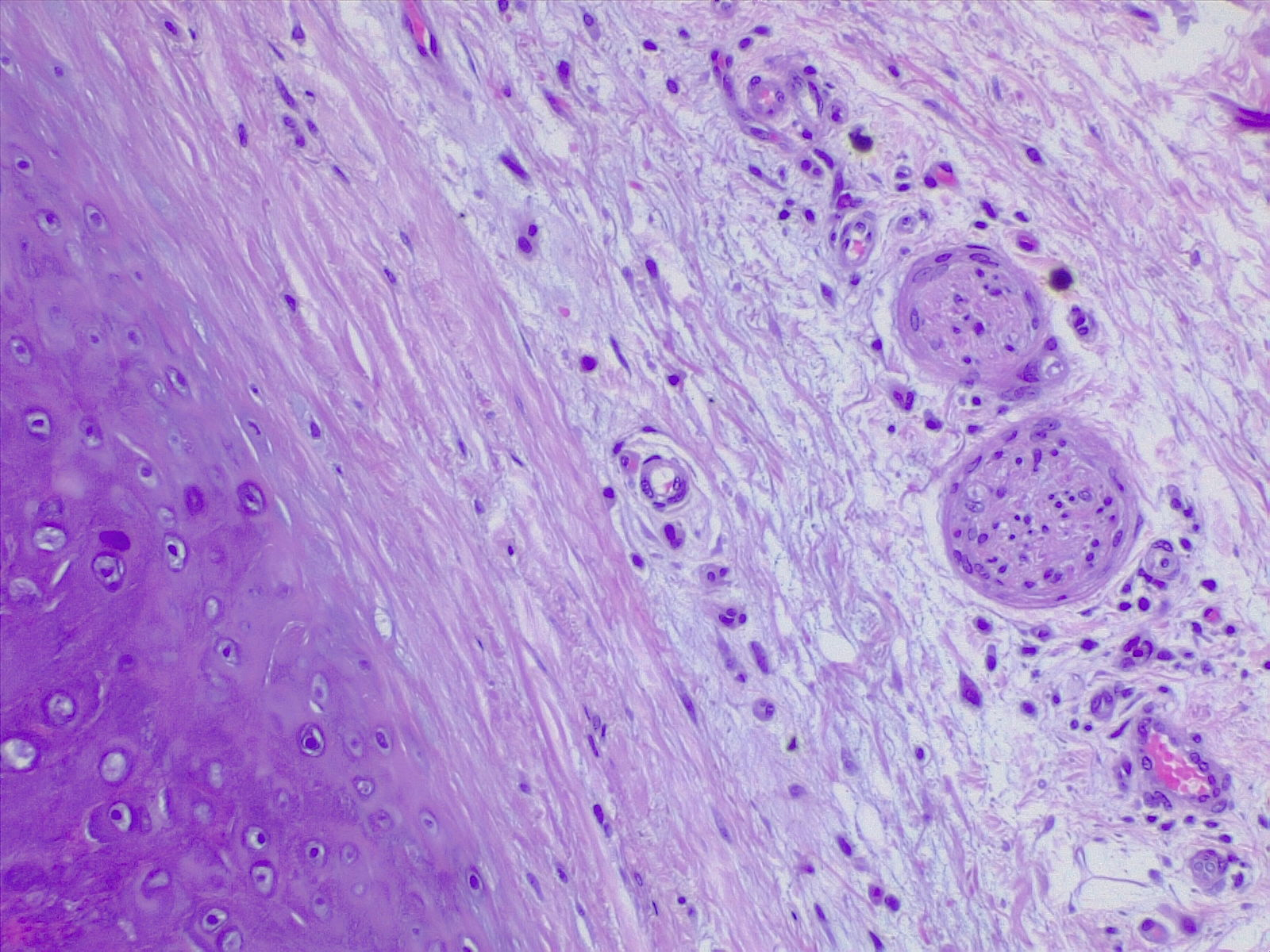
Cartilage and Nerves. H/E 4× magnification.
Contributed by F Farci, MD
References
Gupton M, Munjal A, Terreberry RR. Anatomy, Hinge Joints. StatPearls. 2024 Jan:(): [PubMed PMID: 30085509]
Loy BN, Zimel M, Gowda AL, Tooley TR, Maerz T, Bicos J, Guettler J. A Biomechanical and Structural Comparison of Articular Cartilage and Subchondral Bone of the Glenoid and Humeral Head. Orthopaedic journal of sports medicine. 2018 Jul:6(7):2325967118785854. doi: 10.1177/2325967118785854. Epub 2018 Jul 20 [PubMed PMID: 30046634]
Safshekan F, Tafazzoli-Shadpour M, Abdouss M, Shadmehr MB. Viscoelastic Properties of Human Tracheal Tissues. Journal of biomechanical engineering. 2017 Jan 1:139(1):. doi: 10.1115/1.4034651. Epub [PubMed PMID: 27618230]
Chen S,Fu P,Wu H,Pei M, Meniscus, articular cartilage and nucleus pulposus: a comparative review of cartilage-like tissues in anatomy, development and function. Cell and tissue research. 2017 Oct [PubMed PMID: 28413859]
Level 2 (mid-level) evidencevon der Mark K, von der Mark H. Immunological and biochemical studies of collagen type transition during in vitro chrondrogenesis of chick limb mesodermal cells. The Journal of cell biology. 1977 Jun:73(3):736-47 [PubMed PMID: 68959]
Level 3 (low-level) evidenceSofat N, Ejindu V, Kiely P. What makes osteoarthritis painful? The evidence for local and central pain processing. Rheumatology (Oxford, England). 2011 Dec:50(12):2157-65. doi: 10.1093/rheumatology/ker283. Epub 2011 Sep 27 [PubMed PMID: 21954151]
Jensen PT, Lambertsen KL, Frich LH. Assembly, maturation, and degradation of the supraspinatus enthesis. Journal of shoulder and elbow surgery. 2018 Apr:27(4):739-750. doi: 10.1016/j.jse.2017.10.030. Epub 2018 Jan 10 [PubMed PMID: 29329904]
Castaño-Betancourt MC, Evans DS, Ramos YF, Boer CG, Metrustry S, Liu Y, den Hollander W, van Rooij J, Kraus VB, Yau MS, Mitchell BD, Muir K, Hofman A, Doherty M, Doherty S, Zhang W, Kraaij R, Rivadeneira F, Barrett-Connor E, Maciewicz RA, Arden N, Nelissen RG, Kloppenburg M, Jordan JM, Nevitt MC, Slagboom EP, Hart DJ, Lafeber F, Styrkarsdottir U, Zeggini E, Evangelou E, Spector TD, Uitterlinden AG, Lane NE, Meulenbelt I, Valdes AM, van Meurs JB. Novel Genetic Variants for Cartilage Thickness and Hip Osteoarthritis. PLoS genetics. 2016 Oct:12(10):e1006260. doi: 10.1371/journal.pgen.1006260. Epub 2016 Oct 4 [PubMed PMID: 27701424]
Huang KY, Hsu YH, Chen WY, Tsai HL, Yan JJ, Wang JD, Liu WL, Lin RM. The roles of IL-19 and IL-20 in the inflammation of degenerative lumbar spondylolisthesis. Journal of inflammation (London, England). 2018:15():19. doi: 10.1186/s12950-018-0195-6. Epub 2018 Sep 18 [PubMed PMID: 30250404]
Merker A, Neumeyer L, Hertel NT, Grigelioniene G, Mäkitie O, Mohnike K, Hagenäs L. Growth in achondroplasia: Development of height, weight, head circumference, and body mass index in a European cohort. American journal of medical genetics. Part A. 2018 Aug:176(8):1723-1734. doi: 10.1002/ajmg.a.38853. Epub 2018 Aug 2 [PubMed PMID: 30070757]
Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, Gripp KW, Amemiya A, Legare JM. Achondroplasia. GeneReviews(®). 1993:(): [PubMed PMID: 20301331]