Introduction
Bone markings are crucial for identifying bones and understanding anatomy. These distinctive features benefit various professionals, including clinicians and forensic scientists. Bone markings are easily overlooked but serve essential functions like facilitating joint movement, locking bones in place, and supporting and protecting soft tissues.
Bone markings arise through a combination of genetic programming, mechanical stimuli, and adaptation to functional demands, resulting in a diverse array of features that serve various anatomical and physiological roles.[1][2] Bone markings hold significant importance in surgery as they serve as crucial landmarks for surgical procedures.[3] Surgeons rely on bone markings to guide incisions, identify anatomical structures, and navigate around critical areas such as nerves and blood vessels. On the other hand, maladaptive bony prominences can impair normal anatomical function and contribute to musculoskeletal dysfunction and pain. Understanding bone markings enables clinicians to evaluate and manage various musculoskeletal conditions.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Common Bone Markings
Common bone markings are distinctive features on bone surfaces that serve various anatomical, functional, and developmental roles. These markings provide essential reference points for understanding skeletal structure, identifying specific bones, and comprehending their interactions within the body (see Image. Labeled Bone Markings). The following are common bone markings:
- Angles: Sharp bony angulations that may serve as bony or soft tissue attachments but are often used for precise anatomical description. Examples include the scapula's superior, inferior, and acromial angles and the occiput's superior, inferior, and lateral angles.
- Body: The bone's largest, most prominent segment. Examples include the diaphysis or shaft of long bones like the femur and humerus.
- Condyle: Refers to a large prominence that provides structural support to the overlying hyaline cartilage. Condyles bear the brunt of the force exerted by a muscle about a joint. Examples include the knee, a hinge joint uniting the femoral lateral and medial condyles with the tibial lateral and medial condyles. The occiput also has an occipital condyle that articulates with the atlas (1st cervical vertebra or C1) and accounts for approximately 25° of cervical flexion and extension.[4]
- Crest: A bone edge's raised or prominent part. Crests provide sites for muscle and connective tissue attachments. The iliac crest is found on the ilium.
- Diaphysis: Refers to a long bone's shaft. Examples of long bones include the femur, humerus, and tibia.
- Epicondyle: A prominence superior to a condyle. The epicondyle provides muscle and connective tissue attachment sites. Examples include the femoral and humeral medial and lateral epicondyles.
- Epiphysis: The bone's articulating segment, usually at the bone's proximal and distal poles. The epiphysis typically has a larger diameter than the diaphysis. This segment is critical to bone growth, as it sits adjacent to the physeal line (growth plate).
- Facet: A facet is a smooth, flat surface that forms a gliding joint with another flat bone or facet. Examples may be seen in the vertebrae's facet joints, which allow for spinal flexion and extension.
- Fissure: An open slit in a bone that usually houses nerves and blood vessels. Examples include the skull's superior and inferior orbital fissures.[5]
- Foramen: A hole through which nerves and blood vessels pass. Examples include the supraorbital, infraorbital, and mental foramina in the cranium.[6]
- Fossa: A shallow depression on the bone surface, which may receive an articulating bone or act to support soft tissue structures. Examples include the trochlear and the posterior, middle, and anterior cranial fossae.
- Groove: A furrow on the bone surface that houses long blood vessel or nerve segments for protection against compression by adjacent structures (see Image. Anterior Surface of Clavicle). Examples include the radial and transverse sinus grooves.
- Head: A rounded, prominent, bony extension that forms part of a joint. The head is separated from the bone shaft by the neck. The head is usually covered in hyaline cartilage and a synovial capsule. This part comprises a bone's main articulating surface in ball-and-socket joints. An example is the femoral head in the hip joint.
- Margin: A flat bone's edge. Margins may be used to define a bone's borders accurately. For example, the part of the temporal bone articulating with the occipital bone is called the "occipital margin" of the temporal bone." Similarly, the part of the occipital bone articulating with the temporal bone is called the occipital bone's "temporal margin."
- Meatus: A tube-like channel that extends within the bone, which may provide passage and protection to nerves and vessels. The external and internal acoustic meatus accommodate sound transmission (see Image. External Ear, Horizontal Section).
- Neck: The segment between a bone's head and shaft. This part is often demarcated from the head by the physeal line in pediatric patients and physeal scar (or physeal line remnant) in adults. The neck is often separated into surgical and anatomical necks. The anatomical neck, representing the old epiphyseal plate, is often demarcated by its attachment to capsular ligaments. The surgical neck is often more distal than the anatomical neck and is a commonly fractured location. For example, the humeral anatomical neck runs obliquely from the greater tuberosity to the humeral head's inferior aspect. The surgical neck runs horizontally and a few centimeters distal to the humeral tuberosities.
- Notch: A bony depression that often, but not always, stabilizes an adjacent articulating bone. The articulating bone slides into and out of the notch, which guides the joint's range of motion. Examples include the ulna's trochlear and radial notches and the suprasternal and mandibular notches.
- Ramus: The curved part of a bone that gives structural support to the rest of the bone. Examples include the superior and inferior pubic and mandibular rami.
- Sinus: A hollow cavity housing air, fluid, or blood. Examples include paranasal and dural venous sinuses.
- Spinous process: A raised, sharp bony elevation where muscles and connective tissues attach. Spinous processes are more pronounced than other bony processes (see Image. Lumbar Vertebral Anatomy).
- Trochanter: A large prominence on one side of a bone. Some of the largest muscle groups and most dense connective tissues attach to the trochanter. The most notable examples are the femur's greater and lesser trochanters.
- Tuberosity: A moderate prominence where muscles and connective tissues attach. Tuberosities function similarly to trochanters. Examples include the tibial, deltoid, and ischial tuberosities.
- Tubercle: A small, rounded prominence where connective tissues attach. Examples include the greater and lesser humeral tubercles.
Bone Markings in the Upper Limb
The upper limb is involved in a wide range of movements essential for daily activities and physical function. Thus, the upper limb's bone markings are particularly relevant for clinical and anatomical study.
Scapula
The scapula serves as the upper limb's mobile platform. One can think of this bone as a massive construction crane with jacks that anchor the cab to the ground, like how muscles and connective tissues attach the scapula to the body. The crane also has a long, mobile arm, resembling the upper limb. The scapula has medial, lateral, and superior borders. The inferior pole is the junction of the medial and lateral borders.
The dorsal scapular surface contains the bone's prominent spine. The trapezius inserts on the scapular spine. The deltoid muscle arises from the scapular spine's lateral aspect, the acromion, and the lateral clavicle.[7] The supraspinous fossa above the scapular spine is the supraspinatus muscle's origin. This muscle inserts on the greater humeral tubercle's “S” facet (see below). The infraspinous fossa below the scapular spine is where the infraspinatus muscle originates. This muscle inserts on the “I” (middle) facet of the greater humeral tubercle.
The acromion (acromial process) lies at the scapular spine's lateral end. The acromial process is one of the deltoid muscle's proximal insertion sites. The deltoid is a triangular muscle named after the capital Greek letter delta. The scapula's medial border is an insertion site for the rhomboid minor and major muscles. The teres minor originates from the scapula's lateral border, while the teres major arises from the inferior scapular angle.
The scapula's anterior surface contains the prominent coracoid process, which resembles a crow’s beak. This process acts as a pectoralis minor attachment point. The coracoid process is also where the biceps brachii's short head and coracobrachialis muscles arise. The subscapular fossa houses the subscapularis' proximal insertion point. The subscapularis distally inserts on the lesser humeral tubercle.
The glenoid fossa receives the humeral head at the scapulohumeral articulation or shoulder joint (see Image. Scapula, Lateral View).[8]
Humerus
The humerus is the arm bone (see Image. Upper Arm Anatomy). The greater and lesser tubercles lie on the superior aspect of this bone. The greater tubercle is located laterally and has 3 prominent facets termed the “S,” “I,” and “T” facets. The superior or "S" facet serves as the distal insertion site for the supraspinatus muscle, which initiates arm abduction. The muscle acts as the primary arm abductor for the first 15° to 20° of abduction. The deltoid becomes the primary abductor beyond this angle. The middle or "I" facet houses the infraspinatus insertion site. This muscle is a lateral arm rotator. The lower or "T" facet contains the teres minor insertion point. The teres minor is another lateral arm rotator.[9]
The lesser humeral tubercle contains the subscapularis muscle's distal insertion point. The subscapularis is a major arm adductor, preventing arm dislocation at the shoulder.[9]
The humeral midshaft's lateral surface exhibits the deltoid tuberosity, the deltoid insertion site. This muscle abducts the arm beyond the first 15° to 20°. The deltoid's anterior fibers rotate the arm medially, while the posterior fibers laterally rotate the arm.[10]
The humeral midshaft's posterior aspect demonstrates the radial spiral groove, which ordinarily lies between the triceps brachii's lateral and medial heads. This groove transmits the radial nerve and profunda brachii artery.
The arm bone's inferior aspect contains the lateral and medial epicondyles. The lateral supracondylar ridge, which contains the proximal insertion point of the brachioradialis and extensor carpi radialis longus, flows into the lateral epicondyle. The lateral epicondyle is a bony prominence where the extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris originate.
The olecranon fossa lies on the arm bone's posterior aspect between the lateral and medial epicondyles. This region receives the ulna's olecranon process at the elbow joint. The distal humeral articulating surfaces include the laterally located capitulum (Latin for "little head") and the trochlea (Greek for "pulley").[11]
Radius
The head comprises the proximal radial end and articulates with the capitulum, allowing rotation for supination (palm up) and pronation (palm down). This mobility, while beneficial, makes the radius susceptible to dislocation, as in "nursemaid's elbow." The radial tuberosity serves as an insertion site for the biceps brachii. The radial shaft leads to the large styloid process at the distal end, where the brachioradialis muscle inserts. The radius articulates with the scaphoid and lunate at the radiocarpal joint.[12]
Ulna
The proximal ulnar end contains the coronoid process, which articulates with the humeral trochlea. This articulation is strong, only permitting flexion and extension. The ulnar tuberosity is where the brachialis muscle distally inserts. This muscle is a pure forearm flexor.[13] The distally located ulnar head articulates with the radius.
Wrist bones, metacarpals, and fingers
The 8 carpal bones are divided into proximal and distal rows. The proximal wrist bones articulate with the radius. The proximal row includes the scaphoid, which resembles the prow of a ship and articulates with the trapezium distally. The trapezium then connects to the 1st metacarpal bone that supports the thumb. Moving from lateral to medial, the proximal row continues with the lunate (resembling the moon), triquetrum (which has 3 corners), and the rounded pisiform. The pisiform can be palpated on the hand's anterior aspect. This bone moves with hand motion, confirming its location within the wrist rather than the forearm.
The distal carpal row starts with the laterally located trapezium (which resembles a 4-sided figure with 2 parallel sides), articulating with the thumb and index finger metacarpals. Medial to the trapezium is the trapezoid, shaped similarly to the trapezium, and capitate, the largest wrist bone. The hamate is medially located and features a prominent hook. The Guyon canal is the space between the pisiform and the hamate's hook that transmits the ulnar nerve. A hamate hook fracture can damage this nerve.
The 14 finger bones are known as the phalanges, a term derived from the military formation "phalanx." Each finger has 3 phalanges, except the thumb, which has 2. Finger movements include flexion (forward), extension (backward), abduction (finger separation), and adduction (fingers coming together). Metacarpal bones, 1 for each finger, connect the wrist bones to the fingers. The thumb's carpometacarpal articulation is rotated 90° compared to the other fingers, allowing flexion and extension along the plane of the hand. Abduction leads the thumb away from the palm, while adduction brings it toward the palm.[14]
Bone Markings in the Lower Limb
The lower limb bone markings serve as attachment sites for muscles, ligaments, and tendons, influencing joint stability and function important for weight-bearing and ambulation. Lower limb bone markings aid healthcare professionals in diagnosing injuries, planning surgical procedures, and guiding rehabilitation efforts.
Hip bone
The hip bone (innominate bone), consisting of the ilium (superior), ischium (posteroinferior), and pubis (anteroinferior), forms a sturdy basin that supports the trunk and provides attachment for lower limb muscles and ligaments. The iliac crest is located along the superior iliac border and acts as a thoracoabdominopelvic, hip, and thigh muscle attachment site. The acetabulum is a deep socket formed by the fusion of the 3 hip bones that receives the femoral head to form the hip joint. The greater sciatic notch on the ilium's posterior aspect allows for the sciatic nerve's passage. The inferoposteriorly located ischial tuberosity is an important weight-bearing structure that also acts as a hip and thigh muscle attachment site. The pubic symphysis is a fibrocartilaginous joint (secondary cartilaginous joint) that unites the pubic bones and stabilizes the hip.[15]
Femur
As the body's longest and strongest bone, the femur (thigh bone) transmits the upper body's weight to the lower limbs when standing and ambulating. The proximal femoral end features the femoral head, articulating with the hip's acetabulum to form the hip joint. The femoral neck unites the head to the shaft and is a common fracture site, particularly in older individuals. The greater and lesser trochanters act as attachment points for hip and thigh muscles. The intertrochanteric line and crest provide additional hip and thigh muscle attachment areas. The linea aspera is a ridge on the posterior surface of the femoral diaphysis that acts as an attachment site for various muscles, including the adductor magnus and vastus lateralis.[16]
Patella
The patella (kneecap) is a sesamoid bone embedded within the quadriceps tendon. This bone forms crucial articulations primarily with the femur and tibia, which are vital in knee stability and motion. The patella glides over the femoral condyles at the patellofemoral joint during flexion and extension.[17]
Tibia
The tibia is the stronger and larger of the 2 leg bones. This bone significantly contributes to weight-bearing and serves as an attachment site for thigh, leg, and extrinsic foot muscles. The tibia's proximal end features medial and lateral condyles, which unite with the femoral condyles to form the knee joint. The tibial tuberosity on the anterior diaphyseal surface provides an attachment site for the patellar ligament. The tibial shaft is relatively flat on its anterior surface, essential for protecting the underlying structures, including the anterior tibial vessels, deep fibular nerve, and leg extensor tendons. The medial malleolus at the distal end forms the prominence of the ankle's inner aspect and provides stability to the ankle joint.[18]
Fibula
The fibula is thinner and more slender than the tibia. This bone does not bear weight, though it provides stability to the ankle joint and is an attachment site for leg and extrinsic foot muscles. The fibular head articulates with the tibia, contributing to the stability of the proximal tibiofibular joint. The lateral malleolus at the fibula's distal end forms the prominence of the ankle's outer aspect and provides additional ankle stability.[19]
Tarsals, metatarsals, and phalanges
The foot consists of multiple bones arranged in intricate arches to support body weight and facilitate movement. The tarsal bones, including the calcaneus, talus, navicular, cuboid, and cuneiforms, form the proximal part of the foot and provide stability and flexibility. The metatarsals, numbered 1 through 5 from medial to lateral, articulate with the tarsal bones proximally and the phalanges distally. The phalanges, similar to those in the hand, consist of proximal, middle, and distal phalanges. The big toe (hallux) has only 2 phalanges. The metatarsophalangeal and interphalangeal joints allow for movement and flexibility during walking and running.[20]
Bone Markings in the Axial Skeleton
The axial skeleton forms the human body's central axis and is comprised of the skull, vertebral column, ribs, and sternum. Numerous bone markings in this region serve diverse anatomical, biomechanical, and clinical functions.
Skull
The craniofacial bones exhibit various markings. The superior orbital fissure lies between the lesser and greater sphenoid wings. The inferior orbital fissure is situated between the maxilla, zygomatic bone, and greater sphenoid wing. The cranial base exhibits various foramina, including the cribriform, anterior and posterior ethmoidal, and jugular foramina (see Image. Skull Base and Foramina). Paranasal sinuses, such as the maxillary sinus, are hollow cavities in craniofacial bones (see Image. Paranasal Sinuses). The transverse sinus groove on the occipital bone's inner surface runs horizontally near the tentorium cerebelli attachment.
The cranial fossae include the anterior, middle, and posterior cranial fossae, which are cranial base depressions supporting the brain, cranial nerves, and head and neck blood vessels. The occipital condyle articulates with the cervical atlas, contributing to the stability and mobility of the head and neck. The temporal bone's external and internal acoustic meatus accommodate sound transmission.
The mandibular body is the bone's horizontal portion that forms the lower jawline. Rami are vertical mandibular extensions on each side, consisting of the ascending ramus and the condylar and coronoid processes. The condylar process connects with the temporal bone to form the temporomandibular joint (see Image. Pterygoids). The coronoid process provides an attachment site for the mastication muscles.
The angle of the mandible is where the mandible body meets the ramus, forming a distinct corner or angle. The mandibular notch (sigmoid notch) is a depression between the condylar and coronoid processes on the ramus' superior border. The mandibular foramen on the ramus' internal surface transmits the inferior alveolar vessels and nerves, supplying the lower teeth and the mandible. The mandibular symphysis is where the 2 halves of the mandible fuse anteriorly at the midline.[21]
Vertebral column
Each vertebra has a body, the main segment that provides structural support. Facet joints between adjacent vertebrae allow spinal flexion and extension. Intervertebral foramina enable thoracic nerves and blood vessels to pass between adjacent vertebrae. The vertebral neck is the segment between the body and vertebral processes. Intervertebral notches on the superior and inferior aspects of adjacent vertebrae form the intervertebral foramina, where spinal nerves traverse from the cord to the body. Spinous processes are raised bony elevations where trunk muscles and connective tissues attach.[22]
Ribs
The rib has superior and inferior angles where the rib curves. These structures also serve as trunk muscle and ligament attachment sites. Ribs also have superior and inferior crests, which are raised edges for thoracic muscle and connective tissue attachment. The body is the rib's main segment. The costal grooves inside the ribs provide passage for intercostal vessels and nerves, supporting thoracic function.
Ribs have facets on their heads that articulate with the thoracic vertebrae, forming the costovertebral joints. The head of the rib is a rounded, prominent extension that articulates with the thoracic vertebrae. Costal margins define rib borders and serve as thoracic muscle attachment sites. The rib's neck is the segment between the head and the body. Costal notches articulate with the vertebrae or sternum. Ribs have articular and nonarticular tubercles, the latter serving as trunk muscle attachment points.[23]
Sternum
The sternomanubrial angle (or sternal angle or angle of Louis) is the junction between the manubrium and sternal body (see Image. Sternum Anatomy). This angle is palpable as a slight elevation and serves as a landmark for locating the 2nd rib and the T4-T5 intervertebral disk. The sternal body (or gladiolus or gladiolus sterni) is the sternum's largest and central segment. The sternal margins provide attachment points for the ribs' costal cartilages. The jugular notch (suprasternal notch) is a U-shaped depression at the sternum's superior aspect, serving as a palpable landmark for anatomical reference and facilitating the identification of cervical structures. Clavicular notches on the manubrium's superior border articulate with the clavicles.[24][25]
Embryology
Skeletal development and bone ossification commence with mesenchymal cell aggregation into condensed structures, serving as the initial foundation for bone formation. The process starts around the 6th to 7th weeks of embryonic growth and involves intramembranous and endochondral ossification. Intramembranous ossification directly converts mesenchymal tissue into bone, forming flat bones like the skull and scapula. Endochondral ossification begins with mesenchymal tissue transforming into intermediate cartilage, eventually replaced by bone, contributing to the formation of long bones and the axial skeleton.[26]
Intramembranous ossification begins with osteoblast differentiation from mesenchymal cells, forming clusters that establish ossification centers. Osteoblasts secrete osteoid within these centers, mineralizing it to form woven bone, which later transforms into compact bone. Endochondral ossification occurs within hyaline cartilage and involves chondrocyte differentiation from mesenchymal cells, leading to the secretion of extracellular matrix and establishment of a cartilage framework for bone formation. Transcription factors like RUNX2 and SOX-9 regulate the process and play a critical role in bone development and fracture healing.
Appositional growth, driven by osteoblasts from periosteum and endosteum osteoclasts, contributes to the circumferential enlargement of long bones. Bone remodeling, a dynamic process throughout life, involves bone formation and resorption, influenced by various factors like age, genetics, hormones, and physical activity. The Wolff Law describes how bone contours reflect forces, with articulating features developing from articulating surfaces and protuberances from connective tissue and muscle traction forces. These events shape bone markings early in embryologic development and continue into early adulthood. Bone remodeling maintains bone health and balance, which is crucial for sustaining mature and resilient bone tissue.[27]
Blood Supply and Lymphatics
Blood vessels permeate bone tissue, except in cartilaginous regions like the growth plate. Arteries supply oxygenated blood to bones, while veins carry blood away, connected by capillary networks. Long bones such as the tibia and femur feature various artery types, including the principal nutrient artery, which splits into ascending and descending central arteries, supplying the medulla and cortical layers.[28] Additionally, periosteal and Haversian arteries traverse the bone's outer and cortical surfaces, respectively, with Volkmann arteries acting as bridges between these vessels.[29] Veins exit bones via periosteal veins, and epiphyseal and metaphyseal arteries supply blood to bone ends. Flat bones like cranial bones are perfused primarily by periosteal arteries, while irregular bones like the mandible have complex vascular arrangements.
The bone capillary network fills the marrow cavity, predominantly comprising dense, fenestrated, and branched sinusoidal vessels. Linear columnar vessels predominate in the metaphysis and endosteum, interconnected by loops or arches. These vessels drain into a central vein in long bone diaphyses, with smaller veins branching off to periosteal veins. Type H vessels, expressing markers like endomucin and CD31, exhibit higher oxygen levels and blood velocity due to direct arteriolar connections, influencing tissue microenvironments. Various cell types surrounding blood vessels, like pericytes and stromal cells, show distinct characteristics depending on the vessel type and share similarities with mesenchymal progenitor cells, suggesting a role in tissue repair. These cells contribute to bone lineage during development and adulthood, supporting diverse cellular environments within bone tissue.
Transcortical vessels traverse cortical bone, providing direct arteriovenous connections in the endosteum. The distribution and heterogeneity of perivascular cells in bone contribute to tissue homeostasis and repair. Different cell types associated with specific vessel subtypes, such as Nestin-expressing cells around type H vessels and LepR-expressing cells near type L vessels, exhibit multilineage potential. These cells contribute to bone marrow stroma, hematopoiesis, and adipogenesis, playing crucial roles in bone health and repair. Additionally, recent studies highlight the role of new adipogenic lineage cells called "marrow adipogenic lineage precursors" in maintaining marrow vasculature and modulating bone formation.[30]
Nerves
Steverink et al's study reveals that nerve fiber distribution within the bone and bone-related compartments contain innervation density and fiber type variations. The periosteum harbors greater nerve fiber density, particularly A∂, C, and sympathetic nerve fibers, than cortical bone and bone marrow. Periosteal and bone marrow sensory fibers form large bundles, while cortical bone predominantly contains single fibers confined to Haversian canals. Sympathetic fibers are colocalized with blood vessels in all compartments, suggesting a role in vascular regulation. Confocal imaging of periosteal whole-mount samples illustrates a branched network of nerve fibers, indicating extensive innervation throughout the periosteum, particularly around blood vessels.
The periosteum exhibits similar quantities of A∂ and C fibers. In contrast, cortical bone and bone marrow contain more C than A∂ fibers. Sympathetic nerve fibers outnumber A∂ and C fibers in all compartments, indicating the prevalence of sympathetic innervation throughout bone tissue.[31]
Peripheral nerves play a crucial role in bone mechanosensing and adaptation to mechanical stimuli, as demonstrated by studies utilizing perineural anesthesia and sensory nerve signaling modulation. However, the role of the sympathetic nervous system in the anabolic bone response to mechanical loading remains uncertain. In disuse conditions, such as immobilization or peripheral nerve dysfunction, peripheral nerve activity may modulate bone resorption responses, suggesting a regulatory role for sensory nerves in bone volume maintenance. Sympathetic nerves have also been implicated in modulating unloading-induced (eg, immobilization-related) bone loss, with studies reporting both inhibitory and activating effects of sympathetic nerve modulation on bone formation and resorption.[32]
Muscles
Muscles are crucial in forming bone markings, as they exert traction forces on bones at their attachment sites. These forces stimulate bone growth and remodeling, resulting in the development of various protuberances such as crests, trochanters, tuberosities, and tubercles, which serve as muscle attachment points. The bone markings' sizes and shapes indicate the magnitude and direction of the forces applied by the associated muscles. Additionally, articulating features of bones, like facets, condyles, and heads, develop in response to the articulating surfaces between 2 bones, further influenced by muscle action and joint movement. Overall, the interaction between muscles and bones during movement and physical activity shapes the structural characteristics of bones, reflecting functional demands.
Surgical Considerations
Bone markings are significant to physicians and surgeons, serving as anatomic landmarks that give information about the surrounding structures. For example, an anesthesiologist will inject medial and posterior to the ischial spine to achieve a pudendal nerve block. Alternatively, bone markings like the femur's adductor tubercle give valuable information about the muscles within the surgeon's view.[33][34]
Clinical Significance
Uses of Bone Markings
Nearly all medical providers use bony landmarks to approximate injection sites, localize the targeted tissue, or guide medical imaging. Spinous processes are palpated and used as anatomic guides during epidural steroid injections or lumbar punctures (spinal tap). Tibial and femoral condyles are palpated to approximate the meniscal sites during the McMurray test, which evaluates the menisci's structural integrity. Bony landmarks of the elbow are used to orient the operator and locate areas of interest for targeted medical imaging like ultrasound. These applications underscore the importance of these osteological features.
Nursemaid’s Elbow
Nursemaid's elbow, also known as radial head subluxation, typically occurs in young children when a sudden traction force on the extended arm causes the radius to partially dislocate from the annular ligament. The patient holds the affected arm in a flexed and pronated position, demonstrating pain and reluctance to use the arm. The condition can impair arm supination.[35]
Greater Humeral Tubercular Fracture
Fracture of the greater humeral tubercle damages the insertions of the supraspinatus (“S” facet), infraspinatus (“I” facet), and teres minor (“T”) facet. Supraspinatus weakness impairs arm abduction. This condition may be tested by holding the patient’s arm and having them initiate abduction against resistance. The more powerful deltoid muscle can abduct the arm past the supraspinatus' range (15° to 20° degrees). Without testing against resistance, the patient may bump the arm enough to appear to be able to abduct it completely. Having the patient abduct the arm against resistance reveals the deficit. Lateral arm rotation weakness due to infraspinatus and teres minor impairment may be observed. However, the stronger posterior fibers of the deltoid muscle can compensate. Another injury indicator is pain experienced upon palpation of the greater tubercle.[36][37].
Lesser Humeral Tubercular Fracture
Fracture of the lesser tubercle of the humerus may damage the subscapularis insertion. Arm adduction and medial rotation subsequently weaken. Pain often worsens upon lesser tubercle palpation.[38][39][40]
Humeral Surgical Neck Fracture
Fracture of the humeral surgical neck damages the axillary nerve, weakening the deltoid and teres minor. The axillary nerve terminates as the arm's upper lateral cutaneous nerve. Injury to this nerve may cause pain or anesthesia over the proximal lateral arm region.[41][42]
Lateral Epicondylar Fracture
This injury damages the radial nerve, which innervates the forearm and hand extensors. Radial nerve injury produces a wrist drop or the inability to extend the hand. Testing involves flexing the forearm in a pronated position, with the examiner holding the forearm and hand dorsum. The patient is then instructed to extend the fingers against resistance.[43]
Medial Epicondylar Fracture
This condition damages the ulnar nerve, resulting in forearm flexion weakness and radial deviation of the wrist's medial side. A “claw hand” may also develop, with the 3rd and 4th fingers flexed due to impairment of the 3rd and 4th lumbricals and the interossei. Sensory loss over the hand's medial 1-1/2 side may also be observed.[44][45]
Hamate Hook Fracture
Fracture of the hook of the hamate causes swelling in the surrounding soft tissue that can compress the ulnar nerve at the Guyon canal. Muscles that may weaken include the abductor, flexor, and opponens digiti minimi, the 3rd and 4th lumbricals, interossei, and adductor pollicis brevis. Palpation of the pisiform and hook of the hamate bone produces pain. To test adductor pollicis weakness, the patient may be instructed to hold a piece of paper or the examiner's index finger tightly without letting it slip. Ulnar nerve injury weakens this muscle, leading to the inability to maintain the grip and compensatory flexion of the thumb's distal phalanx, known as the Froment sign.[46][47][48]
Scaphoid Fracture
The scaphoid is located in the depths of the anatomical snuffbox, formed by the tendons of the abductor pollicis longus and extensor pollicis longus anteriorly and the tendon of the extensor pollicis longus posteriorly. A scaphoid injury produces pain, tenderness, and bruising over the anatomical snuffbox. Palpation over this area worsens the pain. The injury may not be detected on radiography until a week postinjury. The wrist should be splinted to prevent displacing the fractured scaphoid. Allowing the fractured scaphoid segment to move freely may cause nonunion, which may become permanent due to the area's poor vascularity.[49][50][51]
Femoral Neck Fracture
Fractures of the femoral neck are common in older adults and can lead to significant morbidity and mortality. Other risk factors for femoral neck fractures include female sex, lower body mass index (<18.5), reduced bone mineral density, smoking, poor nutrition, medications, and sedentariness. Complications of these injuries include avascular necrosis, nonunion, malunion, posttraumatic arthritis, and loss of mobility and function.[52][53]
Iliotibial Band Syndrome
The iliotibial band inserts onto the lateral tibial condyle. Repetitive friction over this bony prominence during activities like swimming or cycling can lead to inflammation and lateral knee pain. This condition, known as iliotibial band syndrome, often presents as lateral knee pain aggravated by repetitive flexion and extension.[54]
Jumper's Knee
Patellar tendonitis or jumper's knee involves patellar tendon inflammation. Excessive stress on this attachment site at the tibial tuberosity, such as during repetitive jumping or running, can lead to pain, swelling, and tenderness over the tibial tuberosity.[55]
Medial Tibial Stress Syndrome
Shin splints involve tibial periosteal inflammation, particularly along the medial border where muscles attach. Medial stress syndrome arises from repetitive stress on the tibial attachment sites of leg muscles, eg, the tibialis posterior and soleus, presenting with pain and tenderness along the tibia's medial aspect.[56]
Achilles Tendinopathy
The Achilles tendon insertion onto the calcaneus (heel bone) is vulnerable to inflammation and degeneration, a condition known as Achilles tendonitis. This disorder commonly affects athletes involved in running or jumping sports and can manifest as pain, swelling, and stiffness at the back of the heel.[57]
Atlantoaxial Instability
Various ligaments and bony structures stabilize the atlantoaxial joint (C1-C2 joint), including C2's odontoid process (dens). Pathologies such as rheumatoid arthritis, trauma, or congenital abnormalities can lead to atlantoaxial instability, where excessive movement between C1 and C2 occurs. The condition can result in the compression of the spinal cord or surrounding nerves and produce neurological deficits, neck pain, and potentially life-threatening complications.[58]
Temporal Bone Fracture
The temporal bone contains several notable landmarks, including the mastoid process and external auditory meatus. Temporal bone fractures typically result from significant head trauma, such as motor vehicle crashes or falls from height. These injuries can disrupt the integrity of the middle and inner ear structures, potentially leading to hearing loss, vertigo, facial nerve paralysis (Bell palsy), or cerebrospinal fluid leakage.[59]
Cervical Rib
A cervical rib is an additional rib that arises from C7 and may extend to T1.[60] This anatomical variation can compress nearby nerves and blood vessels, leading to thoracic outlet syndrome. Symptoms include pain, numbness, upper extremity weakness, arm swelling, and discoloration.[61]
Spinous Process Fracture
Trauma or repetitive stress can lead to spinous process fractures. These injuries most frequently affect the vertebral column's thoracic and lumbar regions. Falls, motor vehicle collisions, and sports injuries are the usual causes. Symptoms include localized pain, tenderness, and restricted spinal mobility.[62]
Sternal Fracture
Sternal fractures commonly arise from blunt chest trauma, eg, from motor vehicle accidents or direct blows to the chest. Fractures may involve the manubrium, body, or xiphoid process and may produce severe chest pain, difficulty breathing, and potential damage to underlying structures such as the heart or lungs.[63]
Media
(Click Image to Enlarge)
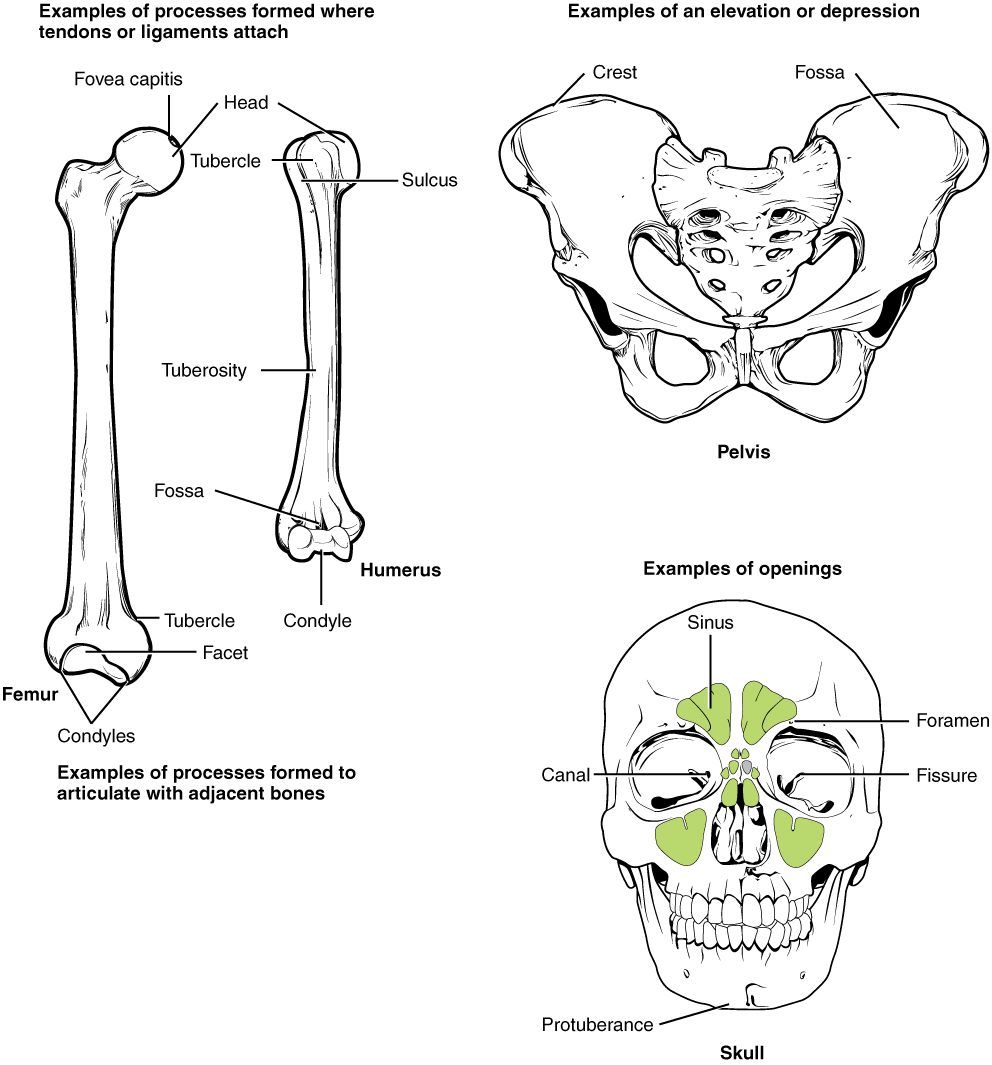
Labeled Bone Markings. This image illustrates bone markings on the femur, innominate bone, and skull.
Contributed by Anatomy & Physiology, Connexions Web site. http://cnx.org/content/col11496/1.6/ (CC BY 3.0 https://creativecommons.org/licenses/by/3.0/deed.en)
(Click Image to Enlarge)
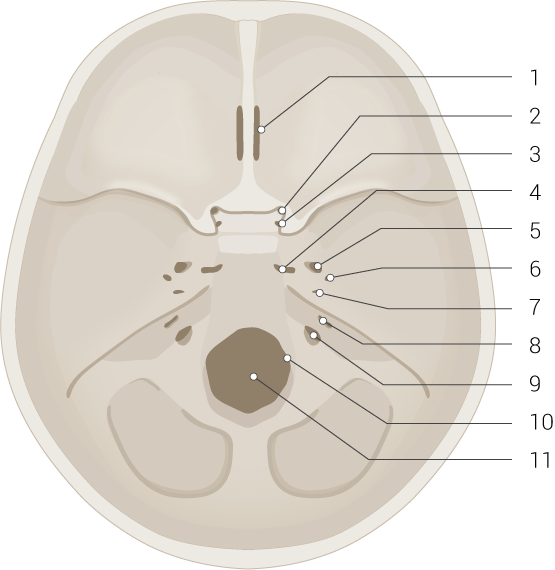
Skull Base and Foramina. This illustration shows the cribriform plate of the ethmoid bone (1), optic canal (2), foramen rotundum (3), foramen lacerum (4), foramen ovale (5), foramen spinosum (6), carotid canal (7), internal acoustic meatus (8), jugular foramen (9), hypoglossal canal (10), and foramen magnum (11). The anterior (foramen 1), middle (foramina 2-7), and posterior cranial fossae (foramina 8-11) are also shown but not labeled.
Illustrated by B Palmer
(Click Image to Enlarge)
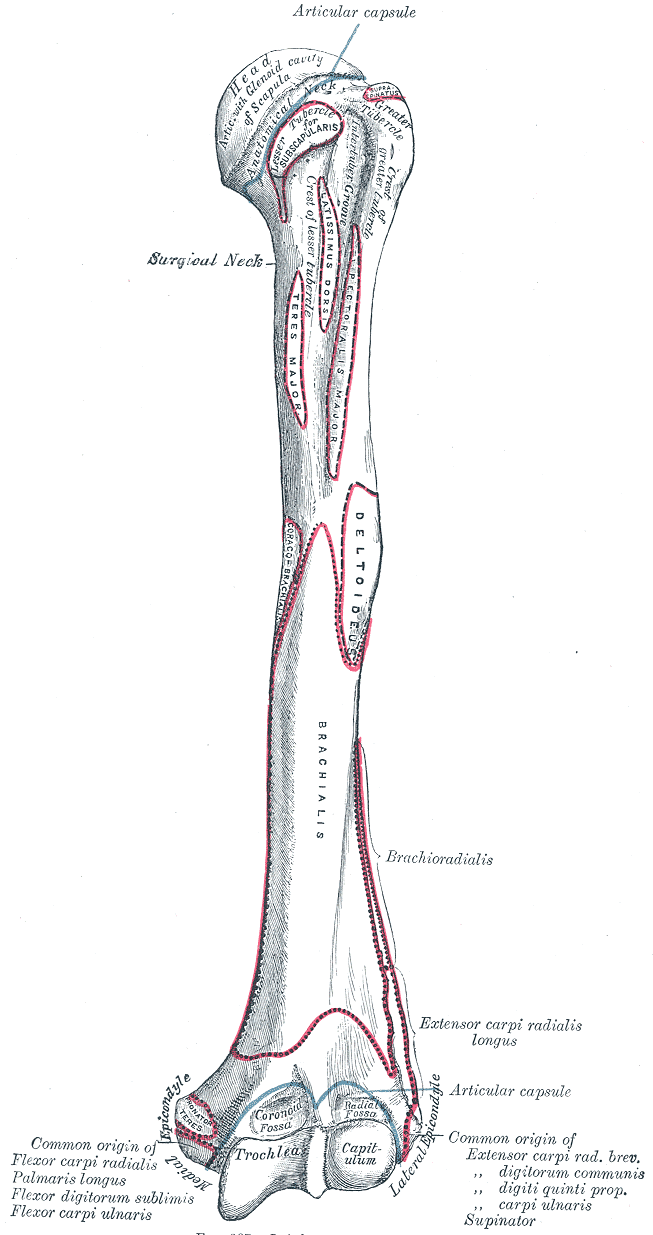
Upper Arm Anatomy. This illustration details the humerus and various attachment sites on its surface. Shown are the head, surgical and anatomical necks, greater and lesser tubercles, crest of lesser tubercle, intertubercular groove, trochlea capitulum, radial and coronoid fossae, lateral and medial epicondyles, and attachment sites for the subscapularis, coracobrachialis, teres major, latissimus dorsi, pectoralis major, deltoid, brachialis, forearm extensors and flexors, brachioradialis, and extensor carpi radialis longus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

Sternum Anatomy. The sternum anatomy includes a jugular notch, manubrium, sternal angle, body, xiphoid process, clavicular notch, and facets for attachment of costal cartilages 1-7.
Contributed by B Palmer
(Click Image to Enlarge)
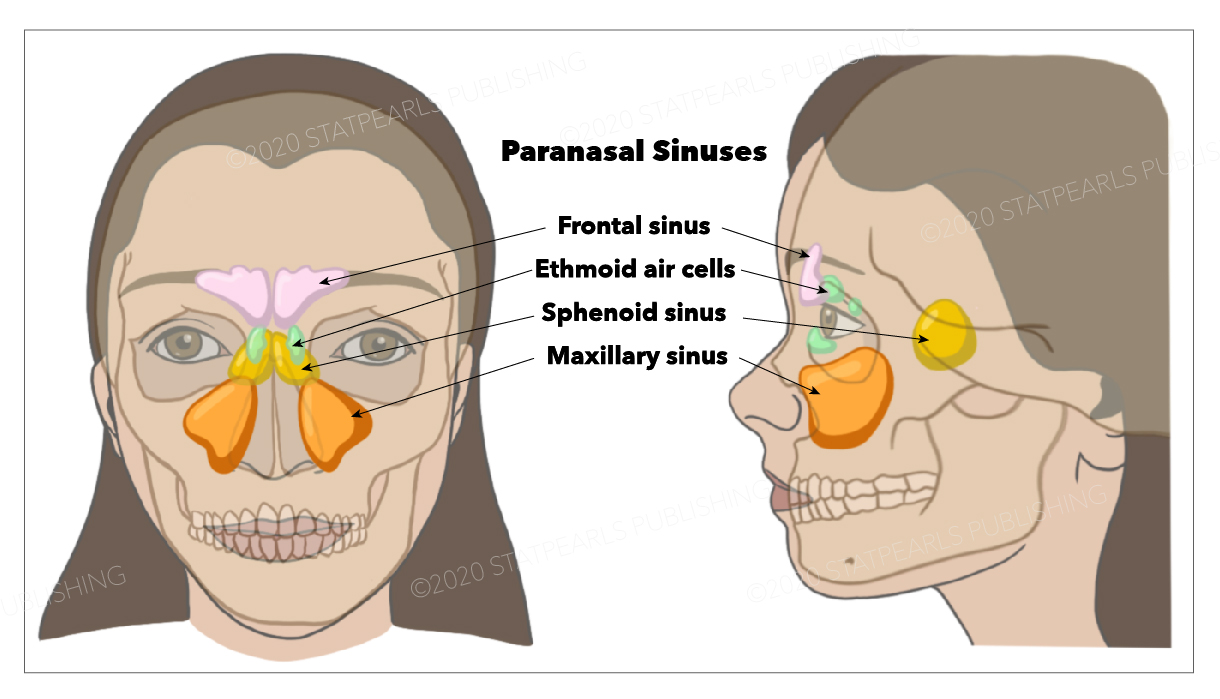
Paranasal Sinuses. The illustrated image shows the frontal, sphenoid, and maxillary sinuses and the ethmoid air cells.
StatPearls Publishing Illustration
(Click Image to Enlarge)

External Ear, Horizontal Section. This horizontal section through the left ear shows the auditory tube, condyle of the mandible, tragus, external and internal acoustic meatus, internal carotid artery, helix, tympanic cavity and membrane, mastoid air-cells, part of the parotid gland, and transverse sinus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
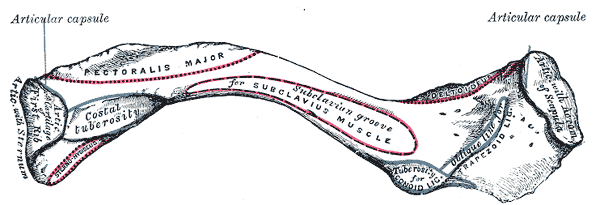
Anterior Surface of Clavicle. Image shows articular capsule, costal tuberosity, subclavian groove, articulating cartilage of first rib, articulation with sternum, deltoid, tuberosity for conoid ligament, acromion of scapula, and trapezoid ligament.
Gray's Anatomy
(Click Image to Enlarge)
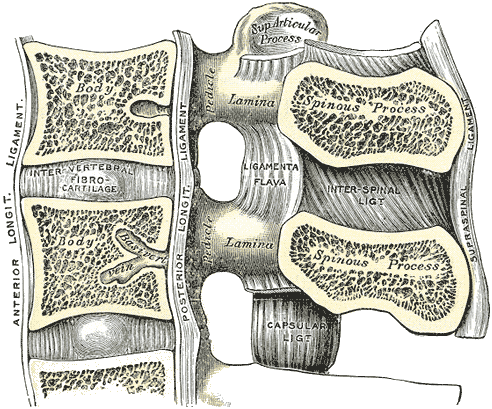
Lumbar Vertebral Anatomy. This medial sagittal section shows the relationship between the anterior longitudinal ligament, vertebral bodies, intervertebral fibrocartilage, posterior longitudinal ligament, vertebral laminae, ligamenta flava, superior articular processes, pedicles, spinous processes, interspinal ligament, capsular ligament, and supraspinal ligament.
Gray's Anatomy
(Click Image to Enlarge)

Scapula, Lateral View. This image includes the supraglenoid and infraglenoid tubercles, coracoid process, acromion, scapular spine, glenoid cavity, subscapularis attachment, and axillary border.
Gray's Anatomy
(Click Image to Enlarge)

Pterygoids. This image shows the greater wing of the sphenoid and the mandibular body, condyle, articular disk, angle, and ramus and their relationship to the pterygoideus externus and internus.
Henry Vandyke Carter, Public domain, via Wikimedia Commons
References
Arostegui M, Scott RW, Underhill TM. Hic1 identifies a specialized mesenchymal progenitor population in the embryonic limb responsible for bone superstructure formation. Cell reports. 2023 Apr 25:42(4):112325. doi: 10.1016/j.celrep.2023.112325. Epub 2023 Mar 31 [PubMed PMID: 37002923]
Sui H, Dou J, Shi B, Cheng X. The reciprocity of skeletal muscle and bone: an evolving view from mechanical coupling, secretory crosstalk to stem cell exchange. Frontiers in physiology. 2024:15():1349253. doi: 10.3389/fphys.2024.1349253. Epub 2024 Mar 4 [PubMed PMID: 38505709]
İnceoğlu A, Bahşi İ, Orhan M, Yalçın ED, İnceoğlu F. The Radiological Evaluation of the Mastoid Process and Its Implications for Surgical Approaches. Cureus. 2021 Jul:13(7):e16101. doi: 10.7759/cureus.16101. Epub 2021 Jul 2 [PubMed PMID: 34350070]
Fiester P, Rao D, Soule E, Orallo P, Rahmathulla G. Anatomic, functional, and radiographic review of the ligaments of the craniocervical junction. Journal of craniovertebral junction & spine. 2021 Jan-Mar:12(1):4-9. doi: 10.4103/jcvjs.JCVJS_209_20. Epub 2021 Mar 4 [PubMed PMID: 33850375]
Hu S, Colley P. Surgical Orbital Anatomy. Seminars in plastic surgery. 2019 May:33(2):85-91. doi: 10.1055/s-0039-1685476. Epub 2019 Apr 26 [PubMed PMID: 31037044]
Lipsett BJ, Alsayouri K. Anatomy, Head and Neck, Skull Foramen. StatPearls. 2024 Jan:(): [PubMed PMID: 31536228]
Ourieff J, Scheckel B, Agarwal A. Anatomy, Back, Trapezius. StatPearls. 2024 Jan:(): [PubMed PMID: 30085536]
McCausland C, Sawyer E, Eovaldi BJ, Varacallo MA. Anatomy, Shoulder and Upper Limb, Shoulder Muscles. StatPearls. 2025 Jan:(): [PubMed PMID: 30521257]
Rudran B, Little C, Duff A, Poon H, Tang Q. Proximal humerus fractures: anatomy, diagnosis and management. British journal of hospital medicine (London, England : 2005). 2022 Jul 2:83(7):1-10. doi: 10.12968/hmed.2021.0554. Epub 2022 Jul 6 [PubMed PMID: 35938761]
Stokey PJ, Kaur S, Lee A, Behrens K, Ebraheim N. Anatomy and Deficiency of the Deltoid Muscle: A Review of Literature. Orthopedic reviews. 2024:16():115352. doi: 10.52965/001c.115352. Epub 2024 Mar 30 [PubMed PMID: 38562147]
Mostafa E, Imonugo O, Varacallo M. Anatomy, Shoulder and Upper Limb, Humerus. StatPearls. 2024 Jan:(): [PubMed PMID: 30521242]
Bair MM, Zafar Gondal A. Anatomy, Shoulder and Upper Limb, Forearm Radius. StatPearls. 2024 Jan:(): [PubMed PMID: 31356039]
Card RK, Lowe JB. Anatomy, Shoulder and Upper Limb, Elbow Joint. StatPearls. 2024 Jan:(): [PubMed PMID: 30422543]
Arias DG, Black AC, Varacallo M. Anatomy, Shoulder and Upper Limb, Hand Bones. StatPearls. 2024 Jan:(): [PubMed PMID: 31613464]
Wobser AM, Adkins Z, Wobser RW. Anatomy, Abdomen and Pelvis: Bones (Ilium, Ischium, and Pubis). StatPearls. 2024 Jan:(): [PubMed PMID: 30137809]
Chang A, Breeland G, Black AC, Hubbard JB. Anatomy, Bony Pelvis and Lower Limb: Femur. StatPearls. 2024 Jan:(): [PubMed PMID: 30422577]
Cox CF, Sinkler MA, Black AC, Launico MV, Hubbard JB. Anatomy, Bony Pelvis and Lower Limb, Knee Patella. StatPearls. 2024 Jan:(): [PubMed PMID: 30137819]
Bourne M, Sinkler MA, Murphy PB. Anatomy, Bony Pelvis and Lower Limb: Tibia. StatPearls. 2025 Jan:(): [PubMed PMID: 30252309]
Cantrell AJ, Imonugo O, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Leg Bones. StatPearls. 2024 Jan:(): [PubMed PMID: 30725709]
Ghanem I, Massaad A, Assi A, Rizkallah M, Bizdikian AJ, El Abiad R, Seringe R, Mosca V, Wicart P. Understanding the foot's functional anatomy in physiological and pathological conditions: the calcaneopedal unit concept. Journal of children's orthopaedics. 2019 Apr 1:13(2):134-146. doi: 10.1302/1863-2548.13.180022. Epub [PubMed PMID: 30996737]
Level 3 (low-level) evidencePanesar K, Susarla SM. Mandibular Fractures: Diagnosis and Management. Seminars in plastic surgery. 2021 Nov:35(4):238-249. doi: 10.1055/s-0041-1735818. Epub 2021 Oct 11 [PubMed PMID: 34819805]
Frost BA, Camarero-Espinosa S, Foster EJ. Materials for the Spine: Anatomy, Problems, and Solutions. Materials (Basel, Switzerland). 2019 Jan 14:12(2):. doi: 10.3390/ma12020253. Epub 2019 Jan 14 [PubMed PMID: 30646556]
de Farias LPG, Menezes DC, Faé IS, de Arruda PHC, Santos JMMM, Teles GBDS. Anatomical variations and congenital anomalies of the ribs revisited by multidetector computed tomography. Radiologia brasileira. 2020 Nov-Dec:53(6):413-418. doi: 10.1590/0100-3984.2019.0131. Epub [PubMed PMID: 33304010]
Ball M, Falkson SR, Fakoya AO, Adigun OO. Anatomy, Angle of Louis. StatPearls. 2025 Jan:(): [PubMed PMID: 29083679]
Altalib AA, Miao KH, Menezes RG. Anatomy, Thorax, Sternum. StatPearls. 2025 Jan:(): [PubMed PMID: 31082185]
Breeland G, Sinkler MA, Menezes RG. Embryology, Bone Ossification. StatPearls. 2024 Jan:(): [PubMed PMID: 30969540]
Šromová V, Sobola D, Kaspar P. A Brief Review of Bone Cell Function and Importance. Cells. 2023 Nov 5:12(21):. doi: 10.3390/cells12212576. Epub 2023 Nov 5 [PubMed PMID: 37947654]
Kawasaki Y, Kinose S, Kato K, Sakai T, Ichimura K. Anatomic characterization of the femoral nutrient artery: Application to fracture and surgery of the femur. Clinical anatomy (New York, N.Y.). 2020 May:33(4):479-487. doi: 10.1002/ca.23390. Epub 2019 Apr 30 [PubMed PMID: 31008535]
Cowan PT, Kahai P. Anatomy, Bones. StatPearls. 2024 Jan:(): [PubMed PMID: 30725884]
Chen J, Hendriks M, Chatzis A, Ramasamy SK, Kusumbe AP. Bone Vasculature and Bone Marrow Vascular Niches in Health and Disease. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 2020 Nov:35(11):2103-2120. doi: 10.1002/jbmr.4171. Epub 2020 Sep 23 [PubMed PMID: 32845550]
Steverink JG, Oostinga D, van Tol FR, van Rijen MHP, Mackaaij C, Verlinde-Schellekens SAMW, Oosterman BJ, Van Wijck AJM, Roeling TAP, Verlaan JJ. Sensory Innervation of Human Bone: An Immunohistochemical Study to Further Understand Bone Pain. The journal of pain. 2021 Nov:22(11):1385-1395. doi: 10.1016/j.jpain.2021.04.006. Epub 2021 May 5 [PubMed PMID: 33964414]
Tomlinson RE, Christiansen BA, Giannone AA, Genetos DC. The Role of Nerves in Skeletal Development, Adaptation, and Aging. Frontiers in endocrinology. 2020:11():646. doi: 10.3389/fendo.2020.00646. Epub 2020 Sep 23 [PubMed PMID: 33071963]
Ashafai NS, Visocchi M, Wąsik N. Occipitocervical Fusion: An Updated Review. Acta neurochirurgica. Supplement. 2019:125():247-252. doi: 10.1007/978-3-319-62515-7_35. Epub [PubMed PMID: 30610329]
Langer MF, Unglaub F, Breiter S, Ueberberg J, Wieskötter B, Oeckenpöhler S. [Anatomy and pathobiomechanics of the scaphoid]. Der Unfallchirurg. 2019 Mar:122(3):170-181. doi: 10.1007/s00113-018-0597-1. Epub [PubMed PMID: 30607486]
Nardi NM, Schaefer TJ. Nursemaid Elbow. StatPearls. 2024 Jan:(): [PubMed PMID: 28613528]
Slobogean GP, Johal H, Lefaivre KA, MacIntyre NJ, Sprague S, Scott T, Guy P, Cripton PA, McKee M, Bhandari M. A scoping review of the proximal humerus fracture literature. BMC musculoskeletal disorders. 2015 May 10:16():112. doi: 10.1186/s12891-015-0564-8. Epub 2015 May 10 [PubMed PMID: 25958203]
Level 2 (mid-level) evidenceRouleau DM, Mutch J, Laflamme GY. Surgical Treatment of Displaced Greater Tuberosity Fractures of the Humerus. The Journal of the American Academy of Orthopaedic Surgeons. 2016 Jan:24(1):46-56. doi: 10.5435/JAAOS-D-14-00289. Epub [PubMed PMID: 26700632]
Earwaker J. Isolated avulsion fracture of the lesser tuberosity of the humerus. Skeletal radiology. 1990:19(2):121-5 [PubMed PMID: 2181684]
Level 3 (low-level) evidenceBedoya MA, Barrera CA, Bencardino JT, Ho-Fung V. Humeral lesser tuberosity avulsion fractures - magnetic resonance imaging characteristics in the pediatric population. Pediatric radiology. 2021 Jul:51(8):1421-1430. doi: 10.1007/s00247-021-04988-y. Epub 2021 Mar 5 [PubMed PMID: 33666731]
Katthagen JC, Michel P, Raschke MJ, Sußiek J, Frank A, Wermers J, Dyrna F, Schliemann B. The forgotten fragment: additional lesser tuberosity fixation of 4-part proximal humeral fractures-a biomechanical investigation. Journal of shoulder and elbow surgery. 2021 Dec:30(12):2852-2861. doi: 10.1016/j.jse.2021.04.041. Epub 2021 May 19 [PubMed PMID: 34022364]
Rangan A, Handoll H, Brealey S, Jefferson L, Keding A, Martin BC, Goodchild L, Chuang LH, Hewitt C, Torgerson D, PROFHER Trial Collaborators. Surgical vs nonsurgical treatment of adults with displaced fractures of the proximal humerus: the PROFHER randomized clinical trial. JAMA. 2015 Mar 10:313(10):1037-47. doi: 10.1001/jama.2015.1629. Epub [PubMed PMID: 25756440]
Level 1 (high-level) evidenceAttum B, Thompson JH. Humerus Fractures Overview. StatPearls. 2024 Jan:(): [PubMed PMID: 29489190]
Level 3 (low-level) evidenceAndo A, Hagiwara Y, Koide M, Yamashiro M, Matsuda M, Itoi E. Lateral dislocation of the elbow with concomitant lateral epicondyle fracture: A case report and review of the literature. Journal of orthopaedic science : official journal of the Japanese Orthopaedic Association. 2019 May:24(3):563-567. doi: 10.1016/j.jos.2016.12.028. Epub 2017 Feb 2 [PubMed PMID: 28162856]
Level 3 (low-level) evidenceOgawa K, Yoshida A, Matsumura N, Inokuchi W. Fracture-Separation of the Medial Humeral Epicondyle Caused by Arm Wrestling: A Systematic Review. Orthopaedic journal of sports medicine. 2022 May:10(5):23259671221087606. doi: 10.1177/23259671221087606. Epub 2022 May 4 [PubMed PMID: 35528993]
Level 1 (high-level) evidenceRehm A, Thahir A, Ngu A. Pediatric Medial Epicondyle Fracture Management: A Systematic Review. Journal of pediatric orthopedics. 2021 Feb 1:41(2):e202-e203. doi: 10.1097/BPO.0000000000001692. Epub [PubMed PMID: 33165265]
Level 1 (high-level) evidenceKim H, Kwon B, Kim J, Nam K. Isolated hook of hamate fracture in sports that require a strong grip comprehensive literature review. Medicine. 2018 Nov:97(46):e13275. doi: 10.1097/MD.0000000000013275. Epub [PubMed PMID: 30431614]
Tian A, Goldfarb CA. Hook of Hamate Fractures. Hand clinics. 2021 Nov:37(4):545-552. doi: 10.1016/j.hcl.2021.06.013. Epub [PubMed PMID: 34602134]
Davis DL. Hook of the Hamate: The Spectrum of Often Missed Pathologic Findings. AJR. American journal of roentgenology. 2017 Nov:209(5):1110-1118. doi: 10.2214/AJR.17.18043. Epub 2017 Aug 23 [PubMed PMID: 28834449]
Tada K, Ikeda K, Okamoto S, Hachinota A, Yamamoto D, Tsuchiya H. Scaphoid Fracture--Overview and Conservative Treatment. Hand surgery : an international journal devoted to hand and upper limb surgery and related research : journal of the Asia-Pacific Federation of Societies for Surgery of the Hand. 2015:20(2):204-9 [PubMed PMID: 26051761]
Level 3 (low-level) evidenceFowler JR, Hughes TB. Scaphoid fractures. Clinics in sports medicine. 2015 Jan:34(1):37-50. doi: 10.1016/j.csm.2014.09.011. Epub 2014 Nov 25 [PubMed PMID: 25455395]
Jernigan EW, Morse KW, Carlson MG. Managing the Athlete with a Scaphoid Fracture. Hand clinics. 2019 Aug:35(3):365-371. doi: 10.1016/j.hcl.2019.03.011. Epub [PubMed PMID: 31178093]
Lutnick E, Kang J, Freccero DM. Surgical Treatment of Femoral Neck Fractures: A Brief Review. Geriatrics (Basel, Switzerland). 2020 Apr 1:5(2):. doi: 10.3390/geriatrics5020022. Epub 2020 Apr 1 [PubMed PMID: 32244621]
Castano Betancourt MC, Maia CR, Munhoz M, Morais CL, Machado EG. A review of Risk Factors for Post-traumatic hip and knee osteoarthritis following musculoskeletal injuries other than anterior cruciate ligament rupture. Orthopedic reviews. 2022:14(4):38747. doi: 10.52965/001c.38747. Epub 2022 Nov 3 [PubMed PMID: 36349350]
Pegrum J, Self A, Hall N. Iliotibial band syndrome. BMJ (Clinical research ed.). 2019 Mar 21:364():l980. doi: 10.1136/bmj.l980. Epub 2019 Mar 21 [PubMed PMID: 30898786]
Santana JA, Mabrouk A, Sherman AL. Jumpers Knee. StatPearls. 2024 Jan:(): [PubMed PMID: 30422564]
Deshmukh NS, Phansopkar P. Medial Tibial Stress Syndrome: A Review Article. Cureus. 2022 Jul:14(7):e26641. doi: 10.7759/cureus.26641. Epub 2022 Jul 7 [PubMed PMID: 35949792]
Vo TP, Ho GWK, Andrea J. Achilles Tendinopathy, A Brief Review and Update of Current Literature. Current sports medicine reports. 2021 Sep 1:20(9):453-461. doi: 10.1249/JSR.0000000000000884. Epub [PubMed PMID: 34524189]
Tominaga H, MacDowall A, Olerud C. Surgical treatment of the severely damaged atlantoaxial joint with C1-C2 facet spacers: Three case reports. Medicine. 2019 May:98(22):e15827. doi: 10.1097/MD.0000000000015827. Epub [PubMed PMID: 31145323]
Level 3 (low-level) evidenceAbrahão NM, Guimarães GC, Castilho AM, da Silva VAR. Bilateral facial paralysis secondary to temporal bone trauma: A case report and literature review. Clinical case reports. 2021 Jun:9(6):e04272. doi: 10.1002/ccr3.4272. Epub 2021 Jun 22 [PubMed PMID: 34188929]
Level 3 (low-level) evidenceJiang S, Shen H, Tan WQ, Lu H. Arterial thoracic outlet syndrome caused by cervical ribs-an unusual case report. Medicine. 2019 Mar:98(11):e14778. doi: 10.1097/MD.0000000000014778. Epub [PubMed PMID: 30882649]
Level 3 (low-level) evidenceFarina R, Foti PV, Iannace FA, Conti A, Ferlito A, Conti A, Pennisi M, Santonocito S, Basile A. Thoracic outlet syndrome: a rare case with bilateral cervical ribs and bilateral anterior scalene hypertrophy. Journal of ultrasound. 2021 Sep:24(3):331-336. doi: 10.1007/s40477-019-00418-w. Epub 2019 Dec 13 [PubMed PMID: 31834601]
Level 3 (low-level) evidenceNakamae T, Kamei N, Fujimoto Y, Yamada K, Ujigo S, Adachi N. Spinous Process Fractures in Osteoporotic Vertebral Fractures: A Cross-Sectional Study. Spine surgery and related research. 2022:6(2):139-144. doi: 10.22603/ssrr.2021-0066. Epub 2021 Jun 30 [PubMed PMID: 35478979]
Level 2 (mid-level) evidenceBentley TP, Ponnarasu S, Journey JD. Sternal Fracture. StatPearls. 2024 Jan:(): [PubMed PMID: 29939567]