 Anatomy, Shoulder and Upper Limb, Hand Volar Arch Arteries
Anatomy, Shoulder and Upper Limb, Hand Volar Arch Arteries
Introduction
Blood supply to the volar (palmar) surface of the hand originates from the radial and ulnar artery. As the arteries carry blood across the wrist and reach the palm, they anastomose to form two arches called the superficial volar arch and the deep volar arch. These arches, along with their branches, form an abundant network of blood vessels that is responsible for providing oxygenated blood to all musculoskeletal components of the hand and fingers.[1][2][3]
Because the hand often performs a variety of tasks such as grasping objects and applying digital pressure across different planes of movement to carry out dynamic composite functions, the extensive collateral circulation of the hand serves an important role in providing adequate perfusion to all parts of the hand. The recent advancements in hand surgery have made understanding the arterial pattern of the hand and its variants crucial for safe and successful surgical outcomes.[4] This article presents an overview of the hand volar arch arteries and discusses the structure and function, embryology, muscle groups, physiologic variants, surgical considerations, and clinical significance.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The arteries of the volar surface of the hand consist of two systems: the superficial volar arch and the deep volar arch. These arches and their branches form the basis of an extensive collateral circulation that is responsible for providing oxygenated blood to all parts of the hand and fingers.
The superficial volar arch is considered the dominant vascular structure of the palm. It forms mainly by the ulnar artery and the superficial branch of the radial artery. The ulnar artery enters the hand superficial to the flexor retinaculum, via the ulnar canal (Guyon canal), and terminates in the superficial volar arch, where it anastomoses with the superficial branch of the radial artery.[1][2][5] This branch of the radial artery runs superficial to the flexor retinaculum and completes the superficial volar arch. The superficial volar arch localizes superficially to the flexor tendons and deep to the palmar aponeurosis. It lies between the first web space to the hook of Hamate and extends more distally than the deep volar arch.[6][7][5]
Arising from the superficial volar arch are three common palmar digital arteries that travel in the palm, between the finger webs, to supply blood to the fingers. As the common palmar digital arteries travel towards the fingers, they split at the finger web space into two proper palmar digital arteries that run along the contiguous sides of digits two, three, four, and the lateral side of the little finger. The medial aspect of the fifth digit receives supply from a branch off of the superficial volar arch.[6][8]
The deep volar arch forms from the dorsal radial artery and the deep palmar branch of the ulnar artery. Before reaching the flexor retinaculum, the radial artery gives off the superficial branch of the radial artery and then continues as the dorsal radial artery. The dorsal radial artery continues its course by curving around to enter the dorsal aspect of the hand while passing the scaphoid and trapezium, through the floor of the anatomical snuffbox.[9] From there, it passes between the two heads of the first dorsal interosseous muscle to reenter the palmar aspect of the hand.[10] On the palmar side, it turns medially and terminates in the deep volar arch, where it anastomoses with the deep palmar branch of the ulnar artery. The deep palmar branch is a branch of the ulnar artery that completes the deep volar arch. The deep volar arch is localized deep to the flexor tendons of the hand. It lies between the flexor tendons and the metacarpal bones and is proximal to the superficial volar arch.[6]
Arising from the deep volar arch are three palmar metacarpal arteries that anastomose with the common palmar digital arteries coming off of the superficial volar arch.[1][11] The deep volar arch also provides blood supply to the thumb and lateral side of the index finger. As the radial artery turns onto the palmar aspect of the hand, it gives off two branches, the princeps pollicis artery, and radialis indicis artery. The princeps pollicis artery runs along the palmar aspect of the first metacarpal and bifurcates distally into two palmar digital arteries that provide blood supply to each side of the thumb. The radialis indicis artery runs along the first dorsal interosseus muscle to provide blood supply to the lateral side of the index finger.[6]
Embryology
The current theory regarding the embryonic development of the arterial pattern of the hand suggests that development takes place by a combined process. At stage 12, an initial capillary network arises from the dorsal aorta and expands into the growing limb bud. At the same time, the proximal parts of this network begin to enlarge, and the arterial wall begins to differentiate by stage 13. From stages 13 to 21, differentiation occurs in a proximal to a distal sequence starting with the development of the ulnar, interosseous, and median arteries. At stage 18, the radial artery develops and acquires its final differentiated morphological state by stage 21. By stage 21, the definitive arterial pattern of the hand with the palmar arches is established. However, science does not yet fully understand the mechanisms that determine the development of the arterial pattern. One theory states that oxygenation, nutrient requirements, and hemodynamic forces are important influencers. Another theory suggests that the underlying mechanism may have a genetic component.[12]
Blood Supply and Lymphatics
The superficial and deep volar arterial arches are both accompanied by a pair of venae comitantes which are called the superficial and deep palmar venous arches. These veins drain deoxygenated blood from the hand and fingers corresponding to the branches of the arterial arch. The common palmar digital veins receive blood from the proper palmar digital veins and drain into the superficial palmar venous arch. These veins ultimately drain to the radial vein. The palmar metacarpal veins, which receives blood from the metacarpal region of the palm, drains into the deep palmar venous arch. Some branches of the palmar metacarpal veins also drain into the dorsal metacarpal veins and end in the radial veins as well as the superficial veins on the dorsum of the wrist.[10][1]
Similarly, lymphatic drainage of the hand divides into superficial and deep lymphatic vessels. The superficial lymphatic vessels lie near the major superficial veins, while the deep lymphatic vessels follow major deep veins.[13]
Nerves
Sympathetic nerves innervate the arteries of the hand. More specifically, the second and third thoracic ganglia are responsible for the sympathetic innervation of the hand.[14] In response to cold stimuli, to prevent undesirable heat loss, the arterioles of the hand can constrict and reduce blood flow to the surface and ends of fingers.[15]
Raynaud syndrome is an idiopathic condition marked by intermittent ischemia of digits, often accompanied by paresthesia and pain. While this condition is idiopathic, it is usually brought on by cold and emotional stimuli.[15] Cervicodorsal presynaptic sympathectomy is an effective surgical technique for treating Raynaud syndrome in the fingers. This procedure involves excising a segment of the sympathetic chain to dilate the digital arteries.[14]
Muscles
The hand contains an extensive network of collateral vessels so that oxygenated blood can reach all parts of the muscles in the hand and fingers. In the event that one of these vessels is injured, the connections that exist between arteries are capable of maintaining perfusion to the muscle. This network allows blood supply to reach areas of ischemia when injuries occur.[2]
Physiologic Variants
Because the arteries of the hand make up a vast network of highly branched and anastomosed arteries, there are numerous anatomic variations of the arterial patterns of the hand. These variants generally demonstrate either complete or incomplete superficial and deep arterial arches. When an anastomosis is present between the vessels, the arch is considered complete. An incomplete arch is present when there is the absence of anastomosis between the vessels. With recent advancements in hand microsurgery, the understanding of the vasculature of the hand and its variants has become increasingly important. A recent meta-analysis found that the complete superficial volar arch presented in 81.3% of cases. Research has reported seven different types of complete superficial volar arches and five different types of incomplete superficial volar arches. The deep volar arch was found to be less variant with complete arch found in 95.2% of cases.[16]
Surgical Considerations
The radial artery is often the source for drawing blood gases, cannulation for placement of arterial lines, catheterizations, or as a harvested graft for patients undergoing coronary revascularization. Since the ulnar and radial artery form, an anastomosis with the formation of the deep and superficial volar arches, the blood supply to the hand remains intact if one of the arteries becomes occluded during a procedure. However, the risks associated with these procedures include ischemia distal to the radial artery puncture site and compromise to the limb. These complications may occur in cases where the patient’s collateral circulation inadequately maintains perfusion.[17] Thus, the assessment of collateral blood flow to the hands is necessary to ensure adequate circulation after operations. The Allen test and Modified Allen test are diagnostic tools to evaluate collateral circulation before procedures.[18]
Clinical Significance
Clinically, the arterial supply to the hand and fingers are essential. While collateral circulation often remains intact in the event of the occlusion or damage to the ulnar or radial artery, patients with anatomical vascular variations may develop ischemia and limb compromise if collateral circulation is inadequate. Studies have highlighted that clinicians must be aware of, and report significant anatomical vascular variants to prevent potential consequences associated with them.[17]
Other Issues
Traumatic injuries to the hand commonly result in damage to the common digital arteries. Surgeons have explored the technique of repairing the transected common digital arteries by transferring the superficial palmar arch more distally to reach the common digital artery for revascularization.[19]
Media
(Click Image to Enlarge)
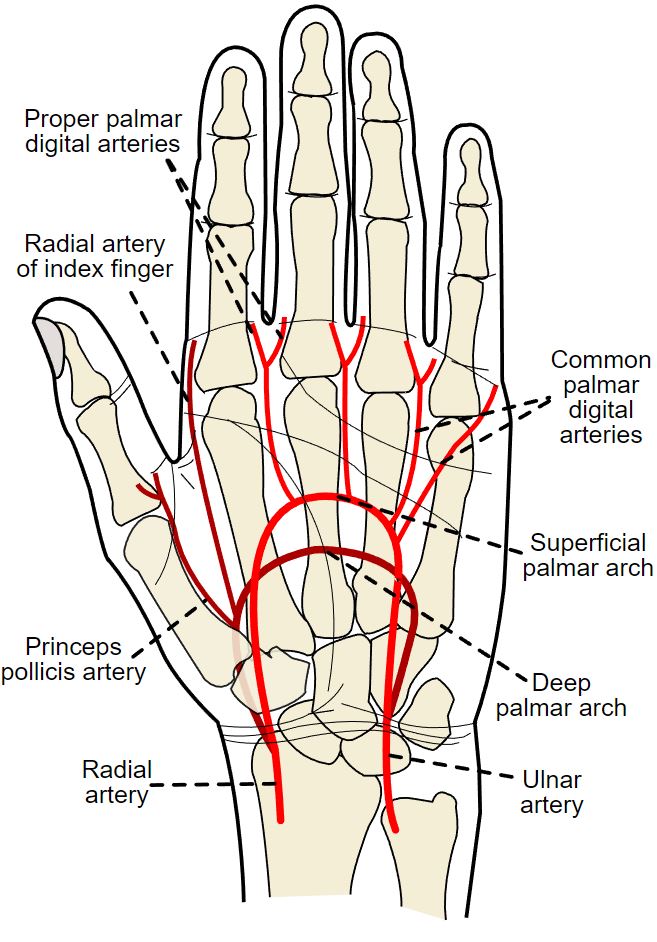
Hand Volar Arches Contributed by Rhcastilhos, released into the public domain.
References
Dawson-Amoah K, Varacallo M. Anatomy, Shoulder and Upper Limb, Hand Intrinsic Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30969632]
Okwumabua E, Sinkler MA, Bordoni B. Anatomy, Shoulder and Upper Limb, Hand Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30725914]
Epperson TN, Varacallo M. Anatomy, Shoulder and Upper Limb, Brachial Artery. StatPearls. 2023 Jan:(): [PubMed PMID: 30725830]
Brzezinski M, Luisetti T, London MJ. Radial artery cannulation: a comprehensive review of recent anatomic and physiologic investigations. Anesthesia and analgesia. 2009 Dec:109(6):1763-81. doi: 10.1213/ANE.0b013e3181bbd416. Epub [PubMed PMID: 19923502]
Ramage JL, Varacallo M. Anatomy, Shoulder and Upper Limb, Hand Guyon Canal. StatPearls. 2023 Jan:(): [PubMed PMID: 30521235]
Singh S, Lazarus L, De Gama BZ, Satyapal KS. An anatomical investigation of the superficial and deep palmar arches. Folia morphologica. 2017:76(2):219-225. doi: 10.5603/FM.a2016.0050. Epub 2016 Sep 26 [PubMed PMID: 27665957]
Aleksenko D, Varacallo M. Guyon Canal Syndrome. StatPearls. 2023 Jan:(): [PubMed PMID: 28613717]
Gnanasekaran D, Veeramani R. Newer insights in the anatomy of superficial palmar arch. Surgical and radiologic anatomy : SRA. 2019 Jul:41(7):791-799. doi: 10.1007/s00276-019-02223-w. Epub 2019 Mar 28 [PubMed PMID: 30923841]
Hallett S, Jozsa F, Ashurst JV. Anatomy, Shoulder and Upper Limb, Hand Anatomical Snuff Box. StatPearls. 2023 Jan:(): [PubMed PMID: 29489241]
Valenzuela M,Bordoni B, Anatomy, Shoulder and Upper Limb, Hand Dorsal Interossei Muscle 2019 Jan; [PubMed PMID: 30725607]
Valenzuela M, Varacallo M. Anatomy, Shoulder and Upper Limb, Hand Interossei Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30521193]
Rodríguez-Niedenführ M, Burton GJ, Deu J, Sañudo JR. Development of the arterial pattern in the upper limb of staged human embryos: normal development and anatomic variations. Journal of anatomy. 2001 Oct:199(Pt 4):407-17 [PubMed PMID: 11693301]
Valenzuela M, Bordoni B. Anatomy, Shoulder and Upper Limb, Hand Palmar Interosseous Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30725850]
Coveliers HM, Hoexum F, Nederhoed JH, Wisselink W, Rauwerda JA. Thoracic sympathectomy for digital ischemia: a summary of evidence. Journal of vascular surgery. 2011 Jul:54(1):273-7. doi: 10.1016/j.jvs.2011.01.069. Epub 2011 Jun 8 [PubMed PMID: 21652164]
Musa R, Qurie A. Raynaud Disease. StatPearls. 2023 Jan:(): [PubMed PMID: 29763008]
Zarzecki MP, Popieluszko P, Zayachkowski A, Pękala PA, Henry BM, Tomaszewski KA. The surgical anatomy of the superficial and deep palmar arches: A Meta-analysis. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2018 Nov:71(11):1577-1592. doi: 10.1016/j.bjps.2018.08.014. Epub 2018 Aug 24 [PubMed PMID: 30245020]
Level 1 (high-level) evidenceHabib J, Baetz L, Satiani B. Assessment of collateral circulation to the hand prior to radial artery harvest. Vascular medicine (London, England). 2012 Oct:17(5):352-61. doi: 10.1177/1358863X12451514. Epub 2012 Jul 19 [PubMed PMID: 22814998]
Zisquit J, Velasquez J, Nedeff N. Allen Test. StatPearls. 2023 Jan:(): [PubMed PMID: 29939593]
Korambayil PM. Use of superficial palmar arch for bridging the gap in digital revascularisation. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2011 Sep:44(3):511-6. doi: 10.4103/0970-0358.90844. Epub [PubMed PMID: 22279293]
Level 3 (low-level) evidence