Introduction
A ventriculoperitoneal (VP) shunt is a cerebral shunt that drains excess cerebrospinal fluid (CSF) when there is an obstruction in the normal outflow or there is a decreased absorption of the fluid. Cerebral shunts are used to treat hydrocephalus. In pediatric patients, untreated hydrocephalus can lead to many adverse effects including increase irritabilities, chronic headaches, learning difficulties, visual disturbances, and in more advanced cases severe mental retardation.[1][2][3]. After placement, if it malfunction, excess CSF accumulated which can increase the intracranial pressure resulting in cerebral edema and ultimately herniation. These shunts drain the CSF into the peritoneal cavity, the atrium, or the pleura; thus, appropriately called ventriculoperitoneal, ventriculoatrial, and ventriculopleural shunts.
A shunt consists of a ventricular catheter that is connected to a valve and then connected to a distal catheter. The distal end of a VP shunt is placed in the peritoneal cavity. The main differences between shunts are the type of valve used, and whether the valve is programmable or not. Advances in the biotechnologies are leading to progressive changes in the shunt components. These advanced components are expected to reduce shunt malfunctions and optimize neurosurgical patient care.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The ventricles of the brain are a communicating network of cavities located within the brain parenchyma. The ventricular system is composed of two lateral ventricles, the third ventricle, the cerebral aqueduct, and the fourth ventricle. The choroid plexus in the ventricles produce CSF, which fills the ventricle and the subarachnoid space in a constant cycle of production and reabsorption.[2][4][5][6] The CSF is then absorbed into the cerebral venous circulation through the Pacchionian (arachnoid)granulations. Any block or obstruction in this pathway will produce obstructive hydrocephalus and if permanent will require a shunt. Sometimes, these granulations become obstructed from blood products or high protein and will not function adequately producing communicating hydrocephalus.
Placement of a cerebral shunt and its location is determined based on the surgeon's preference. It may be placed through a frontal approach into the anterior horn of the lateral ventricles or though a parieto-occipital approach into the trigone or occipital horn of the lateral ventricle. The catheter placed into the cerebral ventricle is called the proximal shunt (ventricular catheter) implying proximity to the brain. The most preferred proximal shunt location is on the right lateral ventricle as any complication will not be associated with the dominant hemisphere. If there is asymmetry, then the larger ventricle is used. The distal catheter can be placed in the abdomen (peritoneal cavity), heart via a cervical venous access, chest cavity (pleura), or rarely into the ureter or the bladder if all previous sites have been used. In all cases, however, the distal end of the catheter can be located in any tissue with cells capable of absorbing the incoming CSF.
A subgaleal shunt is a temporary measure used in infants who are too small or premature to tolerate other shunts of have difficulty with peritoneal absorption. The surgeon forms a pocket beneath the subgaleal space and allows the CSF to drain from the ventricles, creating a fluid-filled swelling on the infant's scalp. As the child grows, these shunts are later converted to a permanent shunt type.[7][8][9]
Indications
Most VP shunts are placed to treat the hydrocephalus. Disorders that typically requiring shunting include the following:
- Congenital hydrocephalus after aqueductal stenosis is a genetic disorder which can cause deformations of the nervous system and is associated with mental retardation, abducted thumbs, and spastic paraplegia
- Tumors leading to CSF blockage of the lateral ventricles, third ventricle, and those in the posterior fossa blocking the cerebral aqueduct or fourth ventricle
- Communicating hydrocephalus secondary to meningitis or subarachnoid hemorrhage
- Myelomeningocele causes the development of hydrocephalus because the flow of CSF is altered due to hindbrain malformation
- Craniosynostosis occurs when the sutures of the skull close too early with sutures fusing before the brain stops growing and in rare occasions can cause hydrocephalus
- Dandy-Walker syndrome presents with a cystic deformity of the fourth ventricle, hypoplasia of the cerebellar vermis, and an enlarged posterior fossa
- Arachnoid cysts are a defect caused when CSF forms a collection that is trapped in the arachnoid membranes resulting in a block of the normal flow of CSF resulting in hydrocephalus
- Idiopathic intracranial hypertension is a rare neurological disorder affecting approximately 1 in 100,000 people, usually women of childbearing age, causing a rise in intracranial pressure which can result in permanent loss of vision
- Normal-pressure hydrocephalus caused a classic triad of memory problems/dementia, gait dysfunction, and urinary incontinence.
Contraindications
Absolute contraindications include:
- Infection over the entry site
- Infection of the CSF
- Allergy to any of the catheter components (silicone)[10][11][12]
Relative contraindications include:
- altered coagulation function
- high CSF protein
- CSF with blood
Equipment
A VP shunt is placed in the operating room under general anesthesia by a neurosurgeon.
Equipment needed to perform the procedure includes:
- Shunt system (ventricular catheter, peritoneal catheter, and valve)
- Valve (small, medium, or high-pressure)
- Programmable valve
- Specimen tubes for CSF
- Drill for the burr hole
- Shunt passer
- Image-guided navigation system (only for small ventricles)
Personnel
Neurosurgeon
Anesthesiologist
Nurse (circulating and technical)
Preparation
Brain magnetic resonance imaging (MRI) or computed tomography (CT) scan is reviewed for the planning of the shunt and the proper placement of the proximal catheter. All patients need appropriate preoperative workup and informed consent for surgery and general anesthesia. The patient is placed supine. For a parieto-occipital approach, the head is tilted to the contralateral side of the shunt placement. Preoperative antibiotics are given and the patient is dressed in sterile conditions.
Technique or Treatment
- Shave the hair away from the head incision site (some surgeons use minimal shaving)
- Clean the skin with an antiseptic
- Apply a sterile fenestrated drape over the incision sites (head, neck, chest, and abdomen)
- Fenestrated drape the patient
- Make a "U or C" shaped skin incision over the entry point where the burr hole is to be performed for the introduction of the ventricular catheter. If the frontal approach will be used, then Kocher’s point is used which is an entry point that is 11 cm superior and posterior from the nasion, 3 cm lateral to midline along the mid pupillary line, and 1 to 2 cm anterior to the coronal suture; catheter should then be passed to a depth of 5-5.5 cm.[13] For a parieto-occipital approach, Keen’s point is used which is approximately 2.5 to 3 cm superior and posterior to the pinna and the catheter should then be passed to a depth of 4 to 5 cm or until reaching the trigone of the ipsilateral lateral ventricle, but sometimes it is aiming toward the frontal horn of the lateral ventricle.[13] Alternatively, Dandy's point can be used which is 3 cm above the inion and 2 cm left or right to the midline.[13]
- Burr hole is performed at the desired entry point and the dura incised. A small entry point in the cortex is coagulated and incised.
- Ventricular catheter is introduced directed into the ventricle and cut to the appropriate pre-measured length
- CSF samples are collected
- The ventricular shunt is connected to the valve and secured with a silk tie.
- An incision in the abdomen is done to access the peritoneal cavity; the site depends on the surgeon's preference and can be done in the upper quadrant or the midline
- Shunt passer is used to pass the peritoneal distal catheter between both incisions.
- Peritoneal catheter is connected to the valve and secured with a silk tie.
- After good distal CSF flow at the peritoneal catheter, it is introduced into the peritoneal cavity.
- Wounds are closed in anatomical layers
- The CSF sample is sent to the laboratory for cell count, glucose, protein, gram stain, and culture
Complications
Complications include the following:
- Infection due to skin flora entering the shunt, usually from Staphylococcus epidermidis
- Intracerebral or intraventricular hemorrhage
- Malposition
- Abdominal perforation during placement
- Shunt erosion of the skin with exposure of the system
- Shunt over drainage (slit ventricles)[14][15][16]
- Shunt nephritis[17][18]
- Shunt disconnection
- Shunt obstruction
- Subdural hematomas
- Abdominal CSF collections (pseudocyst or CSFoma)[16]
- Shunt breakage at any point
- Catheter perforation of viscera and rarely extrusion through the anus[19][20][21]
- Inguinal hernia
- Seizures
In those cases of malfunction, the shunt has to be assessed for proper function. The following technique is used:
- Clean the skin with an antiseptic
- Apply a sterile fenestrated drape over the incision site
- Insert a small (23 ga) butterfly needle perpendicular to the skin into the reservoir
- Evaluate for spontaneous CSF filling the line of the butterfly needle
- Measure the opening pressure using a manometer
- Aspirate CSF with syringe
- Collect 5 mL of CSF and place into sterile specimen containers
- Withdraw the needle from the reservoir
- Gauze applied to site
- Send the cerebrospinal fluid sample for cell count, glucose, protein, gram stain, and culture
Complications of a shunt tap are:
- Bleeding from subcutaneous vessels during the tap
- Cerebrospinal fluid leak from the puncture site
- Ventricular collapse due to rapid aspiration of CSF, especially in slit ventricles
- A misplaced tap can result in the sectioning of the tubing or the reservoir.
Clinical Significance
Ventriculoperitoneal shunts are used to treat hydrocephalus and divert CSF from the lateral ventricles into the peritoneum. Tapping a shunt is performed for both diagnostic and therapeutic reasons (evaluate for infection or malfunction). A VP shunt is one of the high impact advances made in neurosurgical patient care.
Evaluation
Patients with shunts are evaluated for evidence of signs or symptoms related to complications or malfunction. Acute symptoms of malfunction/infection are: headache, lethargy, diplopia, nausea and vomiting, seizure, irritability, poor feeding, head enlargement when sutures are open, tense fontanelle, fever, neck rigidity. Shunt system has to be assessed manually for proper function and visible for evidence of redness or swelling along the shunt tubing. Shunt X rays are done to evaluate the integrity of the system. CT scan or MRI is done to evaluate the size of the ventricles.
Outcome
VP shunt can be lifesaving, but the eventual outcome depends on the reason why the shunt was inserted. For benign disorders, most patients have a good outcome. However, for malignant tumors, the outcomes are usually poor; often these patients die from other causes unrelated to the shunt. The complication rates of VP shunts range from 2-20%. In addition, shunt revision is required in about 5-10% of neonates and young children.[22][23](Level V)
Enhancing Healthcare Team Outcomes
There is no question that VP shunts have saved many lives, but these devices are not without complications. The shunt has to be monitored for infection and malfunction. The abdomen has to be monitored for peritonitis secondary to shunt infection. While the neurosurgeon is always involved in the care of patients with hydrocephalus, it is important to consult with an interprofessional team that includes a pediatrician, and a general surgeon. Any unusual finding by the primary physician has to be immediately reported back to the neurosurgeon. The nurses are also vital members of the interprofessional group as they will monitor the patient's clinical signs and assist with the education of the patient and the family. In the postoperative period for pain, or for shunt infection; the pharmacist will ensure that the patient is on the right analgesics and appropriate antibiotics. The radiologist also plays a role in determining the cause of the malfunction. Without providing a proper history, the radiologist may not be sure what to look for or what additional radiologic exams may be needed. Before the patient is discharged, the family has to be educated on the early identification of shunt failure and how to monitor the child's improvement. In some cases, a home care nurse may be required to pay regular visits to ensure that the VP shunt is functioning without problems.[24][25] (Level V)
Media
(Click Image to Enlarge)

Radiographic Shunt Series. Shunt series, including biplanar head (a and b), anteroposterior chest (c), and anteroposterior abdominal (d) radiographs demonstrating the ventriculoperitoneal shunt catheter throughout its course.
Contributed by M Özdemir, MD
(Click Image to Enlarge)
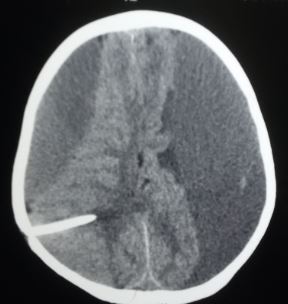
Bilateral chronic subdural hematoma due to shunt over-drain Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)

Shunt disconnection Contributed by Sunil Munakomi, MD
References
Hanna RS, Essa AA, Makhlouf GA, Helmy AA. Comparative Study Between Laparoscopic and Open Techniques for Insertion of Ventriculperitoneal Shunt for Treatment of Congenital Hydrocephalus. Journal of laparoendoscopic & advanced surgical techniques. Part A. 2019 Jan:29(1):109-113. doi: 10.1089/lap.2017.0594. Epub 2018 Oct 10 [PubMed PMID: 30307809]
Level 2 (mid-level) evidenceErps A, Roth J, Constantini S, Lerner-Geva L, Grisaru-Soen G. Risk factors and epidemiology of pediatric ventriculoperitoneal shunt infection. Pediatrics international : official journal of the Japan Pediatric Society. 2018 Dec:60(12):1056-1061. doi: 10.1111/ped.13709. Epub 2018 Dec 10 [PubMed PMID: 30290047]
Kutty RK, Sreemathyamma SB, Korde P, Prabhakar RB, Peethambaran A, Libu GK. Outcome of Ventriculosubgaleal Shunt in the Management of Infectious and Non-infectious Hydrocephalus in Pre-term Infants. Journal of pediatric neurosciences. 2018 Jul-Sep:13(3):322-328. doi: 10.4103/JPN.JPN_41_18. Epub [PubMed PMID: 30271465]
Pan P. Outcome Analysis of Ventriculoperitoneal Shunt Surgery in Pediatric Hydrocephalus. Journal of pediatric neurosciences. 2018 Apr-Jun:13(2):176-181. doi: 10.4103/jpn.JPN_29_18. Epub [PubMed PMID: 30090131]
Burhan B, Serdar KB, Abdurrahman A, Edip AM, Ebuzer D. Abdominal Complications of Ventriculoperitoneal Shunt in Pediatric Patients: Experiences of a Pediatric Surgery Clinic. World neurosurgery. 2018 Oct:118():e129-e136. doi: 10.1016/j.wneu.2018.06.140. Epub 2018 Jun 26 [PubMed PMID: 29959071]
Korzh V. Development of brain ventricular system. Cellular and molecular life sciences : CMLS. 2018 Feb:75(3):375-383. doi: 10.1007/s00018-017-2605-y. Epub 2017 Aug 5 [PubMed PMID: 28780589]
Hong B, Polemikos M, Heissler HE, Hartmann C, Nakamura M, Krauss JK. Challenges in cerebrospinal fluid shunting in patients with glioblastoma. Fluids and barriers of the CNS. 2018 Jun 4:15(1):16. doi: 10.1186/s12987-018-0101-x. Epub 2018 Jun 4 [PubMed PMID: 29860942]
Spirig JM, Frank MN, Regli L, Stieglitz LH. Shunt age-related complications in adult patients with suspected shunt dysfunction. A recommended diagnostic workup. Acta neurochirurgica. 2017 Aug:159(8):1421-1428. doi: 10.1007/s00701-017-3237-6. Epub 2017 Jun 14 [PubMed PMID: 28616668]
Rinaldo L, Lanzino G, Elder BD. Predictors of distal malfunction after ventriculoperitoneal shunting for idiopathic normal pressure hydrocephalus and effect of general surgery involvement. Clinical neurology and neurosurgery. 2018 Nov:174():75-79. doi: 10.1016/j.clineuro.2018.09.009. Epub 2018 Sep 5 [PubMed PMID: 30218879]
Jimenez DF, Keating R, Goodrich JT. Silicone allergy in ventriculoperitoneal shunts. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 1994 Jan:10(1):59-63 [PubMed PMID: 8194064]
Level 3 (low-level) evidenceHussain NS, Wang PP, James C, Carson BS, Avellino AM. Distal ventriculoperitoneal shunt failure caused by silicone allergy. Case report. Journal of neurosurgery. 2005 Mar:102(3):536-9 [PubMed PMID: 15796391]
Level 3 (low-level) evidenceKurin M, Lee K, Gardner P, Fajt M, Umapathy C, Fasanella K. Clinical peritonitis from allergy to silicone ventriculoperitoneal shunt. Clinical journal of gastroenterology. 2017 Jun:10(3):229-231. doi: 10.1007/s12328-017-0729-0. Epub 2017 Mar 6 [PubMed PMID: 28265895]
Morone PJ, Dewan MC, Zuckerman SL, Tubbs RS, Singer RJ. Craniometrics and Ventricular Access: A Review of Kocher's, Kaufman's, Paine's, Menovksy's, Tubbs', Keen's, Frazier's, Dandy's, and Sanchez's Points. Operative neurosurgery (Hagerstown, Md.). 2020 May 1:18(5):461-469. doi: 10.1093/ons/opz194. Epub [PubMed PMID: 31420653]
Ros B, Iglesias S, Martín Á, Carrasco A, Ibáñez G, Arráez MA. Shunt overdrainage syndrome: review of the literature. Neurosurgical review. 2018 Oct:41(4):969-981. doi: 10.1007/s10143-017-0849-5. Epub 2017 Mar 29 [PubMed PMID: 28352945]
Bruce DA, Weprin B. The slit ventricle syndrome. Neurosurgery clinics of North America. 2001 Oct:12(4):709-17, viii [PubMed PMID: 11524292]
Kashyap S, Ghanchi H, Minasian T, Dong F, Miulli D. Abdominal pseudocyst as a complication of ventriculoperitoneal shunt placement: Review of the literature and a proposed algorithm for treatment using 4 illustrative cases. Surgical neurology international. 2017:8():78. doi: 10.4103/2152-7806.206007. Epub 2017 May 10 [PubMed PMID: 28584681]
Level 3 (low-level) evidenceHarland TA, Winston KR, Jovanovich AJ, Johnson RJ. Shunt Nephritis: An Increasingly Unfamiliar Diagnosis. World neurosurgery. 2018 Mar:111():346-348. doi: 10.1016/j.wneu.2018.01.017. Epub 2018 Jan 8 [PubMed PMID: 29325951]
Satoskar AA, Parikh SV, Nadasdy T. Epidemiology, pathogenesis, treatment and outcomes of infection-associated glomerulonephritis. Nature reviews. Nephrology. 2020 Jan:16(1):32-50. doi: 10.1038/s41581-019-0178-8. Epub 2019 Aug 9 [PubMed PMID: 31399725]
Turkis OF, Karadag A, Middlebrooks EH, Senoglu M. Anal Extrusion of a Ventriculoperitoneal Shunt. Journal of the College of Physicians and Surgeons--Pakistan : JCPSP. 2019 May:29(5):478-480. doi: 10.29271/jcpsp.2019.05.478. Epub [PubMed PMID: 31036124]
Bansal H, Gupta G, Gupta M, Kaushal R. Unusual Ventriculoperitoneal (VP) Shunt Tube Extrusion through Anus in a Child with Dandy Walker Malformation: A Rare Case Report. Journal of clinical and diagnostic research : JCDR. 2015 Jan:9(1):PD25-6. doi: 10.7860/JCDR/2015/11354.5488. Epub 2015 Jan 1 [PubMed PMID: 25738035]
Level 3 (low-level) evidenceBrownlee JD, Brodkey JS, Schaefer IK. Colonic perforation by ventriculoperitoneal shunt tubing: a case of suspected silicone allergy. Surgical neurology. 1998 Jan:49(1):21-4 [PubMed PMID: 9428890]
Level 3 (low-level) evidenceJunaid M, Ahmed M, Rashid MU. An experience with ventriculoperitoneal shunting at keen's point for hydrocephalus. Pakistan journal of medical sciences. 2018 May-Jun:34(3):691-695. doi: 10.12669/pjms.343.14081. Epub [PubMed PMID: 30034441]
Nakajima M, Miyajima M, Ogino I, Akiba C, Kawamura K, Kurosawa M, Kuriyama N, Watanabe Y, Fukushima W, Mori E, Kato T, Sugano H, Karagiozov K, Arai H. Shunt Intervention for Possible Idiopathic Normal Pressure Hydrocephalus Improves Patient Outcomes: A Nationwide Hospital-Based Survey in Japan. Frontiers in neurology. 2018:9():421. doi: 10.3389/fneur.2018.00421. Epub 2018 Jun 7 [PubMed PMID: 29942280]
Level 3 (low-level) evidenceTavares PAJ, Hamamoto Filho PT, Ferreira ASSBS, Avila MAG. Construction and Validation of Educational Material for Children with Hydrocephalus and Their Informal Caregivers. World neurosurgery. 2018 Jun:114():381-390. doi: 10.1016/j.wneu.2018.03.082. Epub 2018 Mar 19 [PubMed PMID: 29567289]
Level 1 (high-level) evidenceJoseph RA, Killian MR, Brady EE. Nursing Care of Infants With a Ventriculoperitoneal Shunt. Advances in neonatal care : official journal of the National Association of Neonatal Nurses. 2017 Dec:17(6):430-439. doi: 10.1097/ANC.0000000000000439. Epub [PubMed PMID: 29166295]
Level 3 (low-level) evidence