Introduction
Abdominal Aortic Aneurysms (AAAs) are a relatively common pathology with a prevalence of 1.3% in patients over 50 years and an incidence in elderly men over 12%.[1] Ruptured aneurysms have an exceptionally high mortality rate ranging 50% to 95%. In fact, mortality increases by 1% with each subsequent minute, mandating prompt diagnosis and intervention. Nearly 30% of ruptured AAAs are misdiagnosed on initial presentation. Physical examination has poor sensitivity of less than 65%. Moreover, less than 25% of patients present with the characteristic triad of hypotension, abdominal pain, and a pulsatile abdominal mass.[2][3][4]
Prompt diagnosis by utilizing point of care ultrasound has demonstrated sensitivities of 94% to 99%. Costantino et al. confirmed that bedside ultrasound is accurate within 4 millimeters of CT measurements with respect to AAA. Bedside ultrasound is a safe and effective diagnostic imaging modality that can be performed in under 5 minutes. More significantly, its use has decreased mortality by 20% to 60%.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The retroperitoneal abdominal aorta enters the abdomen via the aortic hiatus caudal to the xiphoid process. It rests anterior to the vertebral body and parallel to the inferior vena cava. Extending about 1 to 2 centimeters below the umbilicus, the aorta divides into the common iliac arteries at the level of L4. The aorta diminishes in size as it descends through the abdominal cavity, moving more superficially as well. As it moves caudally, the aorta has consecutive arterial branches: the celiac, superior mesenteric, renal, gonadal, and the inferior mesenteric.
An aneurysm is classified as a focal dilatation greater than 50% of a vessel’s normal diameter. A diameter greater than 3 centimeters demarcates an AAA. Two categories of AAAs exist: fusiform and saccular. The majority are fusiform. Fusiform aneurysms expand circumferentially. Whereas saccular aneurysms are localized outpouchings, often secondary to an infectious etiology.
Approximately 90% of AAAs occur infrarenal, although the renal vessels are often difficult to image with a point of care ultrasound. Scan to where the aorta bifurcates to confirm visualization of the aorta in its entirety.[5][6][7][8]
Indications
Who to Scan?
It is important to remember that less than 25% of individuals present with the classic triad of hypotension, abdominal pain, and a pulsatile abdominal mass.
Consider sonographic assessment of the abdominal aorta in the following instances:
- Greater than 50 years old with one of the following: chest, abdominal, flank, groin, or back pain; renal colic; hematuria; or hydronephrosis
- Cardiac Arrest
- Hypotension
- Syncope
- Thromboembolic events to the lower extremities
- Neurologic deficit of the lower extremities
Expert consensus regarding sonographic screening for AAAs in asymptomatic individuals includes the following.
The United States Preventative Services Task Force (USPSTF) & the American Academy of Family Physicians (AAFP) recommendations:
- Men greater than 65 years who ever smoked
Society for Vascular Surgery recommendations:
- All men age greater than 65
- Men greater than 55 with a family history of AAA
- Women greater than 65 with family history of AAA or who have ever smoked
Risk Factors
- Greater than 50 years old
- Family history of AAA
- Male
- Hypertension
- Smoking
- Coronary artery disease
- Diabetes mellitus
- Hyperlipidemia
- Peripheral arterial disease
Contraindications
There are no known contraindications for the sonographic assessment of the abdominal aorta.
Equipment
Sonographic assessment of the aorta is performed in real time B-mode imaging programmed with the abdominal settings. The curvilinear transducer is ideal given its lower frequency and deeper penetration. However, the phased array transducer can be employed as well. Occasionally, the linear probe can provide significant detail in thin individuals.
Preparation
Similar to any sonographic examination, the appropriate configuration is necessary to acquire detailed images of the abdominal aorta. Place the patient in the supine position with the bed adjusted to the level of the provider’s waist. Darken the room and apply sufficient gel.
Initially, maximize the depth to visualize the most important landmark, the vertebral body. It should be hyperechoic with posterior shadowing. Once identified, adjust the depth accordingly to enhance your image. Particularly, as you scan inferiorly towards the umbilicus, the aorta moves to a more superficial position, and less depth is needed.
Continuous, firm pressure will displace impeding bowel gas; and adjustments to the gain will reduce artifact. Modify the probe angle or move slightly off midline. Then angle or rock back medially to improve image acquisition. Or slide caudal to hindering bowel and then tilt cephalad to enhance sonographic visualization. The opposite technique works similarly. Finally, turn the patient into the left lateral decubitus position. This may improve your images as well. Nevertheless, the aorta will not be visible in 5% of individuals. In these instances, advanced diagnostic imaging modalities, such as CTA or MRA, will supplement the evaluation.[9][10][11]
Technique or Treatment
To begin, place the transducer below the xiphoid process in the transverse alignment. Perform a complete scan through the bifurcation of the aorta around the level of the umbilicus. Several consecutive videos may be necessary to image the entire aorta. Measure the abdominal aorta at its maximal diameter to include each outer wall. Dimensions are most precise with the probe positioned completely perpendicular to the aorta. Perform a similar scan in the sagittal view with the transducer position towards the patient’s head.
Be sure to include any visible thrombus. Thrombus will appear as an echogenic substance within the aorta. However, it is easily overlooked. Generally, it is best visualized along the anterolateral wall and may create a false lumen that underestimates the actual extent of an aortic aneurysm.
In unstable patients, providers should routinely complete a right upper quadrant ultrasound to evaluate for pathologic fluid. The majority of AAAs rupture in the retroperitoneum (70% to 90%), where ultrasound cannot assess routinely. Nevertheless, one study established a sensitivity of 97% for identifying ruptured AAAs when point of care ultrasound was combined with clinical gestalt.
Lastly, sonographic assessment of the aorta includes assessing for the occurrence of an undulating intimal flap, the pathognomonic finding that is 100% specific for aortic dissections. Strict blood pressure management and emergent surgical consultation are mandated.
Complications
There are no known complications from the sonographic assessment of the abdominal aorta. Limitations include body habitus, bowel gas, and operator experience. In lieu of a limited evaluation of the abdominal aorta, consider advanced imaging based on the patient's hemodynamic status.
Clinical Significance
More than 90% of abdominal aortic aneurysms occur below the renal arteries. By scanning to the level of the bifurcation, providers ensure complete visualization of the aorta.
Do not overlook an intraluminal thrombus. Include the thrombus to measure the diameter accurately.
Identify intimal flaps, which are pathognomonic for aortic dissections.
It can be difficult to differentiate the IVC from the aorta. Generally, the pulsatile aorta is thick walled, non-compressible, and positioned medial to the IVC. The IVC is thin-walled and compressible. It may appear to pulsate given its proximity to the aorta and secondary to the normal respiratory cycle. Use pulsed-wave Doppler to delineate the aorta’s pulsatile flow from the venous flow of the inferior vena cava, which should display mild respirophasic variation only.
Although the majority are retroperitoneal, when concerned for a ruptured AAA, perform a right upper quadrant ultrasound to assess for pathologic free fluid.
Enhancing Healthcare Team Outcomes
The diagnosis and management of an AAA includes an interprofessional team consisting of a radiologist, vascular surgeon, internist, nurse practitioner, and cardiologist. When an AAA is suspected the initial test of choice is ultrasound. This diagnostic imaging modality permits routine monitoring of patients who are managed non-surgically, while limiting radiation and IV contrast exposure. An MRA or CTA is recommended for surgical planning if the patient is hemodynamically stable. Unstable patients should be managed in close consultation with the vascular surgeon and intensivist.
Media
(Click Image to Enlarge)
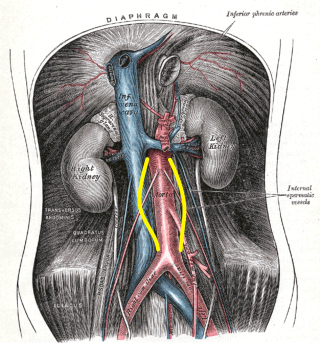
Abdominal Aortic Aneurysm, Illustration. Distention is shown by the yellow markings. This illustration also shows the aorta, inferior vena cava, and aneurysms.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
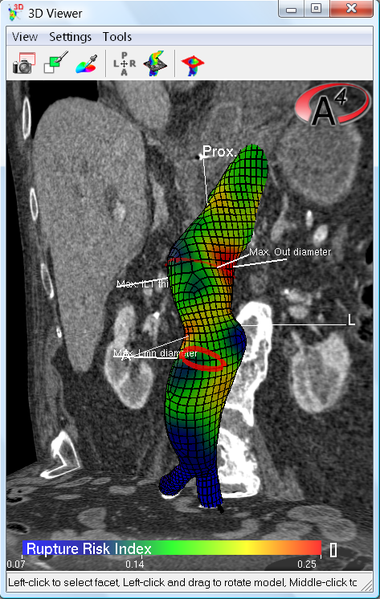
Color coded plot of the rupture risk index of the aneurysm wall, Red portions are closest to the limit load (strength) of the wall, Abdominal Aortic Aneurysm, AAA Contributed by Wikimedia Commons (Public Domain)
(Click Video to Play)
Point of Care Ultrasound of the Inferior Vena Cava and Abdominal Aorta. This ultrasound video shows the inferior vena cava, the collapsible vessel posterior and right (of the patient, left on this view), and the abdominal aorta, the persistently round vessel anterior and left (of the patient, right on this view.
Contributed by Ryan Gibbons, MD FAAEM
(Click Image to Enlarge)
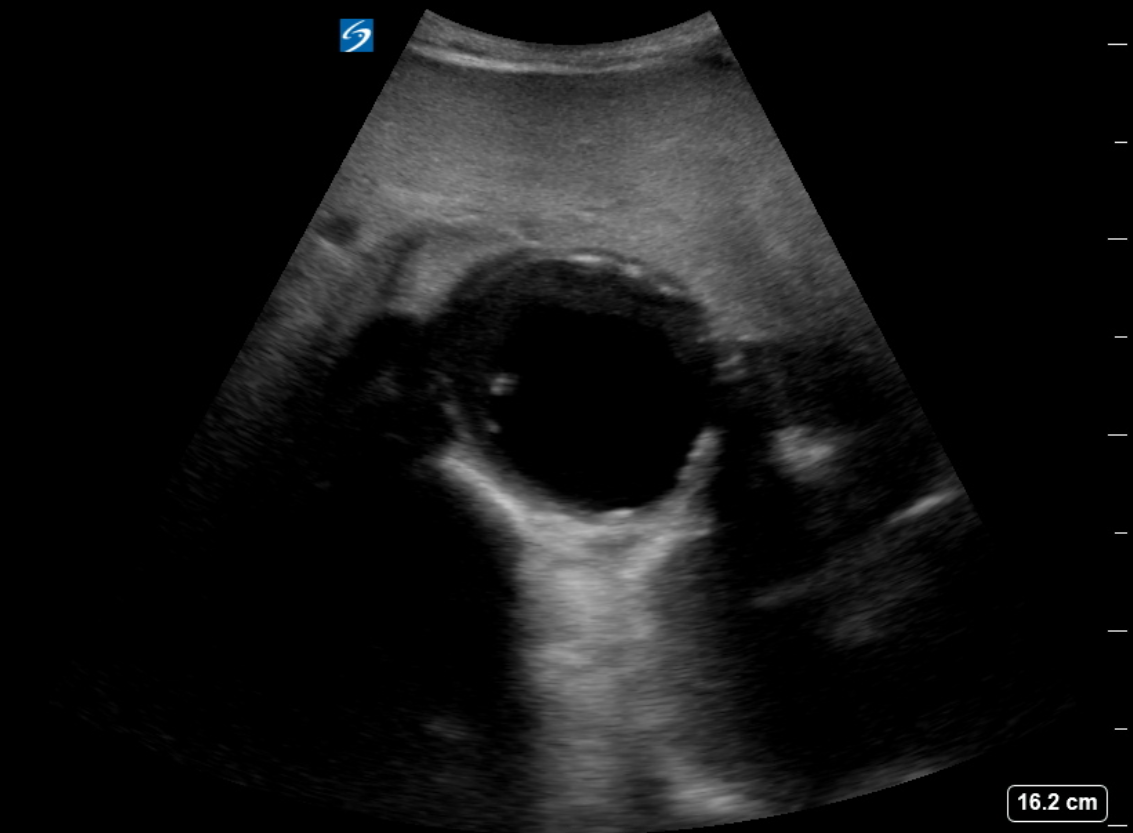
Abdominal Aortic Aneurysm, Ultrasound. The diagnosis of an abdominal aortic aneurysm is usually made using ultrasound.
Contributed by K Burns, MD
(Click Image to Enlarge)
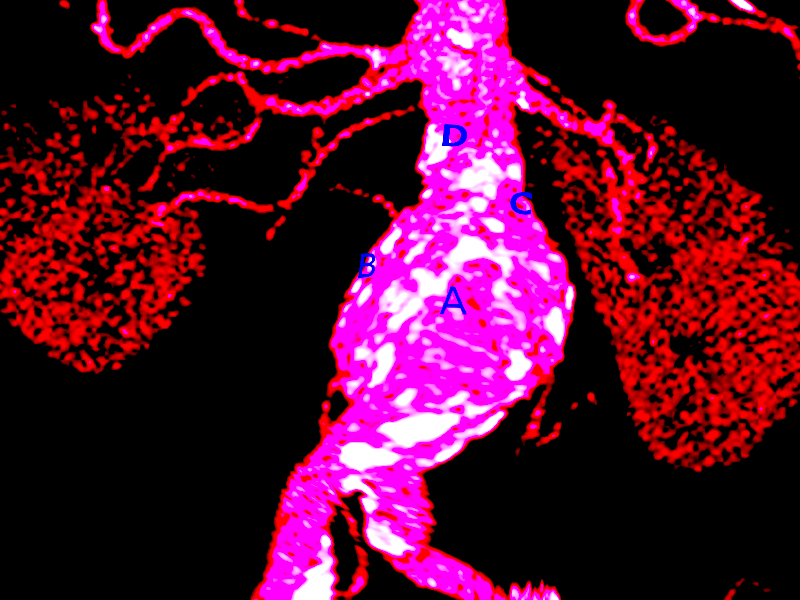
Abdominal Aortic Aneurysm Rupture
Contributed by S Bhimji, MD
References
Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, Hiratzka LF, Murphy WR, Olin JW, Puschett JB, Rosenfield KA, Sacks D, Stanley JC, Taylor LM Jr, White CJ, White J, White RA, Antman EM, Smith SC Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Hunt SA, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B, American Association for Vascular Surgery, Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, ACC/AHA Task Force on Practice Guidelines Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease, American Association of Cardiovascular and Pulmonary Rehabilitation, National Heart, Lung, and Blood Institute, Society for Vascular Nursing, TransAtlantic Inter-Society Consensus, Vascular Disease Foundation. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006 Mar 21:113(11):e463-654 [PubMed PMID: 16549646]
Level 3 (low-level) evidenceRouet L, Dufour C, Collet Billon A, Bredahl K. CT and 3D-ultrasound registration for spatial comparison of post-EVAR abdominal aortic aneurysm measurements: A cross-sectional study. Computerized medical imaging and graphics : the official journal of the Computerized Medical Imaging Society. 2019 Apr:73():49-59. doi: 10.1016/j.compmedimag.2019.02.004. Epub 2019 Mar 2 [PubMed PMID: 30889540]
Level 2 (mid-level) evidenceCebull HL, Soepriatna AH, Boyle JJ, Rothenberger SM, Goergen CJ. Strain Mapping From Four-Dimensional Ultrasound Reveals Complex Remodeling in Dissecting Murine Abdominal Aortic Aneurysms. Journal of biomechanical engineering. 2019 Jun 1:141(6):. pii: 060907. doi: 10.1115/1.4043075. Epub [PubMed PMID: 30840030]
Zagrapan B, Eilenberg W, Prausmueller S, Nawrozi P, Muench K, Hetzer S, Elleder V, Rajic R, Juster F, Martelanz L, Hayden H, Klopf J, Inan C, Teubenbacher P, Weigl MP, Kirchweger P, Beitzke D, Jilma B, Wojta J, Bailey MA, Scott DJA, Huk I, Neumayer C, Brostjan C. A Novel Diagnostic and Prognostic Score for Abdominal Aortic Aneurysms Based on D-Dimer and a Comprehensive Analysis of Myeloid Cell Parameters. Thrombosis and haemostasis. 2019 May:119(5):807-820. doi: 10.1055/s-0039-1679939. Epub 2019 Mar 1 [PubMed PMID: 30822810]
Kazimierczak W, Serafin Z, Kazimierczak N, Ratajczak P, Leszczyński W, Bryl Ł, Lemanowicz A. Contemporary imaging methods for the follow-up after endovascular abdominal aneurysm repair: a review. Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques. 2019 Jan:14(1):1-11. doi: 10.5114/wiitm.2018.78973. Epub 2018 Oct 15 [PubMed PMID: 30766622]
Drelich-Zbroja A, Sojka M, Kuczyńska M, Światłowski Ł, Kuklik E, Sobstyl J, Pyra K, Wolski A, Czekajska-Chehab E, Pech M, Powerski M, Jargiełło T. Diagnostic imaging in patients after endovascular aortic aneurysm repair with special focus on ultrasound contrast agents. Polish archives of internal medicine. 2018 Dec 29:129(2):80-87. doi: 10.20452/pamw.4409. Epub 2018 Dec 29 [PubMed PMID: 30600308]
Brazzelli M, Hernández R, Sharma P, Robertson C, Shimonovich M, MacLennan G, Fraser C, Jamieson R, Vallabhaneni SR. Contrast-enhanced ultrasound and/or colour duplex ultrasound for surveillance after endovascular abdominal aortic aneurysm repair: a systematic review and economic evaluation. Health technology assessment (Winchester, England). 2018 Dec:22(72):1-220. doi: 10.3310/hta22720. Epub [PubMed PMID: 30543179]
Level 1 (high-level) evidenceGolledge J. Abdominal aortic aneurysm: update on pathogenesis and medical treatments. Nature reviews. Cardiology. 2019 Apr:16(4):225-242. doi: 10.1038/s41569-018-0114-9. Epub [PubMed PMID: 30443031]
Sachsamanis G, Charisis N, Maltezos K, Galyfos G, Papapetrou A, Tsiliggiris V, Kantounakis I, Tzilalis V. Management and therapeutic options for abdominal aortic aneurysm coexistent with horseshoe kidney. Journal of vascular surgery. 2019 Apr:69(4):1257-1267. doi: 10.1016/j.jvs.2018.10.009. Epub 2018 Dec 24 [PubMed PMID: 30591298]
Sakalihasan N, Michel JB, Katsargyris A, Kuivaniemi H, Defraigne JO, Nchimi A, Powell JT, Yoshimura K, Hultgren R. Abdominal aortic aneurysms. Nature reviews. Disease primers. 2018 Oct 18:4(1):34. doi: 10.1038/s41572-018-0030-7. Epub 2018 Oct 18 [PubMed PMID: 30337540]
Thompson SG, Bown MJ, Glover MJ, Jones E, Masconi KL, Michaels JA, Powell JT, Ulug P, Sweeting MJ. Screening women aged 65 years or over for abdominal aortic aneurysm: a modelling study and health economic evaluation. Health technology assessment (Winchester, England). 2018 Aug:22(43):1-142. doi: 10.3310/hta22430. Epub [PubMed PMID: 30132754]
Liu H,IJpma AS,de Bruin JL,Verhagen HJM,Roos-Hesselink JW,Bekkers JA,Brüggenwirth HT,van Beusekom HMM,Majoor-Krakauer D, Whole aorta imaging shows increased risk for thoracic aortic aneurysms and dilatations in relatives of abdominal aortic aneurysm patients. Journal of vascular surgery. 2024 Oct 26; [PubMed PMID: 39490460]