Introduction
Truncus arteriosus is a rare, congenital, cyanotic cardiac anomaly characterized by a ventricular septal defect (VSD), a single truncal valve, and a common ventricular outflow tract. Systemic and pulmonary venous blood mix at the VSD and desaturated blood is ejected into the outflow tract. The pulmonary arteries arise directly from the truncus. Thus, pulmonary vascular resistance (PVR) determines the amount of pulmonary blood flow (PBF). Death in infancy is probable without surgical intervention. Long-term surgical outcomes are positive, but residual and potential complications require long-term cardiology follow-up.[1][2]
Anatomy
The most salient pathologic finding in truncus arteriosus is the absence of an aorticopulmonary septum (21%). However, the most common truncus arteriosus type is a partially formed aorticopulmonary septum (50%).[3] The typical semilunar valve may have 1 to 4 cusps, usually 3 (see Image. Truncus Arteriosus Embryologic Origin). The presence of a single arterial trunk may be associated with several cardiac, aortic, and pulmonary abnormalities. In order of frequency, aortic arch anomalies may include a right-sided, interrupted, or hypoplastic aortic arch with or without coarctation of the aorta.
Coronary origin is usually abnormal and follows no specific pattern.[4] The pulmonary arteries are abnormal, ranging from a single small trunk to the left of the aortic root to originating at various locations from within the aortic root or a patent ductus arteriosus (PDA).[5] Other cardiac defects that may coexist with a truncus arteriosus include secundum atrial septal defects, aberrant subclavian artery, persistent left superior vena cava with drainage into the coronary sinus, and PDA.[6]
Classification
Collett and Edwards and Van Praagh each classified the various forms of truncus arteriosus. Collett and Edwards based their system solely on the origins of the pulmonary vascular system (see Image. Collett and Edwards' Truncus Arteriosus Classification), while Van Praagh also considered aortic abnormalities.[7][8][9][10][11]
The Collett and Edwards classification includes the following subtypes of truncus arteriosus:
- Type I: A main pulmonary trunk arising from the truncal root
- Type II: Right and left branch pulmonary arteries have close but separate origins from the truncal root's posterior aspect
- Type III: Right and left branch pulmonary arteries have separate origins, also from the truncal root
- Type IV: Right and left branch pulmonary arteries originate from the descending aorta
Collett and Edwards Type IV truncus arteriosus is currently considered a form of pulmonary atresia. This differentiation emphasizes the specific developmental irregularities in each condition, distinguishing between truncus arteriosus' characteristic septation abnormalities and pulmonary atresia's subpulmonary myocardial developmental anomalies.[12][13]
Meanwhile, the Van Praagh classification includes the following truncus arteriosus subtypes:
- Type A1: A main pulmonary trunk arises from the truncal root, as in Collett and Edwards Type I. This type has a partially formed aorticopulmonary septum and is the most common (50%).
- Type A2: The right and left branch pulmonary arteries have separate origins, like Collett and Edwards Types II and III. The aorticopulmonary septum is absent. This type is the second most common form of truncus arteriosus (21%).
- Type A3: This category has unilateral pulmonary branch atresia. Blood flow to the affected lung tissue is facilitated through collateral vessels originating from the aortic arch or other collateral arteries.
- Type A4: This type has an aortic arch interruption, most commonly between the left common carotid and subclavian arteries.[14]
The Society of Thoracic Surgeons classifies truncus arteriosus into 3 categories by modifying the Van Praagh classification as follows:
- Truncus arteriosus with confluent or near confluent branch pulmonary arteries (includes Van Praagh types A1 and A2)
- Truncus arteriosus with the absence of one branch pulmonary artery (same as Van Praagh type A3)
- Truncus arteriosus with interrupted aortic arch or coarctation (same as Van Praagh type A4) [15]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Truncus arteriosus arises if embryological processes fail to create a conotruncal septal wall, and the single truncal root does not divide into the aortic and pulmonic outflow tracts. This mechanism also inhibits the formation of separate aortic and pulmonary valves, resulting in a single truncal valve (see Image. Truncus Arteriosus Pathology).[16]
While the developmental underpinnings are poorly understood, truncus arteriosus is frequently associated with 22q11.2 microdeletion (Di George) syndrome in 12% to 35% of patients. Abnormalities in the secondary heart field and cardiac neural crest cells are likewise strongly implicated.[17][18]
Epidemiology
Truncus arteriosus has an annual incidence of 7 per 100,000 live births. While the condition accounts for less than 1% of all congenital heart lesions, truncus arteriosus accounts for approximately 4% of critical congenital heart defects.[19]
Pathophysiology
In truncus arteriosus, systemic venous blood returns to the right atrium and flows into the right ventricle. The pulmonary veins carry oxygenated pulmonary venous blood into the left atrium, which empties into the left ventricle. The VSD enables the mixing of oxygenated and deoxygenated blood before ejecting through a common truncal valve to a single artery, supplying the coronary, pulmonary, and systemic circulations.
The mixing of pulmonary and systemic blood and variations in pulmonary blood flow and PVR initiate the pathophysiologic mechanisms of truncus arteriosus. PVR is relatively high starting the 1st week of life. Shunting of mixed oxygenated and deoxygenated blood into the systemic circuit increases, causing mild cyanosis. Pulmonary overcirculation causes congestive heart failure as PVR drops and PBF rises. If untreated, pulmonary overcirculation eventually leads to irreversible pulmonary vascular disease with fixed pulmonary hypertension or Eisenmenger syndrome.[20][21]
History and Physical
History
The severity of pulmonary blood flow variations, semilunar valvular abnormalities, and aortic arch obstruction drives the clinical picture. Birth history may reveal cyanosis or respiratory distress soon after delivery, prompting further evaluation. The critical congenital heart defect screen within the first few days after birth might show mild or moderate desaturation. Unscreened infants may present within the first 2 weeks with symptoms of congestive heart failure resulting from increased blood flow to the lungs as PVR naturally decreases. These infants may exhibit poor feeding, failure to thrive, lethargy, tachypnea, costosternal retractions, grunting, nasal flaring, tachycardia, hepatomegaly, and persistent cyanosis despite oxygen therapy.
Patients with truncus arteriosus often have a prenatal history that may include abnormal cardiac findings on fetal ultrasound or echocardiography. Additionally, there might be a family history of congenital heart disease or genetic syndromes associated with cardiac anomalies. Previous medical history may include cardiac interventions or surgeries. Developmental milestones should be carefully assessed, as some patients may have delays or neurodevelopmental abnormalities associated with the underlying condition.
Physical Examination
On physical examination, patients may exhibit respiratory distress on room air. Jugular venous distension may be present. Examination of the extremities may reveal clubbing and cyanosis. Abdominal assessment may demonstrate hepatomegaly. Other congenital anomalies, such as facial abnormalities and musculoskeletal defects, may be noted if truncus arteriosus is only part of a syndrome.
The cardiac exam is notable for a harsh holosystolic murmur, an ejection click, a single loud second heart sound, and a diastolic murmur if truncal valve regurgitation is present. Peripheral pulses may be bounding due to excess runoff into the pulmonary arteries. An increased pulmonary vascular flow during diastole may correlate with higher pulse pressures.[22][23] Valvular insufficiency and stenosis are common phenomena. Valvular regurgitation, seen in 50% of patients, can worsen symptoms of CHF. Concurrent critical coarctation, seen in 10% of patients with truncus arteriosus or aortic arch interruption, can lead to cardiovascular collapse, with patients presenting in shock or death.[24]
Evaluation
Prenatal diagnosis by fetal echocardiography is usually performed at 22 weeks of gestation on average and as early as 13 weeks of gestation. The imaging modality typically visualizes a single arterial outflow tract, a significant VSD, and the origin of the main pulmonary artery or its supposed branches from the truncal root. Genetic testing is usually performed during pregnancy because of the condition's frequent association with 22q11.2 deletion. Prenatal diagnosis facilitates delivery at an appropriate facility, enabling immediate postnatal echocardiography and initiation of necessary treatment.[25]
Postnatal diagnosis is ascertained with a transthoracic echocardiogram showing the lesion's precise anatomy and type. Occasionally, cardiac magnetic resonance imaging (MRI) or computed tomography angiography (CTA) is used to evaluate coronary artery anatomy and branch pulmonary arteries, especially in Van Praagh Type A3. This modality also helps determine whether aortic interruption or coarctation is present, which is pertinent to surgical planning. Postoperatively, CTA helps evaluate the pulmonary homograft and pulmonary artery anatomy for recurrent or residual stenosis.[26] Cardiac catheterization is mainly reserved for interventions, such as balloon angioplasty or stenting to dilate narrowed pulmonary arteries between surgical procedures.[27]
Treatment / Management
The initial management involves stabilizing the patient and balancing blood flow through the pulmonary and systemic circuits. Interventions should maintain stable ductal patency in patients with interrupted aortic arch. Care is typically provided in a neonatal (NICU) or cardiac intensive care unit (CICU).
Pulmonary Congestive Heart Failure Treatment
Loop and thiazide diuretics are used to help achieve proper fluid balance. These treatments reduce excess volume, filling pressure, and pulmonary congestion to improve left ventricle failure. These diuretics also improve right ventricle failure by maintaining control of systemic venous congestion.
Patients in respiratory distress may require additional positive-pressure support, eg, continuous positive airway pressure, synchronized intermittent positive airway pressure, or endotracheal intubation. Supplemental oxygen is to be avoided as pulmonary overcirculation may worsen. Metabolic derangements, electrolyte abnormalities, hypoglycemia, and anemia should be corrected to prevent worsening heart failure.[28](A1)
Prostaglandin Infusion
Prostaglandins promote ductal patency if a concurrent aortic arch anomaly exists. Maintaining ductal patency is crucial for ensuring adequate systemic blood flow.
Definitive Surgical Correction
Definitive surgical correction may be performed as a single-stage repair within the 1st month of life. The procedure is indicated for truncus arteriosus without truncal valve or aortic arch abnormality. Pulmonary artery mobilization from the truncus to the right ventricle, conduit-based right ventricular outflow tract reconstruction, and VSD patch closure are performed within the same operation. Aortic arch abnormalities and the truncal valve are also fixed.
Primary palliation with pulmonary arterial banding and delayed surgical repair may be required to allow the infant to grow. However, this 2-stage correction is not routinely recommended due to higher morbidity and mortality rates.[29][30]
Immediate Postoperative Care
The postoperative patient is taken to the CICU for close monitoring and stabilization. Fluid and electrolyte management, sedation and pain control, respiratory control, cardiovascular management, renal function, neurological status, infection control, and nutritional status are all important factors to consider during the postoperative period.
Both noninvasive and invasive methods are utilized for continuous monitoring in the CICU. While noninvasive monitoring includes basic parameters such as heart rate, respiratory rate, and oxygen saturation, invasive modalities like pulmonary and atrial catheters and central and arterial lines provide detailed cardiopulmonary information.[31]
Differential Diagnosis
New technological advances have improved the rate of diagnosing truncus arteriosus prenatally to greater than 90%. However, truncus arteriosus may be misdiagnosed as pulmonary atresia with a VSD if structures and aortopulmonary collaterals cannot be correctly identified on prenatal echocardiography.[32][33][34] Other differential diagnoses for a single outflow tract ventricle include a double outlet right ventricle with pulmonary and aortic atresia.[35]
Prognosis
Without the recommended single-stage repair, patients often die before 2 months of age. The 1-year survival rate for patients who do not undergo surgery is less than 20%. By age 4, pulmonary vascular obstructive disease is so severe that surgery is futile, and patients die before the 2nd decade due to cardiac failure. After the primary repair, patients have a 20-year survival rate of over 80%, but the reoperation rate remains high. Therefore, long-term follow-up is recommended.[36]
Complications
Complications associated with truncus arteriosus before surgical intervention are related to associated extracardiac conditions. Many patients with truncus arteriosus have Di George syndrome's 22q11.2 deletion. These patients may present with neonatal seizures from hypocalcemia secondary to parathyroid hypoplasia. Thymic hypoplasia can make older infants with this genetic condition susceptible to viral, fungal, and bacterial infections.
Postoperative complications usually occur within the first 48 hours and include pulmonary hypertensive crisis and low cardiac output syndrome. Decreased manipulation and mobilization of patients may reduce the risk of pulmonary hypertensive crisis during the immediate postoperative phase. Right bundle branch block and arrhythmias such as supraventricular tachycardia can occur. Complications requiring surgical reintervention in the immediate postoperative period include mediastinal bleeding, pleural effusion, pneumothorax, and cardiac tamponade.
Problems common after any surgery include seizures and other nervous system injuries, prolonged bleeding times, and renal failure. Reinterventions are inevitable as patients outgrow their right ventricular pulmonary artery conduit or the truncal valve insufficiency worsens. By the 10th postoperative year, approximately 75% of patients require a reintervention, with the most frequent procedures being right ventricle outflow tract reconstruction and valve repair or replacement with relief of aortic obstruction.[37][38]
Deterrence and Patient Education
Families of patients with truncus arteriosus should be referred for genetic counseling. This intervention informs individuals about truncus arteriosus' genetic factors, aiding in family planning decisions. Genetic counseling identifies at-risk individuals, enabling early prenatal testing to assess recurrence risk in future pregnancies.
Lifelong follow-up with a congenital heart disease specialist should be emphasized to all patients. In the long term, patients and clinicians should pay close attention to changes in exercise tolerance, history of palpitations or syncope, or the emergence of edema and dyspnea. Any diastolic murmur should be noted as a sign of valve insufficiency or conduit regurgitation. Pulmonary congestion and peripheral edema may signify congenital heart failure. Elevated jugular venous pulse or hepatomegaly may indicate increasing right heart pressure.
Routine testing with serial echocardiography is recommended to evaluate the right ventricular pulmonary artery connection, biventricular function, and truncal valve stenosis or insufficiency. Patients with decreased exercise tolerance, congestive symptoms, or arrhythmia require frequent evaluations with electrocardiography, heart rate monitors, echocardiography, and stress testing. MRI or CT may help assess for conduit obstruction, valve regurgitation, cardiac function, and the presence of myocardial fibrosis.[39]
Patients with congenital heart disease are at risk for mental health issues in adulthood.[40] The magnitude of these outcomes is inversely related to the patient's functional status.[41] Interdisciplinary teams improve the quality of life for patients with congenital heart disease, which pediatric and adult congenital heart clinicians are currently advocating.[42]
Pearls and Other Issues
Truncus arteriosus presents with a single arterial trunk originating from the heart, often with a VSD. Echocardiography is the best initial imaging modality, though cardiac catheterization and advanced imaging can give additional diagnostic insights. Surgery is the only definitive treatment for patients with truncus arteriosus requiring repeat interventions. Mortality is high within the 1st year of life without surgery. Patients usually still require multiple cardiac reinterventions postoperatively. Thus, long-term follow-up with a congenital heart disease specialist is advised. Genetic counseling informs families about associated genetic factors and assists in reproductive decisions.
Enhancing Healthcare Team Outcomes
An interprofessional approach to patients with truncus arteriosus is recommended to improve outcomes.[43] Team-based healthcare delivery starts early after conception, involving high-risk obstetricians and fetal cardiac imaging specialists. After delivery, timely surgical reintervention or transcatheter intervention significantly enhances outcomes. Given the condition's common association with 22q11.2 microdeletion syndrome and the need for neonatal open-heart surgery, a team-based approach should include a pediatric cardiologist, a pediatric cardiac surgeon, an intensivist, a geneticist, and a radiologist.[44] Specific team members are vital as patient care often occurs in a NICU or CICU.[45] Teams should include a charge nurse, bedside nurse, respiratory therapist, nutrition specialist, social worker, pharmacist, and x-ray technician.[46]
Children with congenital heart disease survive well into adulthood with increasing success in surgical and postoperative management and the advent of new technological advances. However, questions remain regarding health-related issues. These challenges include clinical care transitions, daily and competitive activity recommendations, medications and adherence, routine medical and dental care, proper insurance and healthcare provider acquisition, reproductive issues, education, and career planning. Clinicians should be aware that impairments in cognition, social interactions, communication skills, and executive functioning are well-documented in children with complex heart disease.[47] A specialist in adult congenital heart disease is ideal, but an electrophysiologist and interventional cardiologist may also be required.
Additionally, an internal medicine clinician may prove beneficial in coordinating required care with a high-risk obstetrician, neurologist, psychologist or psychiatrist, endocrinologist, and geneticist. Other critical members of the adult congenital heart disease team include nurses and nurse practitioners, physician assistants, cardiac anesthesiologists with training in congenital heart disease, a hepatologist, and a cardiac pathologist. Services that may be required include rehabilitation, psychological, social, and financial counselors. The smooth care transition to adult medicine is critical.[48]
Media
(Click Image to Enlarge)
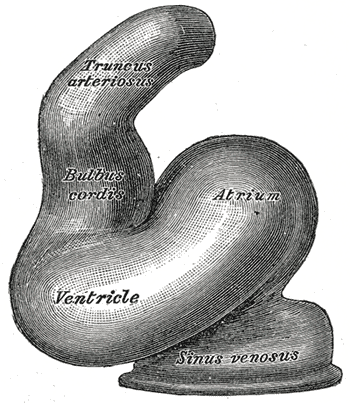
Truncus Arteriosus Embryologic Origin. Truncus arteriosus results from abnormal development of the embryonic outflow tract, where failure of septation leads to a single arterial trunk originating from the heart.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
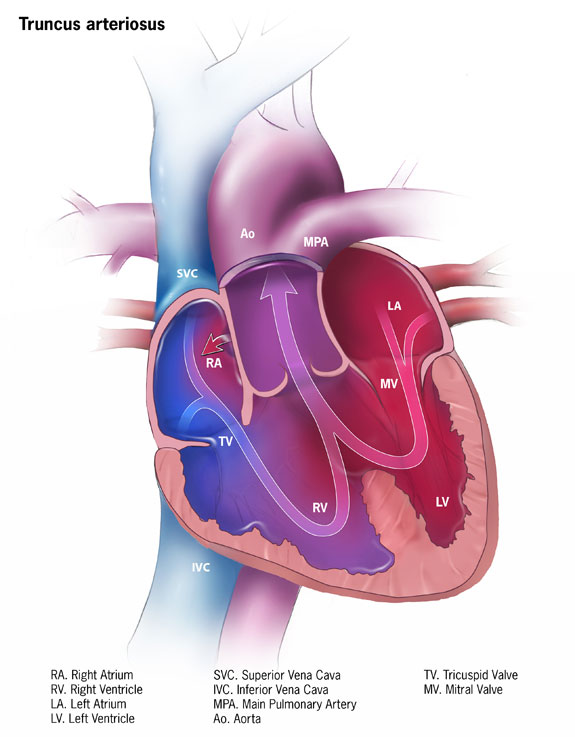
Truncus Arteriosus Pathology. The impact of truncus arteriosus on normal blood flow is illustrated as mixed oxygenated and deoxygenated blood sources.
Centers for Disease Control and Prevention, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
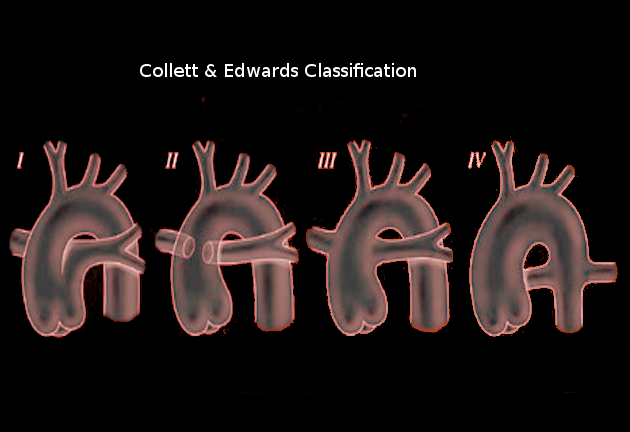
Collett and Edwards' Truncus Arteriosus Classification. This image shows Collett and Edwards' truncus arteriosus classification. The categories are based on the origin and course of the pulmonary arteries. Type I involves a single trunk arising from the heart, giving rise to both the aorta and pulmonary arteries. Type II features separate origins of the pulmonary arteries arising from the posterior aspect of the common trunk. Type III presents with the pulmonary arteries originating individually from the lateral aspects of the common trunk. Type IV, the rarest form, exhibits the pulmonary arteries arising separately from the aortic arch or descending aorta.
Contributed by O Chaigasame, MD
References
Chen Q, Gao H, Hua Z, Yang K, Yan J, Zhang H, Ma K, Zhang S, Qi L, Li S. Outcomes of Surgical Repair for Persistent Truncus Arteriosus from Neonates to Adults: A Single Center's Experience. PloS one. 2016:11(1):e0146800. doi: 10.1371/journal.pone.0146800. Epub 2016 Jan 11 [PubMed PMID: 26752522]
Level 2 (mid-level) evidencePuri K, Allen HD, Qureshi AM. Congenital Heart Disease. Pediatrics in review. 2017 Oct:38(10):471-486. doi: 10.1542/pir.2017-0032. Epub [PubMed PMID: 28972050]
Calder L, Van Praagh R, Van Praagh S, Sears WP, Corwin R, Levy A, Keith JD, Paul MH. Truncus arteriosus communis. Clinical, angiocardiographic, and pathologic findings in 100 patients. American heart journal. 1976 Jul:92(1):23-38 [PubMed PMID: 985630]
Shrivastava S, Edwards JE. Coronary arterial origin in persistent truncus arteriosus. Circulation. 1977 Mar:55(3):551-4 [PubMed PMID: 837493]
ANDERSON RC, OBATA W, LILLEHEI CW. Truncus arteriosus: clinical study of fourteen cases. Circulation. 1957 Oct:16(4):586-98 [PubMed PMID: 13461267]
Level 3 (low-level) evidenceBharati S, McAllister HA Jr, Rosenquist GC, Miller RA, Tatooles CJ, Lev M. The surgical anatomy of truncus arteriosus communis. The Journal of thoracic and cardiovascular surgery. 1974 Apr:67(4):501-10 [PubMed PMID: 4274217]
Lenox CC, Debich DE, Zuberbuhler JR. The role of coronary artery abnormalities in the prognosis of truncus arteriosus. The Journal of thoracic and cardiovascular surgery. 1992 Dec:104(6):1728-42 [PubMed PMID: 1453739]
Martin BJ, Karamlou TB, Tabbutt S. Shunt Lesions Part II: Anomalous Pulmonary Venous Connections and Truncus Arteriosus. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies. 2016 Aug:17(8 Suppl 1):S310-4. doi: 10.1097/PCC.0000000000000822. Epub [PubMed PMID: 27490615]
Konstantinov IE, Karamlou T, Blackstone EH, Mosca RS, Lofland GK, Caldarone CA, Williams WG, Mackie AS, McCrindle BW. Truncus arteriosus associated with interrupted aortic arch in 50 neonates: a Congenital Heart Surgeons Society study. The Annals of thoracic surgery. 2006 Jan:81(1):214-22 [PubMed PMID: 16368368]
Level 2 (mid-level) evidenceButto F, Lucas RV Jr, Edwards JE. Persistent truncus arteriosus: pathologic anatomy in 54 cases. Pediatric cardiology. 1986:7(2):95-101 [PubMed PMID: 3797293]
Level 3 (low-level) evidenceVan Praagh R. Truncus arteriosus: what is it really and how should it be classified? European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 1987:1(2):65-70 [PubMed PMID: 2856609]
COLLETT RW, EDWARDS JE. Persistent truncus arteriosus; a classification according to anatomic types. The Surgical clinics of North America. 1949 Aug:29(4):1245-70 [PubMed PMID: 18141293]
Kirby ML. Pulmonary atresia or persistent truncus arteriosus: is it important to make the distinction and how do we do it? Circulation research. 2008 Aug 15:103(4):337-9. doi: 10.1161/CIRCRESAHA.108.174862. Epub [PubMed PMID: 18703785]
Level 3 (low-level) evidenceVan Praagh R, Van Praagh S. The anatomy of common aorticopulmonary trunk (truncus arteriosus communis) and its embryologic implications. A study of 57 necropsy cases. The American journal of cardiology. 1965 Sep:16(3):406-25 [PubMed PMID: 5828135]
Level 3 (low-level) evidenceJacobs ML. Congenital Heart Surgery Nomenclature and Database Project: truncus arteriosus. The Annals of thoracic surgery. 2000 Apr:69(4 Suppl):S50-5 [PubMed PMID: 10798416]
Moorman A, Webb S, Brown NA, Lamers W, Anderson RH. Development of the heart: (1) formation of the cardiac chambers and arterial trunks. Heart (British Cardiac Society). 2003 Jul:89(7):806-14 [PubMed PMID: 12807866]
Pierpont ME, Brueckner M, Chung WK, Garg V, Lacro RV, McGuire AL, Mital S, Priest JR, Pu WT, Roberts A, Ware SM, Gelb BD, Russell MW, American Heart Association Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; and Council on Genomic and Precision Medicine. Genetic Basis for Congenital Heart Disease: Revisited: A Scientific Statement From the American Heart Association. Circulation. 2018 Nov 20:138(21):e653-e711. doi: 10.1161/CIR.0000000000000606. Epub [PubMed PMID: 30571578]
Yamagishi H. Clinical Developmental Cardiology for Understanding Etiology of Congenital Heart Disease. Journal of clinical medicine. 2022 Apr 24:11(9):. doi: 10.3390/jcm11092381. Epub 2022 Apr 24 [PubMed PMID: 35566507]
Level 3 (low-level) evidenceReller MD, Strickland MJ, Riehle-Colarusso T, Mahle WT, Correa A. Prevalence of congenital heart defects in metropolitan Atlanta, 1998-2005. The Journal of pediatrics. 2008 Dec:153(6):807-13. doi: 10.1016/j.jpeds.2008.05.059. Epub 2008 Jul 26 [PubMed PMID: 18657826]
Marcelletti C, McGoon DC, Mair DD. The natural history of truncus arteriosus. Circulation. 1976 Jul:54(1):108-11 [PubMed PMID: 1277412]
Niwa K, Perloff JK, Kaplan S, Child JS, Miner PD. Eisenmenger syndrome in adults: ventricular septal defect, truncus arteriosus, univentricular heart. Journal of the American College of Cardiology. 1999 Jul:34(1):223-32 [PubMed PMID: 10400015]
TAUSSIG HB. Clinical and pathological findings in cases of truncus arteriosus in infancy. The American journal of medicine. 1947 Jan:2(1):26-34 [PubMed PMID: 20278447]
Level 3 (low-level) evidenceTANDON R, HAUCK AJ, NADAS AS. PERSISTENT TRUNCUS ARTERIOSUS. A CLINICAL, HEMODYNAMIC, AND AUTOPSY STUDY OF NINETEEN CASES. Circulation. 1963 Dec:28():1050-60 [PubMed PMID: 14082918]
Level 3 (low-level) evidenceTlaskal T, Hucin B, Kucera V, Vojtovic P, Gebauer R, Chaloupecky V, Skovranek J. Repair of persistent truncus arteriosus with interrupted aortic arch. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2005 Nov:28(5):736-41 [PubMed PMID: 16194613]
Abel JS, Berg C, Geipel A, Gembruch U, Herberg U, Breuer J, Brockmeier K, Gottschalk I. Prenatal diagnosis, associated findings and postnatal outcome of fetuses with truncus arteriosus communis (TAC). Archives of gynecology and obstetrics. 2021 Dec:304(6):1455-1466. doi: 10.1007/s00404-021-06067-x. Epub 2021 May 24 [PubMed PMID: 34028563]
Kumar P, Bhatia M. Role of CT in the Pre- and Postoperative Assessment of Conotruncal Anomalies. Radiology. Cardiothoracic imaging. 2022 Jun:4(3):e210089. doi: 10.1148/ryct.210089. Epub 2022 Jun 30 [PubMed PMID: 35923747]
Lee T, Tsai IC, Fu YC, Jan SL, Wang CC, Chang Y, Chen MC. Using multidetector-row CT in neonates with complex congenital heart disease to replace diagnostic cardiac catheterization for anatomical investigation: initial experiences in technical and clinical feasibility. Pediatric radiology. 2006 Dec:36(12):1273-82 [PubMed PMID: 17036235]
Level 2 (mid-level) evidenceRicci Z, Haiberger R, Pezzella C, Garisto C, Favia I, Cogo P. Furosemide versus ethacrynic acid in pediatric patients undergoing cardiac surgery: a randomized controlled trial. Critical care (London, England). 2015 Jan 7:19(1):2. doi: 10.1186/s13054-014-0724-5. Epub 2015 Jan 7 [PubMed PMID: 25563826]
Level 1 (high-level) evidenceNaimo PS, Fricke TA, Yong MS, d'Udekem Y, Kelly A, Radford DJ, Bullock A, Weintraub RG, Brizard CP, Konstantinov IE. Outcomes of Truncus Arteriosus Repair in Children: 35 Years of Experience From a Single Institution. Seminars in thoracic and cardiovascular surgery. 2016 Summer:28(2):500-511. doi: 10.1053/j.semtcvs.2015.08.009. Epub [PubMed PMID: 28043468]
Sandrio S, Rüffer A, Purbojo A, Glöckler M, Dittrich S, Cesnjevar R. Common arterial trunk: current implementation of the primary and staged repair strategies. Interactive cardiovascular and thoracic surgery. 2015 Dec:21(6):754-60. doi: 10.1093/icvts/ivv261. Epub 2015 Sep 10 [PubMed PMID: 26362626]
Huff C, Mastropietro CW, Riley C, Byrnes J, Kwiatkowski DM, Ellis M, Schuette J, Justice L. Comprehensive Management Considerations of Select Noncardiac Organ Systems in the Cardiac Intensive Care Unit. World journal for pediatric & congenital heart surgery. 2018 Nov:9(6):685-695. doi: 10.1177/2150135118779072. Epub [PubMed PMID: 30322370]
Gómez O, Soveral I, Bennasar M, Crispi F, Masoller N, Marimon E, Bartrons J, Gratacós E, Martinez JM. Accuracy of Fetal Echocardiography in the Differential Diagnosis between Truncus Arteriosus and Pulmonary Atresia with Ventricular Septal Defect. Fetal diagnosis and therapy. 2016:39(2):90-9. doi: 10.1159/000433430. Epub 2015 Jun 25 [PubMed PMID: 26113195]
Gotsch F, Romero R, Espinoza J, Kusanovic JP, Erez O, Hassan S, Yeo L. Prenatal diagnosis of truncus arteriosus using multiplanar display in 4D ultrasonography. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2010 Apr:23(4):297-307. doi: 10.3109/14767050903108206. Epub [PubMed PMID: 19900032]
Traisrisilp K, Tongprasert F, Srisupundit K, Luewan S, Sukpan K, Tongsong T. Prenatal differentiation between truncus arteriosus (Types II and III) and pulmonary atresia with ventricular septal defect. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2015 Nov:46(5):564-70. doi: 10.1002/uog.14788. Epub [PubMed PMID: 25594532]
Shibbani K, Thattaliyath B, Bunker M, Anwar S, Ashwath R. Double-Outlet Right Ventricle, Pulmonary Atresia, and Discontinuous Branch Pulmonary Arteries Supplied by Bilateral Ducti. JACC. Case reports. 2021 Aug 4:3(9):1236-1240. doi: 10.1016/j.jaccas.2021.04.020. Epub 2021 Jun 23 [PubMed PMID: 34401767]
Level 3 (low-level) evidenceKalavrouziotis G, Purohit M, Ciotti G, Corno AF, Pozzi M. Truncus arteriosus communis: early and midterm results of early primary repair. The Annals of thoracic surgery. 2006 Dec:82(6):2200-6 [PubMed PMID: 17126135]
Asagai S, Inai K, Shinohara T, Tomimatsu H, Ishii T, Sugiyama H, Park IS, Nagashima M, Nakanishi T. Long-term Outcomes after Truncus Arteriosus Repair: A Single-center Experience for More than 40 Years. Congenital heart disease. 2016 Dec:11(6):672-677. doi: 10.1111/chd.12359. Epub 2016 Apr 29 [PubMed PMID: 27126954]
Alfieris GM, Swartz MF. The Initial Glimpse at Long-term Outcomes Following the Repair of Truncus Arteriosus. Seminars in thoracic and cardiovascular surgery. 2016 Summer:28(2):512-513. doi: 10.1053/j.semtcvs.2016.08.001. Epub 2016 Aug 11 [PubMed PMID: 28043469]
Graziani F, Delogu AB. Evaluation of Adults With Congenital Heart Disease. World journal for pediatric & congenital heart surgery. 2016 Mar:7(2):185-91. doi: 10.1177/2150135115623285. Epub [PubMed PMID: 26957402]
Tay H, Naimo PS, Huang L, Fricke TA, Brink J, d'Udekem Y, Brizard CP, Konstantinov IE. Long-term quality of life in adults following truncus arteriosus repair. Interactive cardiovascular and thoracic surgery. 2019 Dec 1:29(6):950-954. doi: 10.1093/icvts/ivz198. Epub [PubMed PMID: 31587054]
Level 2 (mid-level) evidenceMoons P, Luyckx K, Thomet C, Budts W, Enomoto J, Sluman MA, Lu CW, Jackson JL, Khairy P, Cook SC, Chidambarathanu S, Alday L, Eriksen K, Dellborg M, Berghammer M, Johansson B, Mackie AS, Menahem S, Caruana M, Veldtman G, Soufi A, Fernandes SM, White K, Callus E, Kutty S, Ombelet F, Apers S, Kovacs AH, APPROACH-IS Consortium and the International Society for Adult Congenital Heart Disease (ISACHD). Physical Functioning, Mental Health, and Quality of Life in Different Congenital Heart Defects: Comparative Analysis in 3538 Patients From 15 Countries. The Canadian journal of cardiology. 2021 Feb:37(2):215-223. doi: 10.1016/j.cjca.2020.03.044. Epub 2020 Apr 6 [PubMed PMID: 32739453]
Level 2 (mid-level) evidenceKovacs AH, Brouillette J, Ibeziako P, Jackson JL, Kasparian NA, Kim YY, Livecchi T, Sillman C, Kochilas LK, American Heart Association Council on Lifelong Congenital Heart Disease and Heart Health in the Young; and Stroke Council. Psychological Outcomes and Interventions for Individuals With Congenital Heart Disease: A Scientific Statement From the American Heart Association. Circulation. Cardiovascular quality and outcomes. 2022 Aug:15(8):e000110. doi: 10.1161/HCQ.0000000000000110. Epub 2022 Jul 14 [PubMed PMID: 35862009]
Level 2 (mid-level) evidenceDavey B, Sinha R, Lee JH, Gauthier M, Flores G. Social determinants of health and outcomes for children and adults with congenital heart disease: a systematic review. Pediatric research. 2021 Jan:89(2):275-294. doi: 10.1038/s41390-020-01196-6. Epub 2020 Oct 17 [PubMed PMID: 33069160]
Level 1 (high-level) evidenceMcElhinney DB, Driscoll DA, Emanuel BS, Goldmuntz E. Chromosome 22q11 deletion in patients with truncus arteriosus. Pediatric cardiology. 2003 Nov-Dec:24(6):569-73 [PubMed PMID: 12947506]
Balachandran R, Nair SG, Kumar RK. Establishing a pediatric cardiac intensive care unit - Special considerations in a limited resources environment. Annals of pediatric cardiology. 2010 Jan:3(1):40-9. doi: 10.4103/0974-2069.64374. Epub [PubMed PMID: 20814475]
Williams JM, de Leeuw M, Black MD, Freedom RM, Williams WG, McCrindle BW. Factors associated with outcomes of persistent truncus arteriosus. Journal of the American College of Cardiology. 1999 Aug:34(2):545-53 [PubMed PMID: 10440171]
Lantin-Hermoso MR, Berger S, Bhatt AB, Richerson JE, Morrow R, Freed MD, Beekman RH 3rd, SECTION ON CARDIOLOGY, CARDIAC SURGERY. The Care of Children With Congenital Heart Disease in Their Primary Medical Home. Pediatrics. 2017 Nov:140(5):. pii: e20172607. doi: 10.1542/peds.2017-2607. Epub [PubMed PMID: 29084831]
Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, Colman JM, Crumb SR, Dearani JA, Fuller S, Gurvitz M, Khairy P, Landzberg MJ, Saidi A, Valente AM, Van Hare GF. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2019 Apr 2:73(12):1494-1563. doi: 10.1016/j.jacc.2018.08.1028. Epub 2018 Aug 16 [PubMed PMID: 30121240]
Level 1 (high-level) evidence