
Introduction
Transfusion reactions are defined as adverse events associated with the transfusion of whole blood or one of its components. These may range in severity from minor to life-threatening. Reactions can occur during the transfusion (acute transfusion reactions) or days to weeks later (delayed transfusion reactions) and may be immunologic or non-immunologic. A reaction may be difficult to diagnose as it can present with non-specific, often overlapping symptoms. The most common signs and symptoms include fever, chills, urticaria (hives), and itching. Some symptoms resolve with little or no treatment. However, respiratory distress, high fever, hypotension (low blood pressure), and red urine (hemoglobinuria) can indicate a more serious reaction.
Types of transfusion reactions include the following: acute hemolytic, delayed hemolytic, febrile non-hemolytic, anaphylactic, simple allergic, septic (bacterial contamination), transfusion-related acute lung injury (TRALI), and transfusion-associated circulatory overload (TACO). All suspected reactions should result in immediately stopping the transfusion and notifying the blood bank and treating clinician.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Immune-mediated transfusion reactions typically occur due to mismatch or incompatibility of the transfused product and the recipient. They include naturally occurring antibodies in the blood recipient (such as anti-A, anti-B which are typically responsible for acute hemolytic transfusion reactions) as well as antibodies made in response to foreign antigens (alloantibodies). These alloantibodies account for many reactions including mild allergic, febrile non-hemolytic, acute hemolytic and anaphylactic. Antibodies present in the blood donor can also cause reactions and are thought to be involved in transfusion-associated lung injury (TRALI).[4][5][6]
Non-immunologic reactions are usually caused by the physical effects of blood components or the transmission of disease. Bacterial contamination, for example, results in septic transfusion reactions and is caused by bacterial and/or endotoxin contamination of a blood product. This may happen at the time of collection due to inadequate blood donor arm disinfection, the presence of bacteria in the donor’s circulation at the time of collection, or due to improper product handling after collection.
Transfusion reactions can also occur unrelated to factors intrinsic to the blood. Examples of these include transfusion-associated volume overload (TACO) and hypothermia.
Epidemiology
Transfusion reactions range in frequency from relatively common, (mild allergic and febrile non-hemolytic reactions) to rare (anaphylaxis, acute hemolytic, and sepsis). Fatal adverse events have been reported to occur most commonly with TRALI, and long-term or later adverse events are typically the result of disease transmission.
The severity and incidence vary depending on the type of transfusion reaction, the prevalence of disease in the donor population, and the extent of follow-up care the patient receives. Due to advances in donor screening, improved testing, and automated data systems, the risks and fatalities associated with the transfusion of blood products continue to decrease.[7][8]
Pathophysiology
The pathophysiology varies based on the transfusion reaction.[9][10][11]
Acute Transfusion Reactions
- Mild allergic: Attributed to hypersensitivity to a foreign protein in the donor product.
- Anaphylactic: Similar to a mild allergic reaction, however resulting in a more severe reaction. Sometimes this can occur in a patient with IgA deficiency who makes alloantibodies against IgA and then receives blood products containing IgA.
- Febrile non-hemolytic: Generally thought to be caused by cytokines released from blood donor leukocytes (white blood cells).
- Septic: Caused by bacteria or bacterial byproducts (such as endotoxin) which may contaminate blood.
- Acute hemolytic transfusion reactions: Can result in intravascular or extravascular hemolysis, depending on the specific etiology (cause). Immune-mediated reactions are often a result of recipient antibodies present to blood donor antigens. Non-immune reactions are possible, and occur when red blood cells are damaged before transfusion (e.g., by heat or incorrect osmotic conditions).
- Transfusion-associated circulatory overload (TACO): Occurs when the volume of the transfused component causes hypervolemia (volume overload).
- Transfusion-related acute lung injury: Acute lung injury is due to antibodies in the donor product (human leukocyte antigen or human neutrophil antigen) reacting with antigens in the recipient. The recipient’s immune system responds and causes the release of mediators that lead to pulmonary edema. Possibly contributing to this are clinical conditions that predispose the patient including infection, recent surgery, or inflammation.
Delayed Transfusion Reactions
- Delayed hemolytic transfusion reaction: Typically caused by an anamnestic response to a foreign antigen that the patient was previously exposed to (generally by prior transfusion or pregnancy).
- Transfusion-associated graft-versus-host disease: Results from engraftment of donor lymphocytes (commonly found in cellular blood products) into an immunocompromised recipient’s bone marrow. The donor lymphocytes recognize the patient as foreign and react against the recipient’s body. The patient’s immune system is unable to clear the foreign lymphocytes. This is rare but often fatal.
History and Physical
A thorough understanding of the patient’s medical history and state of health is needed before the transfusion is started. Vital signs are monitored and typically recorded at 15-minute intervals. A small amount of change in vital signs during transfusion may be considered “normal.” These changes may include the following: plus or minus 0.5 C in temperature, plus or minus 5 respirations per minute, plus or minus 10 beats per minute in heart rate, and plus or minus 20 mm Hg in blood pressure. It is important to note that changes greater than these parameters do not mean that there is a transfusion reaction, it suggests that the bedside nurse should be extra vigilant in monitoring for a reaction. Abnormal responses include hives, itching, fever greater than 1 C above the temperature at the start of transfusion, chills, hypotension, and dyspnea.
Evaluation
Diagnosis of acute transfusion reactions begins by recognition of the signs and symptoms by the bedside. Common signs and symptoms and differential diagnosis are listed below.[12][13][14]
- Urticaria/Itching
Urticaria (hives) and/or itching can be the presenting sign of a mild allergic reaction, but can also be associated with the onset of a life-threatening anaphylactic reaction. The transfusion should be stopped, and the patient should be carefully monitored for progression of symptoms.
- Fever/Chills
Fever and/or chills are most commonly associated with a febrile, non-hemolytic reaction, however; they can also be the first sign of a more serious acute hemolytic reaction, TRALI, or septic transfusion reaction. If the temperature rises 1 C or higher from the temperature at the start of transfusion, the transfusion should be stopped. Acute hemolytic reaction or bacterial contamination should be suspected if there is a greater rise in temperature, or more serious symptoms (e.g., rigors).
- Respiratory Distress/Dyspnea
Dyspnea, or shortness of breath, is a concerning sign that can often be seen with more severe reactions including anaphylaxis, TRALI, and TACO. It can also be seen by itself without accompanying symptoms.
- Hypotension
Hypotension can be seen with an acute hemolytic reaction, septic transfusion reactions, anaphylaxis, and TRALI. They have also been reported without the presence of any other associated transfusion reaction.
- Hypothermia
Hypothermia can be seen with large volume transfusions of refrigerated products. The only intervention needed is warming the patient and/or blood product.
Treatment / Management
When a transfusion reaction is suspected, the transfusion should be immediately stopped, and the intravenous line should be kept open using appropriate fluids (usually 0.9% saline). A clerical check should be performed by examining the product bag and confirming the patient’s identification. The patient’s vital signs should be monitored and recorded at 15-minute intervals. A post-transfusion blood sample should be drawn and sent to the lab, in addition to sending the bag and tubing if possible. The blood bank generally completes additional testing and clerical checks to rule out an incompatible transfusion.
Treatment of specific transfusion reactions is most often supportive. For example, antihistamines (such as diphenhydramine) can be given for a mild allergic reaction, or an antipyretic can be given for a non-hemolytic febrile transfusion reaction.[9][15](B3)
Differential Diagnosis
- Anaphylaxis
- Disseminated intravascular coagulation
- Hemolytic anemia
- Septic shock
Complications
- Disseminated intravascular coagulation
- Lung injury
- Renal failure
- Hemolysis
- Death
Pearls and Other Issues
Transfusion reactions are influenced by many factors including the type of component being transfused, the storage requirements, and the patient’s co-morbid conditions at the time of transfusion. Understanding how to quickly identify transfusion reactions and appropriately manage and treat the patient ensures optimal patient care.
Enhancing Healthcare Team Outcomes
Blood transfusions are often necessary in medicine, and all healthcare workers have to be familiar with transfusion reactions. Patient on any ward can receive a blood transfusion and similarly all nurses have to know the potential complications and how to manage them. The majority of blood transfusion reactions occur because of a clerical/nursing error. While some reactions can be severe and lead to death, many transfusion reactions are benign. Anaphylactic reactions from a blood transfusion are very rare but often result in a fatality. Other reactions include TRALI which ranges from 1-9% and often requires intensive pulmonary support to prevent a fatal outcome. The incidence of bacterial contamination is rare but can occur from both gram-negative and gram-positive organisms. The key to reducing the morbidity is vigilance on the part of the nurse. During the patient medical history, one should ask about prior transfusions and any complications. If there is ever any doubt about the patient's blood group or the blood type being administered, the laboratory should be asked to reconfirm the status.[16][17] (Level V)
Media
(Click Image to Enlarge)
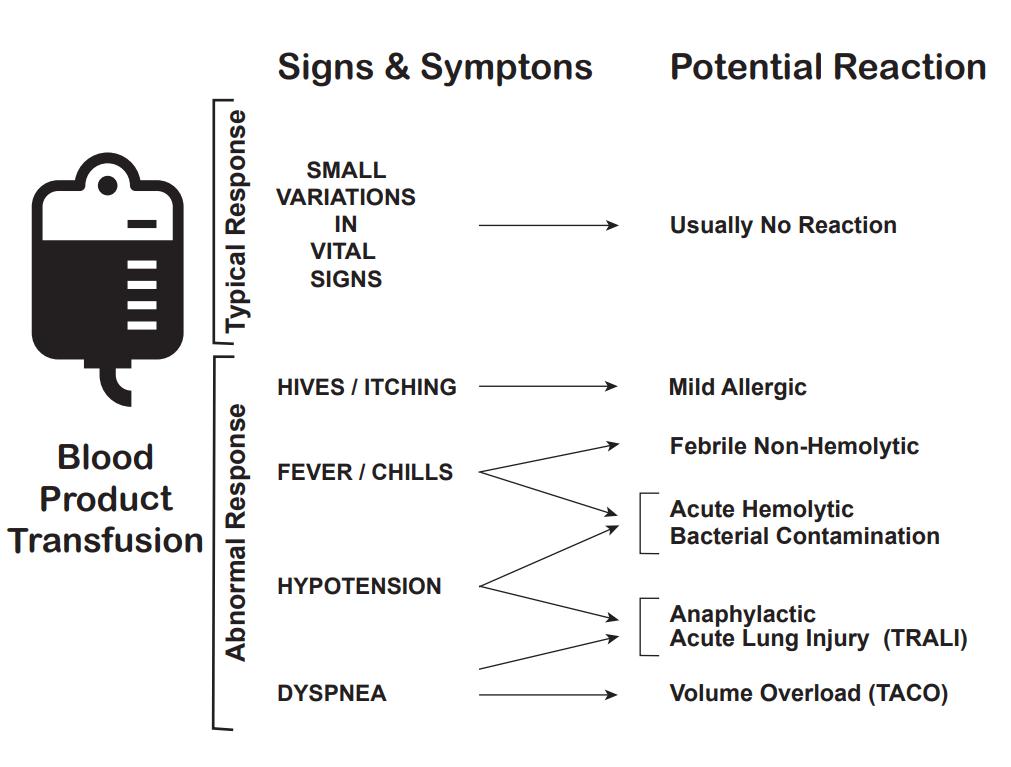
Transfusion Reaction Signs and Symptoms Kendall Crookston MD PhD Professor, Pathology and Medicine University of New Mexico School of Medicine
(Click Image to Enlarge)
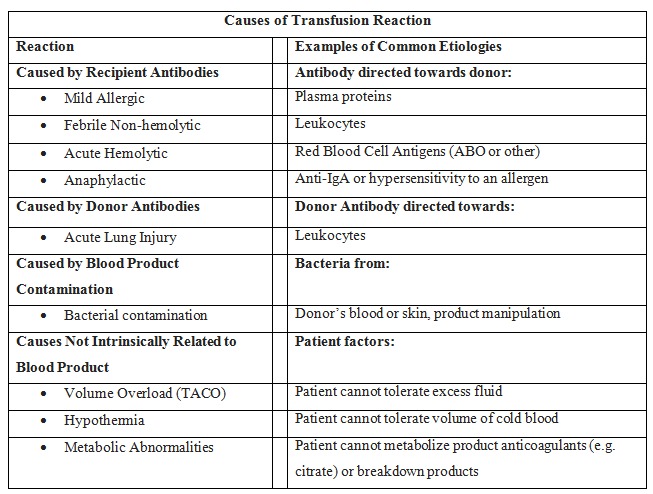
Transfusion Reaction Causes
Contributed by Jolee Suddock, DO, University of New Mexico
References
Sirianni G, Perri G, Callum J, Gardner S, Berall A, Selby D. A Retrospective Chart Review of Transfusion Practices in the Palliative Care Unit Setting. The American journal of hospice & palliative care. 2019 Mar:36(3):185-190. doi: 10.1177/1049909118806456. Epub 2018 Oct 18 [PubMed PMID: 30336680]
Level 2 (mid-level) evidenceMcClosky ME, Cimino Brown D, Weinstein NM, Chappini N, Taney MT, Marryott K, Callan MB. Prevalence of naturally occurring non-AB blood type incompatibilities in cats and influence of crossmatch on transfusion outcomes. Journal of veterinary internal medicine. 2018 Nov:32(6):1934-1942. doi: 10.1111/jvim.15334. Epub 2018 Oct 11 [PubMed PMID: 30307648]
Land KJ, Townsend M, Goldman M, Whitaker BI, Perez GE, Wiersum-Osselton JC. International validation of harmonized definitions for complications of blood donations. Transfusion. 2018 Nov:58(11):2589-2595. doi: 10.1111/trf.14948. Epub 2018 Oct 8 [PubMed PMID: 30294786]
Level 1 (high-level) evidenceAubron C, Aries P, Le Niger C, Sparrow RL, Ozier Y. How clinicians can minimize transfusion-related adverse events? Transfusion clinique et biologique : journal de la Societe francaise de transfusion sanguine. 2018 Nov:25(4):257-261. doi: 10.1016/j.tracli.2018.08.158. Epub 2018 Aug 25 [PubMed PMID: 30197000]
Jasinski S, Glasser CL. Catastrophic Delayed Hemolytic Transfusion Reaction in a Patient With Sickle Cell Disease Without Alloantibodies: Case Report and Review of Literature. Journal of pediatric hematology/oncology. 2019 Nov:41(8):624-626. doi: 10.1097/MPH.0000000000001307. Epub [PubMed PMID: 30179992]
Level 3 (low-level) evidenceErony SM, Marshall CE, Gehrie EA, Boyd JS, Ness PM, Tobian AAR, Carroll KC, Blagg L, Shifflett L, Bloch EM. The epidemiology of bacterial culture-positive and septic transfusion reactions at a large tertiary academic center: 2009 to 2016. Transfusion. 2018 Aug:58(8):1933-1939. doi: 10.1111/trf.14789. Epub 2018 Aug 28 [PubMed PMID: 30153333]
Py JY, Cabezon B, Sapey T, Jutant T. Unacknowledged adverse transfusion reactions: Are they a mine to dig? Transfusion clinique et biologique : journal de la Societe francaise de transfusion sanguine. 2018 Feb:25(1):63-72. doi: 10.1016/j.tracli.2017.06.016. Epub 2017 Jul 6 [PubMed PMID: 28690037]
Jacquot C, Delaney M. Efforts Toward Elimination of Infectious Agents in Blood Products. Journal of intensive care medicine. 2018 Oct:33(10):543-550. doi: 10.1177/0885066618756589. Epub 2018 Mar 21 [PubMed PMID: 29562814]
Siddon AJ, Kenney BC, Hendrickson JE, Tormey CA. Delayed haemolytic and serologic transfusion reactions: pathophysiology, treatment and prevention. Current opinion in hematology. 2018 Nov:25(6):459-467. doi: 10.1097/MOH.0000000000000462. Epub [PubMed PMID: 30124474]
Level 3 (low-level) evidenceTariket S, Sut C, Hamzeh-Cognasse H, Laradi S, Garraud O, Cognasse F. Platelet and TRALI: From blood component to organism. Transfusion clinique et biologique : journal de la Societe francaise de transfusion sanguine. 2018 Sep:25(3):204-209. doi: 10.1016/j.tracli.2018.03.006. Epub 2018 Apr 7 [PubMed PMID: 29631963]
Scher CS. Trauma and transfusion in the geriatric patient. Current opinion in anaesthesiology. 2018 Apr:31(2):238-242. doi: 10.1097/ACO.0000000000000556. Epub [PubMed PMID: 29389749]
Level 3 (low-level) evidenceGarraud O, Cognasse F, Laradi S, Hamzeh-Cognasse H, Peyrard T, Tissot JD, Fontana S. How to mitigate the risk of inducing transfusion-associated adverse reactions. Transfusion clinique et biologique : journal de la Societe francaise de transfusion sanguine. 2018 Nov:25(4):262-268. doi: 10.1016/j.tracli.2018.07.006. Epub 2018 Jul 27 [PubMed PMID: 30139570]
Fasano RM, Meyer EK, Branscomb J, White MS, Gibson RW, Eckman JR. Impact of Red Blood Cell Antigen Matching on Alloimmunization and Transfusion Complications in Patients with Sickle Cell Disease: A Systematic Review. Transfusion medicine reviews. 2019 Jan:33(1):12-23. doi: 10.1016/j.tmrv.2018.07.003. Epub 2018 Jul 26 [PubMed PMID: 30122266]
Level 1 (high-level) evidenceStrasser E. [The new hemotherapy guideline]. Der Unfallchirurg. 2018 May:121(5):423-428. doi: 10.1007/s00113-018-0489-4. Epub [PubMed PMID: 29654513]
Long B, Koyfman A. Emergency Medicine Evaluation and Management of Anemia. Emergency medicine clinics of North America. 2018 Aug:36(3):609-630. doi: 10.1016/j.emc.2018.04.009. Epub 2018 Jun 12 [PubMed PMID: 30037447]
Carman M, Uhlenbrock JS, McClintock SM. CE: A Review of Current Practice in Transfusion Therapy. The American journal of nursing. 2018 May:118(5):36-44. doi: 10.1097/01.NAJ.0000532808.81713.fc. Epub [PubMed PMID: 29664740]
DeLisle J. Is This a Blood Transfusion Reaction? Don't Hesitate; Check It Out. Journal of infusion nursing : the official publication of the Infusion Nurses Society. 2018 Jan/Feb:41(1):43-51. doi: 10.1097/NAN.0000000000000261. Epub [PubMed PMID: 29293197]