Introduction
The thoracodorsal nerve is also referred to as the middle or long subscapular nerve. It arises from the C6 to C8 roots of the brachial plexus. The thoracodorsal nerve exits the posterior cord at the apex of the axilla. It runs posteriorly to the axillary vein in its descent through the axilla and joins the vascular pedicle of the latissimus dorsi muscle. Identification of the thoracodorsal nerve is crucial during surgical procedures of the axilla. Surgeons use the thoracodorsal nerve as a nerve graft in various surgeries. Its primary function is motor innervation of the latissimus dorsi muscle.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The thoracodorsal nerve arises from the C6, C7, and C8 roots but its predominant root is C7.[1] It appears as a branch of the posterior cord of the brachial plexus.
The thoracodorsal nerve courses inferiorly and laterally to form the latissimus dorsi pedicle. In the pedicle, the thoracodorsal nerve is superficial to the thoracodorsal artery and vein.[2] The nerve enters the latissimus dorsi muscle on its tendinous medial surface. The bundle is present on the deep surface of the latissimus dorsi muscle and traces to its lower border.
The thoracodorsal nerve may be identified as posterior and lateral to the lateral thoracic vein, two centimeters from the confluence of the lateral thoracic vein and the axillary vein.[2][3][4] The lateral thoracic vein is lateral to the lateral border of the pectoralis muscle. It is also described to follow the course of the subscapular artery.
Embryology
Muscle development and motoneuron development take place simultaneously. Transcription factors facilitate communication of developing motoneurons to their muscle groups.[5] Motor neurons of the peripheral nervous system arise from the basal plate of the ventral neural tube. The thoracodorsal nerve arises from the hypaxial motor column of the neural tube. Although the deep back muscles arise from epaxial myotomes and hypaxial myotomes are associated with limb muscles and the ventral body wall, the latissimus dorsi muscle is hypaxial in origin. It migrates to the dorsum during development and is a superficial back muscle.
Blood Supply and Lymphatics
The thoracodorsal nerve runs with the thoracodorsal artery and vein to supply the latissimus dorsi muscle. The nerve is close to the lymphatic vessels of the axilla, which are relevant during axillary lymph node dissection procedures. The subscapular lymph nodes are located in the posterior axillary fold, receiving lymph from the posterior thoracic wall and scapular region. Injury to the thoracodorsal nerve during axillary lymph node dissection is less frequent than other complications, including lymphedema and seroma formation.[6]
Muscles
The thoracodorsal nerve is a pure motor nerve that innervates the latissimus dorsi muscle. The latissimus dorsi muscle is a large, fan-shaped muscle that originates from the spinous processes of T7 to L5, the thoracolumbar fascia, and iliac crest. It inserts in the intertubercular groove of the humerus bone and acts to extend, internally rotate, and adduct the arm. The primary blood supply of the latissimus dorsi muscle is the thoracodorsal artery. The dorsal divisions of T6 to T12 provide the sensory innervation of the skin of the latissimus dorsi muscle.
In about 13% of the population, thoracodorsal nerve innervates the teres major muscle.
Physiologic Variants
There are three subtypes of thoracodorsal nerve origin concerning the superior, middle, and inferior trunks of the brachial plexus.[1][7] The superior and middle trunks form Type A, with Type B formed by the middle and inferior trunks and Type C, where the thoracodorsal nerve arises from all three trunks. Branching of the thoracodorsal nerve sometimes occurs proximal to the hilum of the latissimus dorsi muscle.[8]
The thoracodorsal nerve commonly innervates the axillary arch, also known as Langer's arch.[9] This muscular variant of the latissimus dorsi muscle is a musculocutaneous arch that extends between the latissimus dorsi muscle at its humeral insertion point and the pectoralis minor tendon. Its location poses complications during surgical procedures of the axillary region. If present, the axillary arch can complicate axillary lymph node dissection, and the presence of the arch may contribute to lymphedema or entrapment syndromes if not divided.[10]
Surgical Considerations
The thoracodorsal nerve is significant for its use in a variety of nerve reconstruction procedures, as well as its innervation of the latissimus dorsi muscle that
When considering the harvesting of C7, the upper and lower trunks of the brachial plexus have less propensity to contribute to the thoracodorsal nerve and may be safest to use to avoid injury to the thoracodorsal nerve.[1]
The lateral branch of the thoracodorsal nerve is used in nerve graft reconstruction surgery for injuries to the facial, musculocutaneous, accessory, and axillary nerves. The thoracodorsal nerve is also used in surgeries to reinnervate the triceps muscle and restore elbow flexion.[11][12]
In breast reconstructive surgery the latissimus dorsi muscle may be used as a flap to cover an implant or create breast volume. Complications of latissimus dorsi musculocutaneous flap techniques for breast reconstruction include weakening of the shoulder, scarring, and undesired movement of the reconstructed breast. There is no solid consensus regarding the decision to transect or preserve the thoracodorsal nerve or leave it intact.[13][8] Thoracodorsal nerve preservation may cause muscle contraction with potential implant dislocation. A similar degree of atrophy of the latissimus dorsi muscle occurs in patients where there is the preservation of the thoracodorsal nerve. Delayed resection of the thoracodorsal nerve may be more difficult due to fibrosis and impaired access to the latissimus dorsi muscle due to its anterior transposition over the axilla. A complete section of the latissimus dorsi muscle does not guarantee successful denervation. Nonsurgical intervention with botulinum toxin injections has been found to reduce postoperative pain significantly.[14] In comparing the incidence of postoperative latissimus dorsi contraction in a proximal or distal denervation group, the contraction was significantly lower in the proximal group.[15]
The latissimus dorsi flap may also be useful in neophalloplasty procedures in surgeries for gender affirmation and repair of congenital abnormalities and penile trauma.[16][17] The thoracodorsal nerve is joined to the ilioinguinal or obturator nerve using microneurrhaphy techniques.[17][18][17]
Clinical Significance
The latissimus dorsi is among the most frequently used flaps in reconstructive surgery. Despite its popularity, there is less consideration of its consequences on donor muscle function.[19] Consequences of flap harvesting include weakness arising from chair, weakness of arm adduction, and shoulder weakness.
Injuries to the latissimus dorsi muscle tendon may disrupt the contour of the posterior axillary fold.[20] There have been reports of baseball pitchers injuring the latissimus dorsi muscle tendon and muscle belly.[21] The latissimus dorsi muscle may be damaged during anterior spinal surgery using the transthoracic approach.[22]
Other Issues
The axillary arch is a myofascial slip that derives from the latissimus dorsi muscle, involving the axilla and the shoulder. In about 40% of the population, the axillary arch receives innervation from the thoracodorsal nerve. The fascia can create several clinical problems; axillary arch dysfunction could cause nerve traction and be one of the causes of thoracic outlet syndrome.
Media
(Click Image to Enlarge)
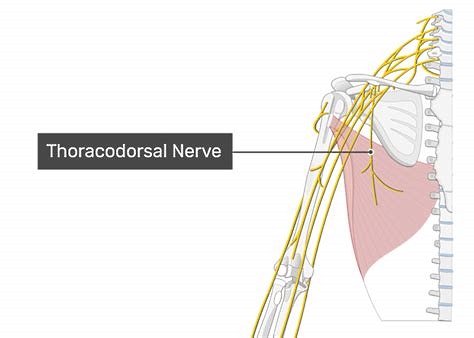
The Thoracodorsal Nerve. The figure shows the thoracodorsal nerve and the latissimus dorsi muscle.
Contributed by B Bordoni, PhD
References
Lu W, Xu JG, Wang DP, Gu YD. Microanatomical study on the functional origin and direction of the thoracodorsal nerve from the trunks of brachial plexus. Clinical anatomy (New York, N.Y.). 2008 Sep:21(6):509-13. doi: 10.1002/ca.20656. Epub [PubMed PMID: 18698655]
Takahashi N, Watanabe K, Koga N, Rikimaru H, Kiyokawa K, Saga T, Nakamura M, Tabira Y, Yamaki K. Anatomical Research of the Three-dimensional Route of the Thoracodorsal Nerve, Artery, and Veins in Latissimus Dorsi Muscle. Plastic and reconstructive surgery. Global open. 2013 May:1(2):1-7. doi: 10.1097/GOX.0b013e3182948534. Epub 2013 Jun 7 [PubMed PMID: 25289214]
Zin T, Maw M, Oo S, Pai D, Paijan R, Kyi M. How I do it: Simple and effortless approach to identify thoracodorsal nerve on axillary clearance procedure. Ecancermedicalscience. 2012:6():255. doi: 10.3332/ecancer.2012.255. Epub 2012 May 28 [PubMed PMID: 22675404]
Anthony DJ, Basnayake BMOD, Ganga NMG, Mathangasinghe Y, Malalasekera AP. An improved technical trick for identification of the thoracodorsal nerve during axillary clearance surgery: a cadaveric dissection study. Patient safety in surgery. 2018:12():18. doi: 10.1186/s13037-018-0164-2. Epub 2018 Jun 26 [PubMed PMID: 29983745]
Musumeci G, Castrogiovanni P, Coleman R, Szychlinska MA, Salvatorelli L, Parenti R, Magro G, Imbesi R. Somitogenesis: From somite to skeletal muscle. Acta histochemica. 2015 May-Jun:117(4-5):313-28. doi: 10.1016/j.acthis.2015.02.011. Epub 2015 Apr 4 [PubMed PMID: 25850375]
Tsangaris TN, Trad K, Brody FJ, Jacobs LK, Tsangaris NT, Sackier JM. Endoscopic axillary exploration and sentinel lymphadenectomy. Surgical endoscopy. 1999 Jan:13(1):43-7 [PubMed PMID: 9869687]
Lee KS. Variation of the spinal nerve compositions of thoracodorsal nerve. Clinical anatomy (New York, N.Y.). 2007 Aug:20(6):660-2 [PubMed PMID: 17352401]
Paolini G, Longo B, Laporta R, Sorotos M, Amoroso M, Santanelli F. Permanent latissimus dorsi muscle denervation in breast reconstruction. Annals of plastic surgery. 2013 Dec:71(6):639-42. doi: 10.1097/SAP.0b013e31825c0840. Epub [PubMed PMID: 23403547]
Level 1 (high-level) evidenceAl Maksoud AM, Barsoum AK, Moneer MM. Langer's arch: a rare anomaly affects axillary lymphadenectomy. Journal of surgical case reports. 2015 Dec 27:2015(12):. pii: rjv159. doi: 10.1093/jscr/rjv159. Epub 2015 Dec 27 [PubMed PMID: 26712801]
Level 3 (low-level) evidenceTaterra D, Henry BM, Zarzecki MP, Sanna B, Pękala PA, Cirocchi R, Walocha JA, Tubbs RS, Tomaszewski KA. Prevalence and anatomy of the axillary arch and its implications in surgical practice: A meta-analysis. The surgeon : journal of the Royal Colleges of Surgeons of Edinburgh and Ireland. 2019 Feb:17(1):43-51. doi: 10.1016/j.surge.2018.04.003. Epub 2018 May 22 [PubMed PMID: 29801707]
Level 1 (high-level) evidenceSoldado F, Ghizoni MF, Bertelli J. Thoracodorsal nerve transfer for triceps reinnervation in partial brachial plexus injuries. Microsurgery. 2016 Mar:36(3):191-7. doi: 10.1002/micr.22386. Epub 2015 Jan 29 [PubMed PMID: 25639376]
Level 2 (mid-level) evidenceSoldado F, Ghizoni MF, Bertelli J. Thoracodorsal nerve transfer for elbow flexion reconstruction in infraclavicular brachial plexus injuries. The Journal of hand surgery. 2014 Sep:39(9):1766-70. doi: 10.1016/j.jhsa.2014.04.043. Epub 2014 Jun 13 [PubMed PMID: 24934602]
Szychta P, Butterworth M, Dixon M, Kulkarni D, Stewart K, Raine C. Breast reconstruction with the denervated latissimus dorsi musculocutaneous flap. Breast (Edinburgh, Scotland). 2013 Oct:22(5):667-72. doi: 10.1016/j.breast.2013.01.001. Epub 2013 Jan 30 [PubMed PMID: 23374963]
Level 1 (high-level) evidenceLayeeque R, Hochberg J, Siegel E, Kunkel K, Kepple J, Henry-Tillman RS, Dunlap M, Seibert J, Klimberg VS. Botulinum toxin infiltration for pain control after mastectomy and expander reconstruction. Annals of surgery. 2004 Oct:240(4):608-13; discussion 613-4 [PubMed PMID: 15383788]
Bolla M, Pasteuris C, Pillet G, Vincent P, Loiseau D. [Causes of failure in the curative treatment of cancer of the exocrine pancreas]. Bulletin du cancer. 1990:77(3):299-304 [PubMed PMID: 2340357]
Dennis M, Granger A, Ortiz A, Terrell M, Loukos M, Schober J. The anatomy of the musculocutaneous latissimus dorsi flap for neophalloplasty. Clinical anatomy (New York, N.Y.). 2018 Mar:31(2):152-159. doi: 10.1002/ca.23016. Epub 2017 Dec 28 [PubMed PMID: 29178203]
Perovic SV, Djinovic R, Bumbasirevic M, Djordjevic M, Vukovic P. Total phalloplasty using a musculocutaneous latissimus dorsi flap. BJU international. 2007 Oct:100(4):899-905; discussion 905 [PubMed PMID: 17822468]
Vesely J, Hyza P, Ranno R, Cigna E, Monni N, Stupka I, Justan I, Dvorak Z, Novak P, Ranno S. New technique of total phalloplasty with reinnervated latissimus dorsi myocutaneous free flap in female-to-male transsexuals. Annals of plastic surgery. 2007 May:58(5):544-50 [PubMed PMID: 17452841]
Kwon ST, Chang H, Oh M. Anatomic basis of interfascicular nerve splitting of innervated partial latissimus dorsi muscle flap. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2011 May:64(5):e109-14. doi: 10.1016/j.bjps.2010.12.008. Epub [PubMed PMID: 21300582]
George MS, Khazzam M. Latissimus Dorsi Tendon Rupture. The Journal of the American Academy of Orthopaedic Surgeons. 2019 Feb 15:27(4):113-118. doi: 10.5435/JAAOS-D-17-00581. Epub [PubMed PMID: 30278013]
Donohue BF, Lubitz MG, Kremchek TE. Sports Injuries to the Latissimus Dorsi and Teres Major. The American journal of sports medicine. 2017 Aug:45(10):2428-2435. doi: 10.1177/0363546516676062. Epub 2016 Dec 20 [PubMed PMID: 28125914]
Lazio BE, Staab M, Stambough JL, Hurst JM. Latissimus dorsi rupture: an unusual complication of anterior spine surgery. Journal of spinal disorders. 1993 Feb:6(1):83-6 [PubMed PMID: 8439723]
Level 3 (low-level) evidence