Introduction
The neck contains multiple muscles, classified in part by their relationship to the hyoid bone. Muscles above the hyoid bone are termed "suprahyoid muscles," while those below are called "infrahyoid muscles." Suprahyoid muscles facilitate chewing, swallowing, and phonation. Along with the infrahyoid muscles, suprahyoid muscles stabilize the hyoid, which lacks articulation with other bones. These muscles likewise assist with neck flexion.[1]
The suprahyoid muscles are positioned between 2 bony landmarks, the base of the mandible superiorly and the hyoid bone inferiorly. These muscles are organized into 4 pairs on each side of the midline, as follows (see Image. Suprahyoid Muscles):
Suprahyoid muscles play a crucial role in airway management, as their dysfunction can contribute to obstructive sleep apnea and complications during intubation. Surgically, these neck muscles are important landmarks in procedures such as submandibular gland excision and reconstruction approaches involving the floor of the mouth. Understanding the anatomy and function of suprahyoid muscles aids in diagnosing and treating conditions affecting swallowing, speech, and airway patency.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Most of the suprahyoid muscles are thin and slender, except for the mylohyoid, and they connect the hyoid bone to the base of the mandible and the skull. These muscles suspend the hyoid bone superiorly and contribute to its elevation, along with the floor of the mouth, during deglutition when the mandible remains stable.[6]
The mylohyoid muscle has a square morphology and forms the muscular floor of the mouth. This muscle lies superficially to the digastric muscles and contributes to the Pirogov triangle, which is defined by the posterior edge of the mylohyoid muscle, the intermediate tendon of the digastric muscle, and the hypoglossal nerve. This anatomical space contains the lingual artery.[7]
The digastric muscle derives its name from its 2 muscular bellies, anterior and posterior, which are connected by an intermediate tendon.[8] The posterior belly attaches to the sternocleidomastoid and splenius capitis muscles, both of which affix to the mastoid process. Additionally, this structure is closely related to the internal jugular vein, internal carotid artery, and parotid gland.[9] The posterior belly also contributes to the Beclard triangle, formed by the posterior edge of the hyoglossus muscle, the greater horn of the hyoid bone, and the posterior edge of the posterior belly of the digastric muscle. This triangle contains the hypoglossal nerve and lingual artery. The anterior belly lies adjacent to its contralateral counterpart and is associated with the submandibular gland and the superficial surface of the mylohyoid muscle.[10]
The geniohyoid muscle, a short, triangular structure, is located beneath the genioglossus muscle and positioned above the digastric and mylohyoid muscles.[10] The stylohyoid muscle is thin and elongated, running alongside the posterior belly of the digastric muscle and medially related to the external carotid artery.
When the infrahyoid muscles stabilize the hyoid bone, the suprahyoid muscles contribute to mandibular depression, facilitating a wide opening of the mouth.[11] Suprahyoid muscles also assist in neck flexion. These muscles are arranged in 3 planes: a deep plane containing the geniohyoid muscle, a middle plane consisting of the mylohyoid muscle, and a superficial plane formed by the digastric and stylohyoid muscles. Some sources classify the hyoglossus muscle as a suprahyoid muscle, but most literature considers it an extrinsic tongue muscle since it does not attach to any superior bony structure like the other suprahyoid muscles.[12]
Each muscle within this group has a distinct function. The digastric muscle aids in chin depression and retraction, assisting with mouth opening. This muscle also elevates the hyoid bone and floor of the oral cavity, contributing to swallowing.[13] The mylohyoid muscle elevates the floor of the mouth and tongue, playing a role in deglutition and speech, and assists in mandibular depression when the hyoid bone remains fixed.[14] The stylohyoid muscle elevates and retracts the hyoid bone, raising the tongue and elongating the floor of the mouth. The geniohyoid muscle moves the hyoid bone upward and forward, widening the airway passage.[15] Studies suggest that the geniohyoid muscle generates greater force in advancing the hyoid bone, while the mylohyoid muscle exerts stronger cranial movement of the hyoid bone.
Embryology
Among the 4 suprahyoid muscles, the mylohyoid and the anterior belly of the digastric originate from the mesoderm of the 1st pharyngeal (branchial) arch and receive innervation from the mandibular nerve, the 3rd division of the trigeminal nerve (cranial nerve V3). In contrast, the posterior belly of the digastric and the stylohyoid develop from the mesoderm of the 2nd pharyngeal arch and are innervated by the facial nerve (cranial nerve VII).[16] The geniohyoid muscle, unlike the others, originates from occipital somitic mesoderm.
The suprahyoid muscles begin developing between the 4th and 5th weeks of embryogenesis as the pharyngeal arches form from neural crest-derived mesenchyme, and muscle primordia start differentiating within their respective arches. Between the 6th and 8th weeks, these muscle masses migrate to their final positions near the hyoid bone and mandible while their associated cranial nerves extend projections to establish innervation. By the 9th week and beyond, the muscles become functionally integrated into the oropharyngeal structures.[17]
Blood Supply and Lymphatics
All suprahyoid muscles receive vascular supply from branches of the external carotid artery. The anterior belly of the digastric muscle is supplied by the submental branch of the facial artery, while the posterior belly receives blood from the occipital and posterior auricular arteries. Branches of the lingual artery supply the geniohyoid muscle. The mylohyoid muscle receives blood from the submental branch of the facial artery and the mylohyoid branch of the inferior alveolar artery.[18] Lymph from the suprahyoid region flows into the submental and submandibular lymph nodes before ultimately draining into the deep cervical lymph nodes.
Nerves
The mylohyoid and the anterior belly of the digastric muscle receive innervation from the mylohyoid nerve, a branch of the inferior alveolar nerve, which arises from the mandibular nerve.[19] The facial nerve innervates the stylohyoid and the posterior belly of the digastric muscle.[20] The geniohyoid muscle receives its nerve supply from the first cervical nerve via the hypoglossal nerve.
Muscles
All the suprahyoid muscles are named based on their origin and insertion, except for the digastric muscle. The 1st part of the name indicates the origin, while the 2nd part denotes the insertion. However, the origin and insertion may be interchangeable, depending on whether the hyoid bone is mobile or stabilized by the infrahyoid muscles.
Digastric
The digastric muscle is a spindle-shaped structure with 2 bellies ("di" signifies "two," and "gastric" denotes "belly"), an anterior and a posterior belly, connected by an intermediate tendon. The posterior belly is relatively longer than the anterior belly. The posterior belly originates from the mastoid notch of the temporal bone, while the anterior belly arises from the digastric fossa of the mandible near the symphysis menti.[21] Both bellies slope downward from their origins and meet at the intermediate tendon, which is anchored to the hyoid bone at the junction of its body and greater cornu by a fascial sling of the deep cervical fascia.
Despite forming a single muscle, the 2 bellies receive innervation from different nerves due to their distinct embryological origins. The facial nerve supplies the posterior belly, while the mylohyoid branch of the inferior alveolar nerve, a branch of the mandibular nerve, innervates the anterior belly. The digastric muscle contributes to the formation of 2 anatomical triangles: the submandibular triangle, defined by its 2 bellies, and the submental triangle, bordered by the 2 anterior bellies on either side of the midline.
Stylohyoid
The stylohyoid runs alongside the posterior belly of the digastric muscle, and both share innervation from the facial nerve. This slender muscle originates from the middle of the styloid process of the temporal bone and inserts onto the hyoid bone at the junction of its body and greater horn, superior to the omohyoid. Stylohyoid pulls the hyoid bone backward and upward, which elevates the tongue and elongates the floor of the mouth, aiding in deglutition. The intermediate tendon of the digastric muscle passes through the stylohyoid muscle near its insertion.
Mylohyoid
The mylohyoid is a flat muscle that originates from the inner surface of the mandible along the mylohyoid line. This muscle's broad origin extends from the symphysis menti anteriorly to the region of the last molar tooth posteriorly, giving rise to its name, as "mylo" derives from the Greek word for "molar." The mylohyoid joins its counterpart on the opposite side, inserting at the midline fibrous raphe anteriorly and the body of the hyoid bone posteriorly, sloping downward and medially on each side. Together, these muscles form a supportive gutter for the floor of the mouth and provide structural support for the tongue.[22] For this reason, the mylohyoid is also referred to as the "diaphragma oris" (oral diaphragm).
Geniohyoid
The geniohyoid is a short, slender, ribbon-shaped muscle situated deep to the mylohyoid, representing the most proximal component of the rectus cervicis muscle group. This muscle originates from the inferior genial tubercle of the mandible near the symphysis menti and inserts into the body of the hyoid bone.[23] The 2 geniohyoid muscles lie parallel and close to each other on either side of the midline.[24]
Physiologic Variants
Variations in the stylohyoid muscle include duplication or absence. In some cases, the stylohyoid may insert onto the mylohyoid or omohyoid muscles instead of the hyoid bone. Additionally, the sublingual glands and vessels may occasionally herniate through the mylohyoid muscle.[25]
Accessory heads of the anterior belly of the digastric muscle are relatively common (65.8%) and may be mistaken for a mass on computed tomography or magnetic resonance imaging. In rare cases, the anterior belly may be absent (agenesis).[26] Although variations in the nerve to the mylohyoid are uncommon, they have significant clinical implications in surgical procedures such as dental implant placement in an edentulous mandible, graft harvesting, and posttraumatic screw fixation.[27]
Surgical Considerations
The suprahyoid muscles define key anatomical landmarks in the suprahyoid region of the neck. The submental triangle is situated between the 2 anterior bellies of the digastric muscle, while the submandibular (digastric) triangle lies between the anterior and posterior bellies of the digastric muscle. These anatomical triangles are critical for identifying specific structures, making an understanding of their boundaries and contents essential for surgeons.
The posterior belly of the digastric muscle serves as an important surgical landmark, as 3 cranial nerves, the hypoglossal, accessory, and vagus, pass deep to it, along with 3 major blood vessels, the external and internal carotid arteries and the internal jugular vein.[28] The anterior belly of the digastric muscle plays a significant role in aesthetic surgical procedures, including rhytidectomy, submental lipectomy, suprahyoid muscle repositioning, submental artery flap reconstruction, cervicomental angle modification, and facial muscle restoration following neurological injury.[29][30]
Stylohyoid muscle transfer is a potential surgical option when the digastric muscle is unsuitable for use.[31] This procedure enhances both aesthetic and functional outcomes, particularly following marginal mandibular nerve injury, which can cause lip asymmetry.[32] In cases of total parotidectomy, incorporating a mylohyoid muscle transfer can improve healing and contribute to tissue volume restoration.
Clinical Significance
The stylohyoid ligament is a fibrous structure that may undergo partial ossification, leading to Eagle syndrome (stylohyoid syndrome). This condition affects approximately 4% of the population and typically presents with unilateral sharp, shooting pain in the jaw that radiates to the throat, tongue, or ear. Symptoms often include difficulty swallowing, sore throat, and tinnitus, which may worsen with neck movement. Another contributing factor is an elongated styloid process measuring 3 cm or more.[33]
Eagle syndrome is more frequently observed in individuals with Turner syndrome than in the general population.[34] In the vascular variant of the syndrome, compression of the internal carotid artery may occur. In some cases, compression of the internal jugular vein may also be observed.[35] Surgical resection of the structure causing compression, whether the ossified ligament or the elongated styloid process, is the primary treatment approach.[36] In some animal species, the stylohyoid ligament undergoes complete ossification, forming a distinct epihyal bone.
Other Issues
Researchers have recently observed that the tongue pressure technique not only strengthens the tongue muscles but also significantly enhances the function of the suprahyoid muscles.[37] Exercises such as Chin-Tuck Against Resistance, Shaker exercise, Expiratory Muscle Strength Training, and Neuromuscular Electrical Stimulation have been shown to improve suprahyoid muscle strength, contributing to better laryngeal elevation and enhanced airway protection during swallowing.[38] Osteopathic approaches, including manual therapy, are used to improve the function of the suprahyoid muscles by enhancing tongue mobility and hyoid bone movement. These treatments primarily involve fascial techniques.
Media
(Click Image to Enlarge)
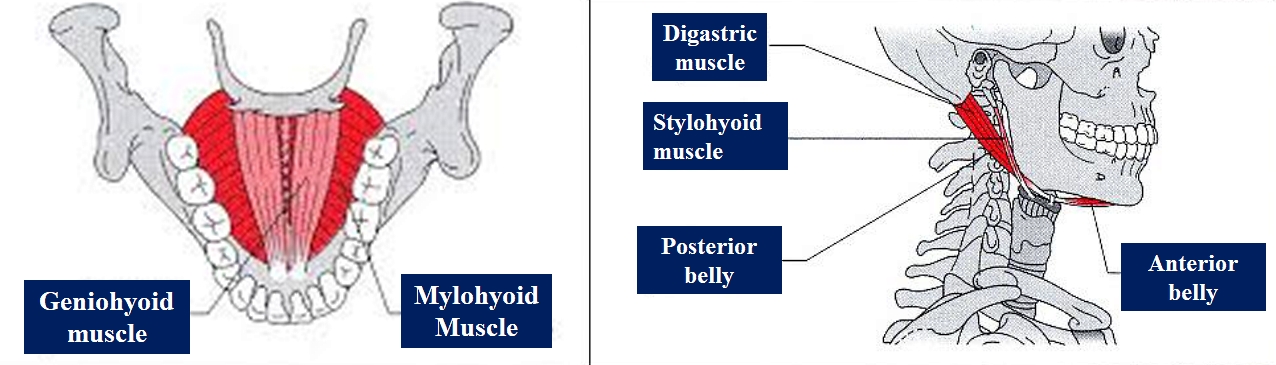
Suprahyoid Muscles. This illustration shows the anatomic relationships between the suprahyoid muscles—the geniohyoid, mylohyoid, digastric (anterior and posterior bellies), and stylohyoid—and nearby head and neck structures.
Contributed by Bruno Bordoni, PhD.
References
Park JS, Hwang NK, Yoon TH, Chang MY. Effects of multi directional chin tuck against resistance exercise on tongue pressure and thickness and suprahyoid muscle activity. Scientific reports. 2024 Dec 3:14(1):30040. doi: 10.1038/s41598-024-81993-9. Epub 2024 Dec 3 [PubMed PMID: 39627405]
Bhat NP, Sumalatha S, Shetty A, Prabhath S. A clinical perspective on the anatomical study of digastric muscle. Anatomy & cell biology. 2023 Dec 31:56(4):441-447. doi: 10.5115/acb.23.043. Epub 2023 Oct 6 [PubMed PMID: 37798015]
Level 3 (low-level) evidenceDepp RM, Irish M, Schag E, Patel D, Olson RA. Bilateral variation of the stylohyoid muscle in a female cadaver. Morphologie : bulletin de l'Association des anatomistes. 2025 Mar:109(364):100925. doi: 10.1016/j.morpho.2024.100925. Epub 2024 Nov 29 [PubMed PMID: 39615186]
Wang Z, Bai J, Cheng K, Zhang X, Fan Z, Chen Y, Ni J. Effects of different mylohyoid muscle stimulations on swallowing cortex excitability in healthy subjects. Behavioural brain research. 2024 Jul 26:470():115055. doi: 10.1016/j.bbr.2024.115055. Epub 2024 May 23 [PubMed PMID: 38795846]
Kawata S, Hiramatsu Y, Honke J, Murakami T, Booka E, Matsumoto T, Morita Y, Kikuchi H, Yamauchi K, Takeuchi H. Preoperative geniohyoid muscle mass in esophageal cancer patients is associated with swallowing function after esophagectomy. Annals of gastroenterological surgery. 2024 Nov:8(6):1026-1035. doi: 10.1002/ags3.12839. Epub 2024 Jun 26 [PubMed PMID: 39502723]
Kelly E, Nazeer S, Fazzini B, Sutt AL, Olusanya S, Campion T, Puthucheary Z. Assessing the oral and suprahyoid muscles in healthy adults using muscle ultrasound to inform the swallowing process: a proof-of-concept study. Scientific reports. 2024 Jun 8:14(1):13198. doi: 10.1038/s41598-024-62032-z. Epub 2024 Jun 8 [PubMed PMID: 38851791]
Domic D, Kappenberger J, Bertl K, Hirtler L, Heimel P, Ulm C. The mylohyoid line is highly variable but does not affect the microarchitecture of the edentulous alveolar bone - an anatomical micro-CT study. BMC oral health. 2024 May 3:24(1):528. doi: 10.1186/s12903-024-04293-8. Epub 2024 May 3 [PubMed PMID: 38702714]
Sagalow ES, Wang R, Babu J, Bigcas JL, Okuyemi O. Incidental Finding of Double Posterior Belly of Digastric Muscle in Head and Neck Cancer Patient. The Annals of otology, rhinology, and laryngology. 2024 Dec:133(12):1033-1036. doi: 10.1177/00034894241284187. Epub 2024 Sep 24 [PubMed PMID: 39318104]
May H, Schwartz C, Dundar Y. How Reliable Is the Posterior Belly of the Digastric Muscle in Preventing Carotid Injury During Neck Dissection? Cureus. 2024 Nov:16(11):e74231. doi: 10.7759/cureus.74231. Epub 2024 Nov 22 [PubMed PMID: 39712745]
Pauloski BR, Yahnke KM. Reliability of Measuring Geniohyoid Cross-Sectional Area with B-Mode Ultrasound. Dysphagia. 2025 Feb:40(1):141-151. doi: 10.1007/s00455-024-10712-3. Epub 2024 May 24 [PubMed PMID: 38789680]
Level 2 (mid-level) evidenceUysal Ö. A Letter to the Editor on "Effect of Visual Biofeedback Obtained Using the Iowa Oral Performance Instrument on the Suprahyoid Muscle Activation Level During Effortful Swallowing Maneuver". Dysphagia. 2024 Dec:39(6):1218-1219. doi: 10.1007/s00455-024-10698-y. Epub 2024 Apr 6 [PubMed PMID: 38581479]
Level 3 (low-level) evidenceNagasaki T, Kurihara-Okawa K, Okawa J, Nihara J, Takahashi K, Hori K, Fukui T, Ono T, Saito I. Tongue pressure and maxillofacial muscle activities during swallowing in patients with mandibular prognathism. Journal of oral rehabilitation. 2024 Aug:51(8):1413-1421. doi: 10.1111/joor.13712. Epub 2024 Apr 25 [PubMed PMID: 38661389]
Oh JC. Effect of Visual Biofeedback Obtained Using the Iowa Oral Performance Instrument on the Suprahyoid Muscle Activation Level During Effortful Swallowing Maneuver. Dysphagia. 2024 Jun:39(3):433-443. doi: 10.1007/s00455-023-10627-5. Epub 2023 Nov 7 [PubMed PMID: 37936019]
Yoshikawa K, Nakamori M, Ushio K, Toko M, Yamada H, Nishikawa Y, Fukuoka T, Maruyama H, Mikami Y. Analysis of the suprahyoid muscles during tongue elevation: High-density surface electromyography as a novel tool for swallowing-related muscle assessment. Journal of oral rehabilitation. 2024 Sep:51(9):1872-1880. doi: 10.1111/joor.13737. Epub 2024 May 12 [PubMed PMID: 38736136]
Mori T, Wakabayashi H, Fujishima I, Narabu R, Shimizu A, Oshima F, Itoda M, Ogawa S, Ohno T, Yamada M, Kunieda K, Shigematsu T, Ogawa N, Nishioka S, Fukuma K, Ishikawa Y, Saito Y, Japanese Working Group on Sarcopenic Dysphagia. Cutoff value of the geniohyoid muscle mass to identify sarcopenic dysphagia by ultrasonography. European geriatric medicine. 2024 Aug:15(4):1031-1037. doi: 10.1007/s41999-024-00971-6. Epub 2024 Apr 8 [PubMed PMID: 38587613]
Kalniev M, Krastev D, Krastev N, Vidinov K, Veltchev L, Apostolov A, Mileva M. A rare variation of the digastric muscle. Clujul medical (1957). 2013:86(4):327-9 [PubMed PMID: 26527971]
Tsyhykalo OV, Kuzniak NB, Perebyjnis PP, Boitsaniuk SI, Tsvyntarna IY, Servatovych AM. PECULIARITIES OF THE MORPHOMETRIC PARAMETERS OF SUPRAHYOID REGION OF THE HUMAN PREFETUSES. Wiadomosci lekarskie (Warsaw, Poland : 1960). 2021:74(2):291-294 [PubMed PMID: 33813489]
Al-Missri MZ, Al Khalili Y. Anatomy, Head and Neck, Submental Triangle. StatPearls. 2025 Jan:(): [PubMed PMID: 31424880]
Chandrasekaran B, John RR, Murugadoss P. Anatomical Variations of Mylohyoid Nerve and Its Clinical Significance: A Cadaveric Study with Review of Literature. Journal of maxillofacial and oral surgery. 2025 Feb:24(1):274-278. doi: 10.1007/s12663-022-01787-2. Epub 2022 Sep 19 [PubMed PMID: 39902408]
Grimmett HJ, Abouzaid KA, Greenberg A, Dar N, Kimbimbi K, Faridi Tavana H, Imam A. A Cadaveric Case Report of Bilateral Accessory Anterior Bellies of the Digastric Muscles. Cureus. 2024 Dec:16(12):e75938. doi: 10.7759/cureus.75938. Epub 2024 Dec 18 [PubMed PMID: 39830572]
Level 3 (low-level) evidenceŠink Ž, Umek N, Cvetko E. Cross-over type of supernumerary digastric muscle. Folia morphologica. 2019:78(3):647-650. doi: 10.5603/FM.a2018.0112. Epub 2018 Dec 11 [PubMed PMID: 30536357]
Level 3 (low-level) evidenceNoguchi T, Morita S, Suzuki R, Matsunaga S, Hirouchi H, Kasahara N, Sugahara K, Abe S. Structural analysis of the mylohyoid muscle as a septum dividing the floor of the oral cavity for the purposes of dental implant surgery: variety of muscle attachment positions and ranges of distribution. International journal of implant dentistry. 2023 Dec 8:9(1):49. doi: 10.1186/s40729-023-00513-y. Epub 2023 Dec 8 [PubMed PMID: 38066306]
Kiyomiya Y, Fujiu-Kurachi M, Hirata A, Nakasone W, Azuma M, Kishida S, Tsuda G. Morphological and functional changes of the geniohyoid muscle in elderly patients after hip fracture surgery: Comparison of ultrasound images with a focus on swallowing function. Journal of oral rehabilitation. 2024 May:51(5):870-878. doi: 10.1111/joor.13650. Epub 2024 Jan 12 [PubMed PMID: 38214198]
Feng X, Todd T, Lintzenich CR, Ding J, Carr JJ, Ge Y, Browne JD, Kritchevsky SB, Butler SG. Aging-related geniohyoid muscle atrophy is related to aspiration status in healthy older adults. The journals of gerontology. Series A, Biological sciences and medical sciences. 2013 Jul:68(7):853-60. doi: 10.1093/gerona/gls225. Epub 2012 Oct 30 [PubMed PMID: 23112114]
Level 2 (mid-level) evidenceOtonari-Yamamoto M, Nakajima K, Tsuji Y, Otonari T, Curtin HD, Okano T, Sano T. Imaging of the mylohyoid muscle: separation of submandibular and sublingual spaces. AJR. American journal of roentgenology. 2010 May:194(5):W431-8. doi: 10.2214/AJR.09.3516. Epub [PubMed PMID: 20410390]
Johns Lalitha J, Riju J, Ramalingam N, Abraham L, Florence Francis G. Navigating the void: outcomes and adaptations during parotid surgery in the absence of posterior belly of digastric muscle. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2024 Oct:281(10):5555-5558. doi: 10.1007/s00405-024-08787-7. Epub 2024 Jul 18 [PubMed PMID: 39025975]
Choi P, Iwanaga J, Dupont G, Oskouian RJ, Tubbs RS. Clinical anatomy of the nerve to the mylohyoid. Anatomy & cell biology. 2019 Mar:52(1):12-16. doi: 10.5115/acb.2019.52.1.12. Epub 2019 Mar 29 [PubMed PMID: 30984446]
Jhawar SS, Nunez M, Pacca P, Voscoboinik DS, Truong H. Craniovertebral junction 360°: A combined microscopic and endoscopic anatomical study. Journal of craniovertebral junction & spine. 2016 Oct-Dec:7(4):204-216 [PubMed PMID: 27891029]
Varelas AN, Bhatt N, Varelas EA, Franco A, Lee JW, Eytan DF. Reanimation of the Lower Lip with the Anterior Belly of Digastric Transfer: A Systematic Review. Facial plastic surgery & aesthetic medicine. 2024 Sep-Oct:26(5):538-543. doi: 10.1089/fpsam.2023.0142. Epub 2024 Feb 13 [PubMed PMID: 38350142]
Level 1 (high-level) evidenceYue Y, Guo X, Lai C, Jin X. Double Chin Concerns after En Bloc Mandibular U-Shaped Osteotomy: Submental-Cervical Soft Tissue Changes and Anterior Belly of Digastric Muscle Assessment. Aesthetic plastic surgery. 2024 Jun:48(11):2025-2033. doi: 10.1007/s00266-024-03955-w. Epub 2024 Mar 27 [PubMed PMID: 38536429]
Kim SM, Patel D, Syed AZ. Osteoma of the stylohyoid chain: A rare presentation in a CBCT study. Imaging science in dentistry. 2024 Mar:54(1):109-113. doi: 10.5624/isd.20230222. Epub 2024 Feb 6 [PubMed PMID: 38571770]
Brauer HU. [Calcified stylohyoid complex]. RoFo : Fortschritte auf dem Gebiete der Rontgenstrahlen und der Nuklearmedizin. 2024 Oct 30:():. doi: 10.1055/a-2443-1429. Epub 2024 Oct 30 [PubMed PMID: 39477216]
Warrier S A, Kc N, K S, Harini DM. Eagle's Syndrome: A Case Report of a Unilateral Elongated Styloid Process. Cureus. 2019 Apr 10:11(4):e4430. doi: 10.7759/cureus.4430. Epub 2019 Apr 10 [PubMed PMID: 31245217]
Level 3 (low-level) evidenceMonteagudo PT, Rossinol VL, do Nascimento Verreschi IT, Dias-da-Silva MR. Stylohyoid Ligament Calcification: A Greater-Than-Expected Cause of Otalgia in Turner Syndrome. Journal of the Endocrine Society. 2019 Jul 1:3(7):1403-1408. doi: 10.1210/js.2019-00009. Epub 2019 May 23 [PubMed PMID: 31286106]
Demirtaş H, Kayan M, Koyuncuoğlu HR, Çelik AO, Kara M, Şengeze N. Eagle Syndrome Causing Vascular Compression with Cervical Rotation: Case Report. Polish journal of radiology. 2016:81():277-80. doi: 10.12659/PJR.896741. Epub 2016 Jun 13 [PubMed PMID: 27354882]
Level 3 (low-level) evidenceLisan Q, Rubin F, Werner A, Guiquerro S, Bonfils P, Laccourreye O. Management of stylohyoid syndrome: A systematic review following PRISMA guidelines. European annals of otorhinolaryngology, head and neck diseases. 2019 Sep:136(4):281-287. doi: 10.1016/j.anorl.2019.05.002. Epub 2019 May 21 [PubMed PMID: 31126893]
Level 1 (high-level) evidenceNamiki C, Hara K, Tohara H, Kobayashi K, Chantaramanee A, Nakagawa K, Saitou T, Yamaguchi K, Yoshimi K, Nakane A, Minakuchi S. Tongue-pressure resistance training improves tongue and suprahyoid muscle functions simultaneously. Clinical interventions in aging. 2019:14():601-608. doi: 10.2147/CIA.S194808. Epub 2019 Mar 22 [PubMed PMID: 30962680]
Zhang Q, Shi Y, Cheng J, Chen Y, Wang J, Wang X, Deng L, Wu S. Impact of rTMS and iTBS on Cerebral Hemodynamics and Swallowing in Unilateral Stroke: Insights from fNIRS. Medical science monitor : international medical journal of experimental and clinical research. 2025 Jan 10:31():e944521. doi: 10.12659/MSM.944521. Epub 2025 Jan 10 [PubMed PMID: 39789787]