 Anatomy, Thorax, Superior Intercostal Arteries
Anatomy, Thorax, Superior Intercostal Arteries
Introduction
The superior intercostal artery (SIA), also known as the highest intercostal artery or the supreme intercostal artery, is a division of the costocervical trunk which itself originates from the subclavian artery. The superior intercostal artery passes inferiorly and posteriorly between the necks of the first and second ribs and the pleura. As it traverses the neck of the first rib, it diverges into two posterior intercostal arteries. These arteries function to supply blood to the first and second intercostal spaces.[1]
Though the SIA traditionally originates from the costocervical trunk, it may also arise from the thyrocervical trunk or its branches, including the dorsal scapular artery or inferior thyroid artery, among others. Knowledge of the structure, function, and variant pathways of the SIA becomes essential when operating in the neck and superior chest, particularly the 1 and 2 intercostal spaces. Aneurysm of the SIA is a rare vascular abnormality associated with coarctation of the aorta and neurofibromatosis type 1. In cases of aortic coarctation, the SIA may give rise to collateral arteries that help to supply arterial flow to the descending aorta.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The superior intercostal artery (SIA), also known as the highest intercostal artery or the supreme intercostal artery, is the first branch off of the costocervical trunk, which itself originates from the subclavian artery bilaterally. The superior intercostal artery courses inferiorly and posteriorly from its origin along the medial and posterior aspect of the thorax, between the pleura and the necks of the first and second ribs, typically dividing into two posterior intercostal arteries as it crosses the neck of the first rib. These arteries function to supply blood to the upper intercostal spaces of the first and second ribs in an analogous approach as the lower posterior intercostal arteries.[1][2]
Embryology
The SIA has historically been considered to anastomose at the convergence of the subclavian artery and the eighth and ninth branches of the intersegmental arteries. New research, however, suggests the SIA originates instead from the seventh and eighth intersegmental arteries and instead of the subclavian itself, by two arteries located posterior to it. The portions of the intersegmental arteries curl between the aorta and the anastomosis. Following this inward curvature, the SIA serves as the primary source of arterial blood to the posterior intercostal arteries associated with the first and second ribs.[3]
Blood Supply and Lymphatics
The SIA forms as a direct result of the embryologic development of the intersegmental arteries. The latter arteries are paired structures of the upper thorax and normally feed into the first and second intercostal arteries. The posterior intercostal arteries which branch from the SIA travel with the intercostal nerves and veins as a neurovascular bundle in the intercostal space inferior to the first and second ribs. The organization of the neurovascular bundle is as follows: the intercostal vein lies superior to the intercostal artery, which lies superior to the intercostal nerve. [4] The bundle runs between the internal intercostal muscle and innermost intercostal muscle and is shielded by the costal groove on the inferior/posterior aspect of each rib. The course of the anterior intercostal arteries mirrors that of the posterior intercostal arteries, and branches from the internal thoracic artery to supply collateral blood to the intercostal spaces. Thus, the internal thoracic artery supplies the anterior half of the upper six intercostal spaces, after which the internal thoracic artery branches into the musculophrenic artery and superior epigastric artery. The musculophrenic artery acts as the outlet for the other intercostal branches. The anterior and posterior intercostal arteries anastomose near the costal midline.[5]
Nerves
The intercostal nerves originate from the ventral rami of corresponding spinal nerves (For example, the T1 spinal nerve gives rise to the first intercostal nerve). These nerves innervate the skin of the thoracic wall, the intercostal muscles, the rib periosteum, and the costal parietal pleura. The intercostal nerves as a concept split into typical and atypical subcategories. The term "typical intercostal nerves" include those originating from T2 through T7, and the atypical intercostal nerves consist of T1 and T7 through T11. While the typical intercostal nerves remain restricted within the thoracic wall, the atypical intercostal nerves extend to supply other regions such as part of the brachial plexus (T1) and the majority of the abdominal wall (T7-11).[6][7][8]
Muscles
The intercostal muscles divide into the external intercostals, internal intercostals, and innermost intercostal muscles. Located most superficially, the external intercostal muscles extend posteriorly from the rib tubercle to the costochondral junction, where the external intercostal membrane replaces muscle fibers.[8] The internal intercostal muscle extends anteriorly from the sternum to the rib cage posteriorly, where the muscle fibers become replaced by the posterior intercostal membrane. The posterior intercostal arteries branching from the SIA enter the intercostal space deep to the internal intercostal muscle. The most anatomically deep of the muscle layers, the innermost intercostal muscle, is lined internally by endothoracic fascia, which itself has an internal lining of parietal pleura.[9]
Physiologic Variants
Variation in the SIA anatomy appears when considering both origin and distribution. Though the SIA historically originates from the costocervical trunk, it can also arise from the thyrocervical trunk. Branches of the thyrocervical trunk have also been reported to be the site of origination, including the dorsal scapular artery and the inferior thyroid artery. The SIA has also been described to arise from the aortic arch, axillary artery, second intercostal artery, and vertebral artery. When originating from the vertebral artery, the SIA is described to course through the transverse foramen of the seventh cervical vertebra, after which it courses inferiorly and then posterior to the ribs. In 72% of cases, research shows that the SIA supplies the first and second intercostal spaces, while in 20% of cases, it supplies only the first intercostal space, and in 8% of cases, it supplies both second and third spaces. Reports describe the SIA being minuscule in size when only supplying the first intercostal space.[10][11][12][13]
Surgical Considerations
Aneurysm of the superior intercostal artery is a rare vascular abnormality that is associated with coarctation of the aorta and neurofibromatosis type 1.[14] The treatment of choice for intercostal artery aneurysm is minimally invasive with selective endovascular embolization combining micro-coils and glue rather than a thoracotomy with ligation, clipping, or excision. The intercostal spaces supplied by the SIA receive collateral flow from the anterior intercostal arteries, so embolization is well tolerated. A dreaded complication of open procedures is a post-operative hematoma, which can expand to compress the brachial plexus, resulting in upper extremity paralysis.[15] Close follow-up with annual CT angiograms may be utilized to ensure resilient occlusion and to assess for disease progression.[14]
Clinical Significance
The SIA typically perfuses the 1 and 2 intercostal spaces, which can become clinically significant if the internal thoracic or anterior intercostal arteries become compromised. Additionally, in cases of coarctation of the aorta, the SIAs may give rise to mediastinal collateral arteries that bypass the coarctation and help to supply arterial flow to the descending aorta. The anterior intercostal arteries also serve to provide collateral flow to the descending aorta in cases of coarctation.[2]
Media
(Click Image to Enlarge)
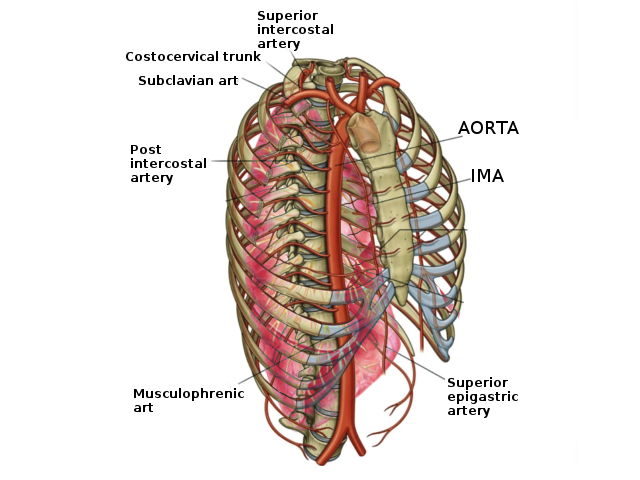
Superior intercostal artery Image courtesy S Bhimji MD
References
Helm EJ, Rahman NM, Talakoub O, Fox DL, Gleeson FV. Course and variation of the intercostal artery by CT scan. Chest. 2013 Mar:143(3):634-639. doi: 10.1378/chest.12-1285. Epub [PubMed PMID: 23079732]
Kirks DR, Currarino G, Chen JT. Mediastinal collateral arteries: important vessels in coarctation of the aorta. AJR. American journal of roentgenology. 1986 Apr:146(4):757-62 [PubMed PMID: 3485349]
Level 3 (low-level) evidenceGailloud P. The supreme intercostal artery includes the last cervical intersegmental artery (C7) - angiographic validation of the intersegmental nomenclature proposed by Dorcas Padget in 1954. Anatomical record (Hoboken, N.J. : 2007). 2014 May:297(5):810-8. doi: 10.1002/ar.22893. Epub 2014 Mar 7 [PubMed PMID: 24610867]
Level 1 (high-level) evidencePalussière J, Canella M, Cornelis F, Catena V, Descat E, Brouste V, Montaudon M. Retrospective review of thoracic neural damage during lung ablation - what the interventional radiologist needs to know about neural thoracic anatomy. Cardiovascular and interventional radiology. 2013 Dec:36(6):1602-1613. doi: 10.1007/s00270-013-0597-z. Epub 2013 Apr 11 [PubMed PMID: 23576208]
Level 2 (mid-level) evidenceGlenesk NL, Rahman S, Lopez PP. Anatomy, Thorax, Intercostal Nerves. StatPearls. 2023 Jan:(): [PubMed PMID: 30855826]
Haam S, Kim D, Hwang J, Paik H, Lee D. An anatomical study of the relationship between the sympathetic trunk and intercostal veins of the third and fourth intercostal spaces during thoracoscopy. Clinical anatomy (New York, N.Y.). 2010 Sep:23(6):702-6. doi: 10.1002/ca.21001. Epub [PubMed PMID: 20533514]
Donley ER, Holme MR, Loyd JW. Anatomy, Thorax, Wall Movements. StatPearls. 2023 Jan:(): [PubMed PMID: 30252279]
Clemens MW, Evans KK, Mardini S, Arnold PG. Introduction to chest wall reconstruction: anatomy and physiology of the chest and indications for chest wall reconstruction. Seminars in plastic surgery. 2011 Feb:25(1):5-15. doi: 10.1055/s-0031-1275166. Epub [PubMed PMID: 22294938]
Miller JI Jr. Muscles of the chest wall. Thoracic surgery clinics. 2007 Nov:17(4):463-72. doi: 10.1016/j.thorsurg.2006.12.007. Epub [PubMed PMID: 18271161]
Yuan SM. Isolated costal cartilage fractures: the radiographically overlooked injuries. Folia morphologica. 2017:76(1):139-142. doi: 10.5603/FM.a2016.0030. Epub 2016 Nov 10 [PubMed PMID: 27830867]
Gailloud P. The supreme intercostal artery in its most rudimentary form does not branch off any intercostal arteries. Anatomical record (Hoboken, N.J. : 2007). 2015 May:298(5):781-2. doi: 10.1002/ar.23092. Epub 2014 Nov 20 [PubMed PMID: 25388017]
Level 3 (low-level) evidenceTubbs RS, Salter G, Wellons JC 3rd, Oakes WJ. Blood supply of the human cervical sympathetic chain and ganglia. European journal of morphology. 2002 Dec:40(5):283-8 [PubMed PMID: 15101443]
Brasileiro Filho G,Pena SD, Molecular biological techniques for the diagnosis of infectious diseases. Revista da Sociedade Brasileira de Medicina Tropical. 1992 Jan-Mar; [PubMed PMID: 1308067]
Fenwick A, Omotoso P, Ferguson D. Endovascular management of unruptured intercostal artery aneurysms. CVIR endovascular. 2019:2(1):2. doi: 10.1186/s42155-018-0048-7. Epub 2019 Jan 4 [PubMed PMID: 30652168]
Aizawa K, Iwashita C, Saito T, Misawa Y. Spontaneous rupture of an intercostal artery in a patient with neurofibromatosis type 1. Interactive cardiovascular and thoracic surgery. 2010 Jan:10(1):128-30. doi: 10.1510/icvts.2009.222125. Epub 2009 Oct 15 [PubMed PMID: 19833637]
Level 3 (low-level) evidence