Introduction
Strabismus is derived from a Greek word that translates to "eyes looking obliquely" and means misaligned eyes.[1] Often, strabismic eyes are referred to as "squinting eyes," "crossed eyes," and "wall eyes." Typically, both eyes fixate equally while focusing on an object with the head held in the primary position. In strabismus or squint, 1 or both eyes deviate inwards or outwards and appear to be in nonalignment towards the direction of the focused object (see Image. Strabismus). It can be due to refractive error, binocular fusion abnormalities, or neuromuscular anomalies of ocular movements.[2] If diagnosed and treated early, strabismus has an excellent prognosis. Treatment is usually by refractive error correction, orthoptic exercises, occlusive patching, topical medications, and extraocular muscle surgery.
Orthophoria is defined as the perfect ocular alignment, even when no stimulus for fusion is present. Orthotropia is defined as the correct direction of the eyes under binocular conditions. Both of these terms describe eyes without any manifest strabismus.
Heterophoria is defined as an ocular deviation kept in control by a fusional mechanism. Heterotropia is defined as the deviation that is present on the corneal reflex test itself. This is the manifest deviation that can be related to underlying amblyopia.[3]
The different deviations can be defined as follows:
- Eso- This is a convergent strabismus in which the eyeball deviates nasally.
- Exo- This is a divergent strabismus in which the eyeball deviates temporally.
- Hyper- This is a vertical strabismus in which the eyeball deviates superiorly.
- Hypo- This is a vertical strabismus in which the eyeball deviates inferiorly.
- Incyclo- The eyeball is intorted, and the superior pole of the vertical meridian is rotated nasally.
- Excyclo- The eyeball is extorted, and the superior pole of the vertical meridian is rotated temporally.[4]
Based on the age of onset of strabismus, it can be defined as infantile when the deviation of eyes has been noticed at or before 6 months of age. Strabismus is defined as acquired if the deviation is noticed after 6 months of age, following a presumed normal ocular alignment.
Further, the strabismus is called comitant if the angle of deviation remains the same in different positions of gaze. It is called incomitant if the deviation varies in size in different positions of gaze.[5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Strabismus or Squint is Broadly Classified as
- Pseudostrabismus or apparent squint: Pseudoesotropia and pseudoexotropia
- Latent squint (Heterophoria)
- Manifest squint (Heterotopia): Concomitant squint and incomitant squint [6]
Causes for Pseudostrabismus
- Pseudoesotropia: Prominent epicanthal fold and negative angle kappa
- Pseudoexotropia: Hypertelorism and positive angle kappa [7]
Causes for Heterophoria
- Anatomical causes: Orbital asymmetry, abnormal interpupillary distance (IPD), mild weakness of extraocular muscles, etc.
- Physiological causes: Esophoria is seen in increased accommodation (hyperopes) and exophoria in decreased accommodation (myopes), excessive or decreased use of convergence, and in dissociated works like working with a uniocular microscope or magnifying glasses.
- Decompensation causes psychiatric disorders, illness, inadequacy of the fusional reserve, older age, and precision jobs.[8]
Causes of Concomitant Squint
- Sensory causes: Interfere with a clear image formation in 1 eye and include refractive errors, anisometropia, media opacities, obstruction of pupillary area, macular and optic nerve diseases, and wrong glass prescription for refractive error.[9]
- Motor causes: Interfere with ocular alignment and include orbital, extraocular muscle, and accommodation abnormalities.[10]
Causes of Incomitant Squint
- Neurogenic causes: Hypoplasia of 3rd, 4th, and 6th cranial nerve nuclei, tumors, infections, trauma, toxicity (alcohol, lead, carbon monoxide), vascular (ophthalmoplegic migraine), and demyelinating lesions affecting the third and sixth cranial nerves.[11]
- Myogenic causes: Congenital lesions, trauma, muscle incarceration in orbital fractures, post-viral myositis, and chronic progressive external ophthalmoplegia (CPEO).
- Neuromuscular junction disorders: Myasthenia gravis.[12]
Risk Factors
Strabismus is more prevalent with certain syndromes like Down syndrome, cerebral palsy, Apert-Crouzon syndrome, premature infants with low birth weight, and children with affected parents or siblings. All siblings of a strabismic child should be screened at an early age for strabismus as sensorimotor anomalies are common in the pedigrees of strabismic probands.[12]
Epidemiology
The prevalence of strabismus is 2% to 5% in the general population.[13][14]. In the U.S., 5 to 15 million individuals are affected by strabismus. In a National Health Survey, exotropia was seen in 2.1% and esotropia in 1.2% of the population aged 4 to 74 years. This difference is due to the higher prevalence of exotropia in the population between 55 to 75 years of age.[14]
Fifty percent of all childhood esotropias are either fully or partially accommodative. Non-accommodative esotropia is seen in 10% of all strabismus cases and is the second most common form of childhood esotropia.[15] Infantile esotropia affects 1 in every 100 to 500 persons, which accounts for 8.1% of cases of esotropia.[16]
Intermittent esotropia is seen in 1% of the population and is the most common form of exotropia.[17][18] Exotropia is more prevalent in Asian and black populations.[19] Women make up 60% to 70% of exotropia cases.[20]
Pathophysiology
Etiopathogenesis of strabismus is unclear. The physiology of ocular motility involves extraocular muscles, cranial nerves, supranuclear pathways, and their cerebral controls. All of these have been implicated in the development of strabismus. The following 2 theories are popular:
- Claude Worth's theory states that an inherent absence of cortical fusional potential is the cause of strabismus.[21]
- Chavasse theory states that motor alignment leads to a poor sensory status, which, if left untreated, leads to strabismus. This theory justifies early treatment for squint, which leads to sustained improvement in binocular single vision (BSV). Hence, many surgeons justify doing early surgery in conditions like infantile esotropia.[3]
Concerning muscle innervation and action, the following 2 laws of ocular motility govern extraocular motility.
- Sherrington's law of reciprocal innervation: Increased innervation to a muscle is accompanied by decreased innervation to its antagonist. Exception: Duane retraction syndrome.[22]
- Herring law of equal innervation: Equal and simultaneous innervation flows through synergistic muscles during any conjugate eye movement. Exception: Dissociated vertical deviation.[23]
Histopathology
Falki et al. studied specimens of extraocular muscles from strabismus patients and found the fibers to be disarranged, atrophied, swollen, and disintegrated. In contrast, skeletal muscle fibers of unaffected patients have tight, normally arranged fibers with clear striations.
Transmission electron microscopy of normal extraocular muscles shows an intact basal membrane, sarcolemma, tightly aligned myofibrils with well-arranged sarcomeres, a Z line, and an H zone, and normally distributed mitochondria. Strabismic extraocular muscles reveal vacuolation and degeneration of myofibrils, lipid droplet accumulation, subsarcolemmal inclusions, and mitochondrial clustering. Histopathology of the extraocular muscles in patients with Down syndrome shows extensive vacuolation, myofibril disintegration, and intracellular and extracellular deposition of collagen fibrils.[24]
History and Physical
Although strabismus can occur at any age, it is commonly seen before 6 years, with a peak onset of about 3 years. Parents often claim that their child has crossed eyes since birth. Family photographs often help to document the age of onset. Moreover, pictures might show ocular preference in fixation. Alternating fixation denotes an absence of amblyopia in squinting infants. Strong fixation of 1 eye implies strabismic amblyopia in the other eye.[1] A low birth weight history indicates prematurity retinopathy, which might lead to pseudostrabismus from the ectopic macula.
The acute onset of esotropia in an older child always requires a thorough evaluation to rule out neurological abnormalities. Intermittent strabismus indicates a better recovery of normal binocular vision, implying that fusion is present part of the time. Photosensitivity is commonly seen in intermittent exotropia and is caused by a decreased binocular photophobia threshold.[25] Obtaining a detailed history of possible allergy to dilating drops, familial hepatic porphyria, sensitivity to suxamethonium, and malignant hyperthermia is essential to prevent fatal anesthetic complications during surgical management of strabismus.[26]
The important questions that should be asked of parents or caretakers should include the age of onset of deviation, preceding history of physical illness, nature of deviation–constant or intermittent, change in deviation with illness or fatigue, if the deviation is constant or intermittent, and whether the deviation occurs dominantly in 1 eye or alternates.[4]
Clinical features of the commonly occurring strabismus conditions include the following:
Essential Infantile Esotropia (Congenital Esotropia)
Large angle stable esotropia, which presents within 6 months of age with a positive family history and no neurological deficit. Refractive error is uncommon, with poor potential for BSV. Cross fixation, asymmetrical optokinetic response, and latent horizontal nystagmus are seen. Dissociated vertical deviation (DVD) develops in 80% of children by 3 years of age. Treatment is aimed at correcting hyperopia and treating amblyopia. Muscle surgery should be performed early, between 6 months to 2 years of age.[27]
Accommodative Esotropia
Onset is between 2 to 5 years of age with <10 prism diopters (PD) deviation and precipitated by trauma or illness. Family history and amblyopia are common. Mechanisms involved in accommodative esotropia are uncorrected hypermetropia, accommodative convergence, and poor fusional divergence. Normal accommodation convergence/accommodation ratio (AC/A ratio) with hyperopia >2 diopters (D) is seen in the refractive type, while the nonrefractive type shows a high AC/A ratio with no clinically significant hyperopia. Treatment includes full cycloplegic correction and short-term miotics if children are intolerant to spectacles. If the AC/A ratio is high, bifocals are prescribed with minimum plus add given for near vision. Surgery is indicated if the residual esotropia is >10 PD.[28]
Microtropia
Microtropia or monofixation syndrome is a unilateral abnormality of BSV with amblyopia and ultra-small angle deviation of <5° or 8 PD. Anisometropia is seen in nearly all patients with reduced stereopsis, abnormal retinal correspondence (ARC), normal motor fusion, and foveal suppression scotoma. A ‘4-prism diopter’ placed base out in front of the non fixating eye will not show any refixation movement in microtropia as the image will be shifted within the central suppression scotoma. Treatment is by correcting anisometropia and amblyopia.[29]
Intermittent Exotropia
This presents around 2 years of age with exophoria, which breaks down to exotropia under conditions of visual inattention, bright light, fatigue, or ill health. Other features include headache, asthenopia, diplopia, photo-diplopia, micropsia, abnormal stereopsis, and temporal retinal hemisuppression. Treatment should begin with correcting refractive errors and treating amblyopia. Orthoptic exercises with pencil pushups help to some extent. A bilateral lateral rectus recession is commonly performed strabismus surgery to correct the divergence excess.[30]
Dissociated Vertical Deviation (DVD)
This bilateral, asymmetric, and asymptomatic strabismus manifests around 2 years of age and is commonly associated with congenital esotropia (75%). It presents as an updraft with excyclotropia of the eye undercover or during visual inattention. When the cover is removed, the affected eye will move down without the corresponding downdrift of the other eye. This downdrift of the occluded eye is also seen when the fixating eye is occluded with increasing neutral density filters. This is called the ‘Bielschowsky phenomenon’ and is specific to DVD. Inferior oblique overaction (IOOA) is the most common differential diagnosis of DVD, demonstrating an absent Bielschowsky phenomenon. The surgery of choice is superior rectus recession with retroequatorial myopexy (Faden procedure).[31]
Monocular Elevation Deficiency
Also called ‘double elevator palsy,’ this condition presents as a unilateral total inability to elevate with hypotropia in primary gaze, ptosis, and chin-up position. The Knapp procedure (full tendon width vertical transposition of horizontal recti) for superior rectus weakness and inferior rectus recession for inferior rectus restriction is the procedure of choice.[32]
Alphabet Patterns
The alphabet pattern is strabismus, where the horizontal deviation changes from upgaze and downgaze. V pattern is more common than A pattern.[33]
Duane Retraction Syndrome
This congenital syndrome presents as a globe retraction on adduction with palpebral fissure narrowing. In severe cases, globe up-shoot or down-shoot is seen with adduction. It is commonly seen in females with a preponderance to the left eye and is seen bilaterally in 20% of cases. It arises due to a congenital innervation of the lateral rectus by the third cranial nerve due to agenesis of the sixth cranial nerve (pontine agenesis). Globe retraction is due to the co-contraction of both the medial and lateral rectus. Surgery is indicated in significant heterotopia in primary gaze, abnormal head position, cosmetically unacceptable globe retraction, and up-shoot/down-shoot movements.[34]
Brown Syndrome
This restrictive disorder of the superior oblique tendon can be congenital or acquired and presents as a limitation of elevation in adduction. It presents bilaterally in 10% of cases, commonly seen in females and affecting more often the right eye. Acquired causes are due to trauma or inflammation (rheumatoid arthritis, sinusitis, scleritis, etc) to the superior oblique tendon. The forced duction test is positive on retropulsion.[35]
Mobius Syndrome
This presents as an inability to abduct either eye past midline, with vertical gaze being normal, and is due to congenital bilateral aplasia of the sixth and seventh cranial nerve.[36]
Oculomotor Palsy
Third cranial nerve palsy presents as ptosis with abducted and intorted eye with defective accommodation.[37]
Lateral Rectus Palsy
This condition presents as an esotropic eye with a limitation of abduction.[38]
Superior Oblique Palsy
This disorder presents as an ipsilateral limitation of depression on adduction, excyclotorsion, and vertical and torsional diplopia on looking down. A Parks 3-step test helps diagnose the paretic muscle in vertical diplopia, especially in superior oblique palsy. A right superior oblique palsy presents as hypertropia on the primary gaze with increasing hypertropia on the left gaze and the right-sided head tilt.[39] The head is tilted and turned towards the opposite side with a depression of the chin. Bilateral cases show right hypertropia in the right gaze and left hypertropia on the left gaze with >10° of cyclodeviation on the double Maddox rod test and chin depression without head tilt. It is seen both as a congenital or acquired disorder. Acquired causes are trauma, vascular lesions, aneurysms, and tumors. Surgery involves superior oblique strengthening by tucking/tenoplication or the Harada Ito procedure (splitting and anterolateral transposition of the lateral half of the superior oblique tendon).[40]
Evaluation
Visual Acuity
Infants
'CSM' method is a simple technique to observe fixation and followability. With a simple torch, observe the corneal reflex while moving it from side to side. Central corneal light reflex shows "central" fixation and the followability of the eye sidewards to the torch is termed "steady." If both eyes are in alignment during the movement, then it is termed as "maintained."[41]
Preverbal Children
Preferential-looking tests, eg, Cardiff picture card [42]
Uncooperative Children
Children might cry or object to occluding the eye with good vision [43]
Children
Snellen charts, Illiterate E chart, Sheridan-Gardiner chart [44]
Stereoacuity
Stereoacuity measures the visual sense of depth. It is the sense of fusion of 2 simultaneous, slightly dissimilar images with integration by the brain. Titmus stereo-fly test and Lang cards are commonly used. The Worth 4-dot test and Bagolini striated glasses are used to assess the fusional reserve, while both stereopsis and fusion can be assessed by synoptophore.[45]
Compensator Head Posture (CHP)
CHP is a motor adaptation to strabismus to attain binocular single vision (BSV). Loss of CHP in concomitant strabismus may indicate the loss of BSV and warrants surgical intervention. In acquired paretic strabismus, CHP eliminates diplopia and helps to centralize the binocular visual field. Head tilt, face turn, and chin up/down are commonly seen as abnormal head postures. A head tilt to the left is seen in the right superior oblique palsy. A face turn to the left is seen in left lateral rectus palsy. Chin up or down is seen in the "A" or "V" pattern strabismus.[46]
AC/A Ratio
The accommodative convergence/accommodation (AC/A) ratio is the amount of convergence in prism diopters per diopter change in accommodation. Two methods are used to measure the AC/A ratio: the lens gradient method and the heterophoria method. The normative range lies between 3 and 5 to 1.[47]
Measurement of Deviation
- Hirschberg test: The Hirshberg test gives a rough estimate of the angle of manifest strabismus by noting the position of the corneal light reflex produced by shining a torchlight over the cornea. Each millimeter of deviation equals 7° of deviation or 14 prism diopters (PD), assuming the pupil is 4 mm in diameter. If the light reflex is at the temporal border of the pupil, then the angle of deviation of esotropia is about 15°, and if it is at the limbus, the angle is about 45°.[48]
- Krimsky test: This test uses prisms placed in front of the fixating eye to measure the deviation. The modified Krimsky test is done by holding the prism in front of the deviating eye. This test is essentially used to measure tropias and not for phorias.[49]
- Cover test: The cover test is performed to detect heterotropia. The fixating eye is covered, and movement of the uncovered eye is noted both for distance and near.[50]
- Uncover test: The uncover test detects heterophoria. After covering an eye for 2 to 3 seconds, the same eye movement is observed on uncovering. This test is done for both distance and near. Most examiners do the cover test and uncover test sequentially; hence, it is called the "cover-uncover" test.[51]
- Alternate cover test: This dissociation test reveals the total deviation when fusion is interrupted and should be performed only after the cover-uncover test. Patients with poor fusional control may decompensate to a manifest deviation when this test is done. The speed and smoothness of recovery are noted following a fast cover-uncover test done alternatively to both eyes.[52]
- Prism cover test: This test combines the alternative cover test with a prism for both near and distant fixation.[53]
- Maddox wing: This test dissociates the eyes for near fixation (33cm) and measures heterophoria. When seeing through this instrument, the right eye sees only the arrows (white vertical and red horizontal), while the left eye sees only rows of numbers (horizontal and vertical). The white arrow position denotes horizontal deviation, and the red arrow denotes vertical deviation. By aligning the red arrow parallel to the horizontal row of a number, cyclophoria can be measured.[54]
- Maddox rod: Maddox rod converts a white light spot into a perpendicular red streak by a series of fused cylindrical red glass rods. The amount of dissociation is calculated by the superimposition of the 2 images using the prisms.[55]
Ocular Motility: Extraocular movements involve the assessment of smooth pursuit movements followed by saccades.
- Versions: All 9 diagnostic positions of gaze binocularly are assessed with a torch or a pen, and the cover-uncover test is done in each cardinal position to assess tropia/phoria.[51]
- Ductions: Ductions are monocular eye movements elicited in all 6 cardinal positions by occluding the other eye. Ductions are assessed if either or both eyes' ocular motility limitations are noticed. Underaction is graded from -1 to -4 with increasing degrees of underaction, and 0 indicates full movement.[56]
- Vergence: convergence and divergence movements
- Near point of convergence: Near point of convergence (NPC) is the nearest point at which the patient reports diplopia when tested with an RAF rule. It should be nearer than 10 cm.
- Near point of accommodation: Near point of accommodation (NPA) is the nearest point at which the eyes can maintain clear focus when tested with the RAF rule. At 20 years of age, it is 8 cm and recedes to 46 cm by 50 years.
- Fusional amplitudes: Fusional amplitudes measure the efficacy of vergence movements and are tested with prism bars or synoptophores.
- Postoperative diplopia test: This test is mandatory for all patients older than 7 years before strabismus surgery. Prisms larger than the planned correction for the deviation are placed in front of the deviating eye. If suppression is seen, the risk of diplopia following surgery is less. Intermittent or constant diplopia is an indication to do diagnostic botulinum toxin tests before the surgery.[57]
Field of BSV: The field of BSV is that area where bifoveal fusion of the object of regard occurs. The Hess chart assesses the field of BSV to diagnose and monitor patients with incomitant strabismus caused by either extraocular muscle palsy (third, fourth, or sixth cranial nerve palsies) or restriction (thyroid ophthalmopathy, blow-out fracture, or myasthenia gravis). The Hess chart uses either the Hess screen or Lees screen to chart the field by dissociating the ocular movements. Hess's screen uses a tangent screen with red-green goggles, and Lees's screen uses 2 glass screens at right angles.[58]
The following is the interpretation of the Hess chart appearance:
- Smaller chart: indicates the eye with the paretic muscle, and the greatest restriction is in the direction of the paretic muscle.
- Larger chart: indicates the eye with an overacting muscle, and the greatest expansion is in the main direction of action of the yoke muscle.[59]
The following sequelae are seen in the muscles in a paretic squint:
- Overaction of the ipsilateral antagonist (contracture)
- Secondary inhibition palsy of the antagonist of the yoke muscle [60]
Refraction: Assessing the correct refractive error and power is crucial in managing strabismus. Most commonly, hypermetropia is seen in strabismus patients. Refraction should be done under both non cycloplegic and cycloplegic conditions. Instilling 1 drop of 1% cyclopentolate hydrochloride twice at 5-minute intervals, followed by retinoscopy 30 minutes later, is the standard practice.[61]
Forced Duction Test (FDT): This test is done to assess if the limitation of movement is due to the mechanical restriction of the muscle (fibrosis/tethering). The anesthetized conjunctiva of the eyeball is held with forceps and moved first in the direction of the muscle action and later in all directions to see if there is a restriction on the movement of the eyeball. This test should be mandatorily performed before any strabismus surgery.[62]
Parks-Bielschowsky 3-Step Test: This test is done in acquired vertical diplopia to isolate the paretic muscle. Step 1: Which eye is hypertrophic in the primary gaze? Step 2: Is the hypertropia worsening of the right or left gaze? Step 3: Is the hypertropia worsening with the right head tilt or left head tilt? This test helps in diagnosing superior oblique palsy.[63]
Fundoscopy: A dilated fundus examination is mandatory to rule out intraocular pathologies like optic disc hypoplasia, macular scarring, or retinoblastoma, which might cause squint.[64]
Investigations for Strabismus: Neuroimaging is essential, especially in sudden onset adult-onset strabismus, to rule out stroke, diabetic mononeuritis, myasthenia gravis, thyroid eye disease, etc. Rarely, a primary neurological disorder such as hydrocephalus, optic nerve glioma, medulloblastoma, or craniopharyngioma might cause childhood strabismus and need neuroimaging.[51]
4-Prism Base-Out Test: This test is important in diagnosing patients with small facultative scotoma and no obvious, manifest deviation. A 4-prism with the base out is placed before 1 eye while the patient is viewing binocularly, and ocular movements are noted in both tests. Patients with bifixation show a version movement toward the apex of the prism. The eye under the prism moves toward the prism apex, and the other eye moves along as per Hering's law. This is followed by a recovery movement in the other eye to restore binocular vision. In patients with monofixation, no movement is observed when the prism is placed before the non fixating eye. Similarly, there is the absence of recovery movement if the other eye is the non fixating eye. This helps in the diagnosis of microtropia or monofixation syndrome.[65]
Prism Adaptation Test: The binocular function is tested with prisms. The ocular alignment is achieved with prisms, which help predict whether the patient will achieve postsurgical fusion or prismatic alignment.[66]
Treatment / Management
The primary aim of treating strabismus is to restore proper ocular alignment. The secondary aims are to treat amblyopia, maintain binocularity, and eliminate diplopia. See Image. Strabismus Surgery.
The various methods of treating strabismus are as follows:
Observation: Strabismus secondary to myasthenia gravis, diabetic mononeuropathy, and posttraumatic restrictive strabismus mainly improve with time and the treatment of the primary cause. Some healthy neonates show intermittent deviation of the eyes. These are called ‘neonatal ocular misalignments,’ which improve by 2 months and resolve in 4 months. They usually reflect a normally developing vergence system.[67]
Correction of Refractive Errors: The first step in managing any child with strabismus is to evaluate for a refractive error and correct it fully. The full correction of hypermetropia is the treatment of choice for all forms of esotropia. Full correction without subtracting any lens power for cycloplegia is prescribed. In convergence excess esotropia, executive bifocals are prescribed to relieve accommodation and thereby prevent accommodative convergence. A minimal plus “add” required is prescribed with the flat top of the bifocal segment bisecting the upper border of the pupil.[28] In intermittent exotropia, full myopic correction often controls the exotropia.[68] (B3)
Amblyopia Treatment: Amblyopia in strabismus is reduced visual acuity in 1 or both eyes because of misalignment of eyes in the absence of any demonstrable visual pathway abnormality. Refractive correction alone is successful in improving amblyopia in nearly one-third of patients.[69] Patching the better eye to force the brain to use the weaker eye is the gold standard treatment for amblyopia. Patching the better eye for 2 to 6 hours per day is recommended and is most effective with children younger than 7. Atropine penalization (atropine 1% eyedrops twice daily in the better eye) is also as effective as occlusion.[70][71] As the effect of atropine actions lasts 2 to 3 weeks, frequent follow-ups are necessary to detect occlusion/reversal amblyopia of the better eye. (A1)
Orthoptics: Orthoptic exercises are commonly used to treat intermittent exotropia. Fusional exercises like “pencil push-ups” are done with a pencil held at arm’s length and slowly moved towards the nose, thereby inducing accommodation and strengthening convergence, which helps treat exotropia.
Prismatic Correction: Ophthalmic prisms move the image closer to the fovea and help improve sensory fusion. They are prescribed for deviations <20 PD. Amblyopia, suppression, and anomalous retinal correspondence are contraindications for prism therapy.[72]
Pharmacological Therapy: Miotics act by inducing peripheral accommodation so that the patient uses less accommodation, thus reducing esotropia. Ecothiopate iodide 0.125% once daily is a short-term treatment for accommodative esotropia patients. This can be used for children too young or intolerant of glasses.[73]
Botulinum Toxin: Botulinum toxin type A is used as a form of chemodenervation to cause temporary paralysis of the extraocular muscle, improving the strabismus. It is used as an adjunct to surgical therapy and to assess postoperative diplopia if anticipated following strabismus surgery. This can induce transient ptosis and vertical strabismus.[74]
Extraocular Muscle Surgery: Strabismus surgery should be considered only after conservative treatments have failed to correct the deviation. Esotropias with >15 PD and exotropia with >20 PD following full spectacle correction are candidates for surgery. Accommodative esotropias are not ideal candidates for surgery as surgery induces consecutive esotropia.[75][76] The ideal age for infantile strabismus surgery is before 2 years of age. A postsurgical deviation of <10 PD yields better binocular vision, whereas to achieve stereopsis, the residual deviation should be ≤4 PD.[77] A 60% reduction of the overall deviation or a deviation of ≤10 PD 6 weeks post-surgery is considered a successful outcome of horizontal strabismus surgery.[78](B2)
The 3 main types of strabismus surgery are:
- Weakening Procedures: These decrease the effective strength of muscle action. Recession, retro equatorial myopexy or posterior fixation (Faden procedure), marginal myectomy, and myectomy (disinsertion) are weakening procedures.
- Strengthening Procedures: These procedures enhance the pull of the muscle. Resection, advancement, double-breasting or tenoplication, and cinching are the strengthening procedures.
- Vector Adjustment Procedures: These transposition procedures alter the direction of muscle action. Hummelscheim, Jensen, O’Connor, Knapp, Callahan, Peter, and Helveston are examples of transpositioning procedures.[79]
Important considerations include the following:
Congenital/infantile esotropia: Early alignment is the key to developing binocular function. The first and most important step is correcting any underlying refractive errors and amblyopia management. The ideal age for surgical correction is by the age of 12 months, and the maximum age is 24 months. The surgical treatment of choice is either a bilateral medial rectus recession or a unilateral recession resection procedure. Angles >50° require bilateral medial rectus recession with unilateral lateral rectus resection. An alignment within 10 prism dioptres is an acceptable goal.[80]
Accommodative esotropia: In this case, the AC/A ratio is normal. There is often an underlying hypermetropia of +2.00 to +7.00 D. Cycloplegic retinoscopy is a must in these cases. Fully accommodative esotropia gets fully corrected with optical correction. BSV is present at all distances with optical correction. Partially accommodative esotropia gets partially corrected with full hypermetropia glasses.[28]
Nonrefractive accommodative esotropia: The AC/A ratio is high, which means there is a greater increase in convergence with each dioptre of accommodation used by the patient. Any underlying refractive errors should be first treated. Full cycloplegic refraction should be prescribed with only distance reduction. Bifocal glasses should be considered for convergence excess esotropia.[81](B2)
Early-onset exotropia: Treatment is mainly surgical and includes lateral rectus recession and medial rectus resection.[82](B2)
Intermittent exotropia: The initial step is to rule out any underlying refractive errors. Spectacle correction in myopic patients can stimulate the accommodation and control deviation. Part-time occlusion of the dominant eye can improve control in some patients. Orthoptic exercises may be helpful to control the near deviation. Surgical correction is indicated in patients with poor control or loss of distance stereopsis. Unilateral recession resection procedures are generally preferred except in the case of true distance exotropia, where lateral rectus recessions may be preferred.[83](A1)
Sensory exotropia: Correction of visual deficit should be targeted first. The correction of deviation follows this. Surgery over the nondominant eye should be done first. Any residual deviations can be corrected in the other eye.[84]
Pattern deviations: A “V” pattern is significant if the difference between upgaze and downgaze is >15 PD. V pattern esotropia can be corrected by bilateral medial rectus recession with downward displacement of tendons. V pattern exotropia can be corrected by bilateral lateral rectus recessions with an upward displacement of tendons.[33]
An “A” pattern is significant if the difference between upgaze and downgaze is >10 PD. For A pattern esotropia, bilateral medial rectus recessions with upward transposition of tendons are advocated. For A pattern exotropia, bilateral lateral rectus recessions with downward transposition of tendons can be planned.[85]
Differential Diagnosis
Differential diagnoses can be classified based on the type of defect. Important differentials to be considered are as follows:
Congenital Esotropia
- Early-onset accommodative esotropia
- Abducens palsy
- Nystagmus blockage syndrome
- Duane retraction syndrome
- Sensory esotropia
- Strabismus fixus
- Moebius syndrome [86]
Fully Accommodative Esotropia
- Non-accommodative esotropia
- Congenital esotropia
- Cyclic esotropia
- Convergence excess and near esotropia [87]
Intermittent Exotropia
- Infantile exotropia
- Convergence weakness or insufficiency
- Sensory exotropia with poor unilateral vision [30]
Prognosis
The prognosis of strabismus is excellent if detected and managed early in life. Healthy neonates sometimes show intermittent deviation of the eyes, which should not be a concern. At about 3 months, normal binocular coordination sets in, and any strabismus persistent after this period should be considered abnormal and significant. Amblyopia sets in if the strabismus is not appropriately managed before 6 to 8 years of age, leading to a permanent decrease in vision. It is essential to know the indications for ophthalmologist referral.[1]
Indications for ophthalmologist referral include the following:
- Altered pupillary reflex or leukocoria
- Constant esotropia
- Incomitant strabismus
- Persistent esotropia at or after 4 months of age
Complications
Complications of strabismus include the following:
- Amblyopia
- Reduced stereopsis
- Asthenopia
- Diplopia
- Nystagmus
- Abnormal head and neck posture
- Impaired social and mental growth
Surgical treatment for strabismus may result in the following:
- Diplopia
- Under/over-correction
- Conjunctival scarring, granuloma, and chronic inflammation
- Corneal dellen
- Scleral perforation
- Lost muscle
- Endophthalmitis
- Anterior segment ischemia
- Retrobulbar hemorrhage
Postoperative and Rehabilitation Care
Postoperative care should include measurement of alignment and evaluation for any obvious over- or under-corrections. Any slipped muscle or unexpected results may warrant exploration in the immediate postoperative period. Low-dose steroids for the initial postoperative period are usually sufficient to control inflammation. Oral nonsteroidal anti-inflammatory drugs may be added for 2 to 3 days in the immediate postoperative period.[88]
Consultations
Any patient presenting with a deviation of the eyeball should undergo a preliminary evaluation by an ophthalmologist. All cases with deviation should undergo a thorough evaluation by a pediatric ophthalmologist and strabismologist to understand the type of strabismus and the necessary intervention. The parent should be helped to understand the nature of pathology and the need for other consultations such as neurology, neurosurgery, and pediatrics.[51]
Deterrence and Patient Education
Parents should be aware of the prognosis, advantages, and complications of managing strabismus and its impact on the child's physical, social, and psychological growth. A treatment plan based on the discussion with the parents should be charted out.[89] In acute onset strabismus, patients and their care providers should be informed about a possible systemic or neurological cause and a possible referral to an appropriate specialist if needed. The parents must know the risks of developing amblyopia and impaired stereopsis if treatment adherence is not maintained.[51]
Pearls and Other Issues
Strabismus is a subspecialty of ophthalmology that is challenging to understand and requires the intervention of pediatric ophthalmologists and strabismologists. Strabismus includes a wide variety of pathologies and needs intervention at the correct age to prevent amblyopia and permanent deviation.[90]
Enhancing Healthcare Team Outcomes
Enhancing patient-centered care and improving outcomes for strabismus necessitates a multidisciplinary approach. The treatment of strabismus in children may occur in various clinical settings. The interprofessional team includes ophthalmologists, orthoptists and optometrists, community pediatricians, general practitioners, psychologists, pharmacists, and nurses. In addition to these varied healthcare professionals, teachers, school nurses, and community optometrists also play an essential role in managing children with strabismus.
Early identification of strabismus is paramount. All team members should be skilled in screening for strabismus and understanding the risk factors and signs that warrant immediate attention. Each team member should possess specialized skills and knowledge relevant to strabismus diagnosis, treatment, and patient education. This includes expertise in ocular motility testing, refractive error correction, orthoptic exercises, occlusive patching, and extraocular muscle surgery.
Effective communication among team members is vital. Regular meetings and consultations between team members are essential for sharing insights, discussing patient progress, and adjusting treatment plans collaboratively. Detailed, clearly written medical and orthoptic records should be available during clinic appointments and surgical admissions. Sharing all patient-ophthalmologist correspondences is crucial in maintaining open communication with community pediatricians.[91] Seamless care coordination is crucial to ensure patients receive comprehensive and consistent care.
Effective and transparent communication between clinicians and parents is also particularly paramount. Healthcare professionals should engage patients and their families in decision-making, impart information about the condition and available treatment choices, and attentively address their concerns. The interprofessional team collaboratively delivers comprehensive and patient-centered care to individuals with strabismus, leading to enhanced outcomes and improved quality of life.
Media
(Click Image to Enlarge)
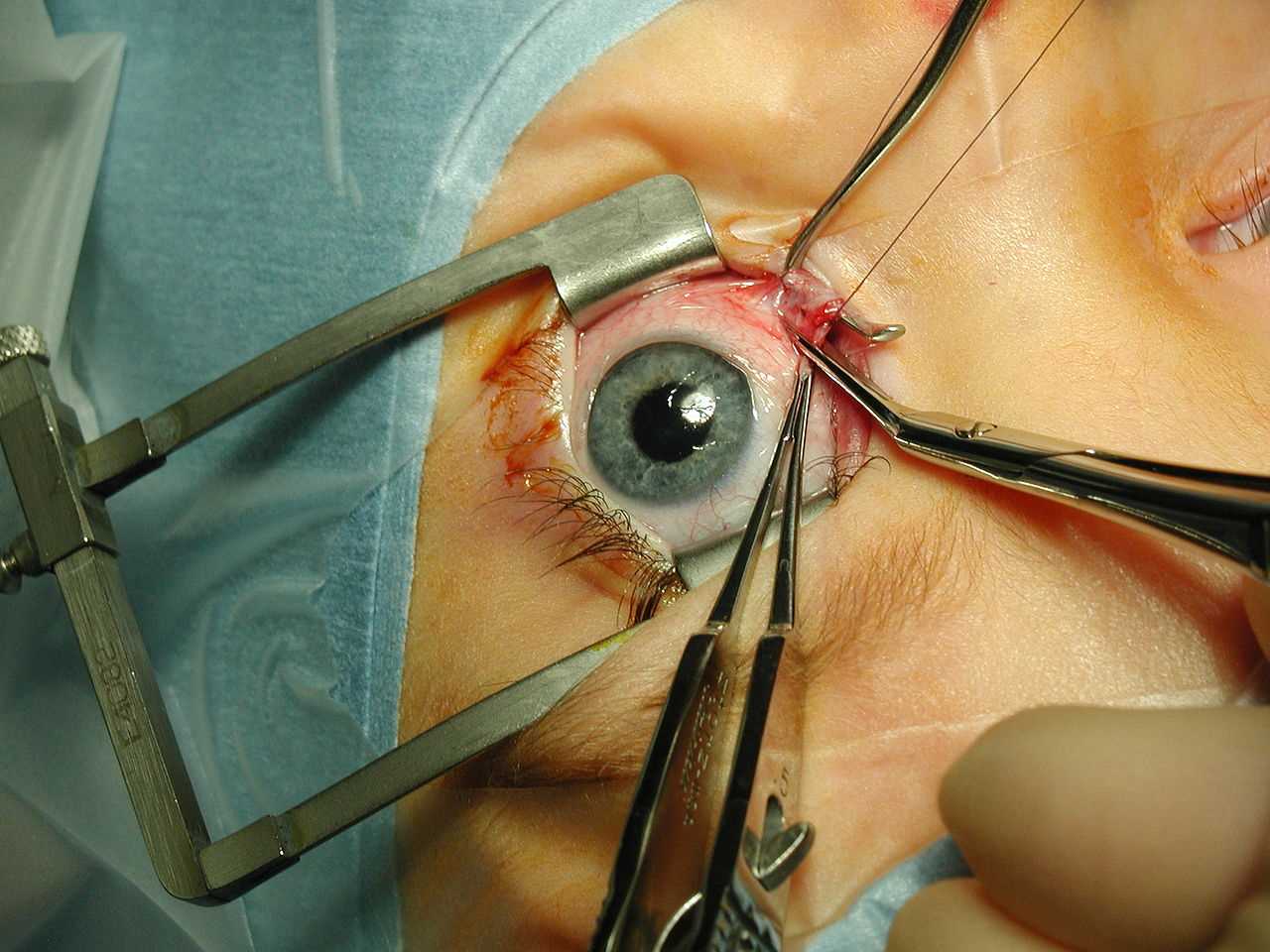
Strabismus Surgery. Medial rectus muscle being disinserted following pre-placement of polyglactin 910 sutures. A Castroviejo locking forceps grasps the superior pole of the muscle, while a Manson-Aebli scissors does the cutting. A Cook speculum is holding the eyelids.
Contributed by Wikimedia Commons (Public Domain)
(Click Image to Enlarge)

Strabismus Image courtesy S Bhimji MD
References
Helveston EM. Understanding, detecting, and managing strabismus. Community eye health. 2010 Mar:23(72):12-4 [PubMed PMID: 20523857]
Level 3 (low-level) evidenceClarke WN. Common types of strabismus. Paediatrics & child health. 1999 Nov:4(8):533-5 [PubMed PMID: 20213000]
Bui Quoc E, Milleret C. Origins of strabismus and loss of binocular vision. Frontiers in integrative neuroscience. 2014:8():71. doi: 10.3389/fnint.2014.00071. Epub 2014 Sep 25 [PubMed PMID: 25309358]
Qanat AS, Alsuheili A, Alzahrani AM, Faydhi AA, Albadri A, Alhibshi N. Assessment of Different Types of Strabismus Among Pediatric Patients in a Tertiary Hospital in Jeddah. Cureus. 2020 Dec 8:12(12):e11978. doi: 10.7759/cureus.11978. Epub 2020 Dec 8 [PubMed PMID: 33425550]
Rowe FJ, Noonan CP. Botulinum toxin for the treatment of strabismus. The Cochrane database of systematic reviews. 2017 Mar 2:3(3):CD006499. doi: 10.1002/14651858.CD006499.pub4. Epub 2017 Mar 2 [PubMed PMID: 28253424]
Level 1 (high-level) evidenceRyu WY, Lambert SR. Incidence of Strabismus and Amblyopia Among Children Initially Diagnosed With Pseudostrabismus Using the Optum Data Set. American journal of ophthalmology. 2020 Mar:211():98-104. doi: 10.1016/j.ajo.2019.10.036. Epub 2019 Nov 13 [PubMed PMID: 31730842]
Mooss VS, Kavitha V, Ravishankar HN, Heralgi MM, Aafreen S. Presence and development of strabismus in children with telecanthus, epicanthus and hypertelorism. Indian journal of ophthalmology. 2022 Oct:70(10):3618-3624. doi: 10.4103/ijo.IJO_776_22. Epub [PubMed PMID: 36190058]
Chen AH, Aziz A. Heterophoria in young adults with emmetropia and myopia. The Malaysian journal of medical sciences : MJMS. 2003 Jan:10(1):90-4 [PubMed PMID: 23365507]
Kim IG, Park JM, Lee SJ. Factors associated with the direction of ocular deviation in sensory horizontal strabismus and unilateral organic ocular problems. Korean journal of ophthalmology : KJO. 2012 Jun:26(3):199-202. doi: 10.3341/kjo.2012.26.3.199. Epub 2012 May 22 [PubMed PMID: 22670077]
Level 2 (mid-level) evidenceMcDermott CJ, Shaw PJ. Diagnosis and management of motor neurone disease. BMJ (Clinical research ed.). 2008 Mar 22:336(7645):658-62. doi: 10.1136/bmj.39493.511759.BE. Epub [PubMed PMID: 18356234]
Lueder GT. Orbital Causes of Incomitant Strabismus. Middle East African journal of ophthalmology. 2015 Jul-Sep:22(3):286-91. doi: 10.4103/0974-9233.159714. Epub [PubMed PMID: 26180465]
Khan AO. A Modern Approach to Incomitant Strabismus. Middle East African journal of ophthalmology. 2015 Jul-Sep:22(3):263-4. doi: 10.4103/0974-9233.159687. Epub [PubMed PMID: 26180461]
Koc F, Ozal H, Yasar H, Firat E. Resolution in partially accomodative esotropia during occlusion treatment for amblyopia. Eye (London, England). 2006 Mar:20(3):325-8 [PubMed PMID: 15933753]
Level 2 (mid-level) evidenceRoberts J, Rowland M. Refraction status and motility defects of persons 4-74 years. Vital and health statistics. Series 11, Data from the National Health Survey. 1978 Aug:(206):1-124 [PubMed PMID: 15807476]
Level 3 (low-level) evidenceMohney BG. Common forms of childhood esotropia. Ophthalmology. 2001 Apr:108(4):805-9 [PubMed PMID: 11297502]
Mohney BG. Common forms of childhood strabismus in an incidence cohort. American journal of ophthalmology. 2007 Sep:144(3):465-7 [PubMed PMID: 17765436]
Level 2 (mid-level) evidenceGovindan M, Mohney BG, Diehl NN, Burke JP. Incidence and types of childhood exotropia: a population-based study. Ophthalmology. 2005 Jan:112(1):104-8 [PubMed PMID: 15629828]
Level 2 (mid-level) evidenceCooper J. Intermittent exotropia of the divergence excess type. Journal of the American Optometric Association. 1977 Oct:48(10):1261-73 [PubMed PMID: 908827]
Ing MR, Pang SW. The racial distribution of strabismus. A statistical study. Hawaii medical journal. 1974 Jan:33(1):22-3 [PubMed PMID: 4811603]
Nusz KJ, Mohney BG, Diehl NN. Female predominance in intermittent exotropia. American journal of ophthalmology. 2005 Sep:140(3):546-7 [PubMed PMID: 16139014]
Level 2 (mid-level) evidenceLevi DM. Rethinking amblyopia 2020. Vision research. 2020 Nov:176():118-129. doi: 10.1016/j.visres.2020.07.014. Epub 2020 Aug 28 [PubMed PMID: 32866759]
Tyler AE, Hutton RS. Was Sherrington right about co-contractions? Brain research. 1986 Apr 2:370(1):171-5 [PubMed PMID: 3708319]
King WM. Binocular coordination of eye movements--Hering's Law of equal innervation or uniocular control? The European journal of neuroscience. 2011 Jun:33(11):2139-46. doi: 10.1111/j.1460-9568.2011.07695.x. Epub [PubMed PMID: 21645107]
Level 3 (low-level) evidenceAl-Falki Y, Al-Shraim M, Alsabaani NA, Eid RA, Radad K. Ultrastructural changes of extraocular muscles in strabismus patients. Ultrastructural pathology. 2019:43(4-5):145-153. doi: 10.1080/01913123.2019.1671927. Epub 2019 Sep 30 [PubMed PMID: 31570030]
Wiggins RE, von Noorden GK. Monocular eye closure in sunlight. Journal of pediatric ophthalmology and strabismus. 1990 Jan-Feb:27(1):16-20; discussion 21-2 [PubMed PMID: 2324913]
Ring J. History of Allergy: Clinical Descriptions, Pathophysiology, and Treatment. Handbook of experimental pharmacology. 2022:268():3-19. doi: 10.1007/164_2021_509. Epub [PubMed PMID: 34424388]
Pensiero S, Diplotti L, Presotto M, Ronfani L, Barbi E. Essential Infantile Esotropia: A Course of Treatment From Our Experience. Frontiers in pediatrics. 2021:9():695841. doi: 10.3389/fped.2021.695841. Epub 2021 Jul 23 [PubMed PMID: 34368027]
Lembo A, Serafino M, Strologo MD, Saunders RA, Trivedi RH, Villani E, Nucci P. Accommodative esotropia: the state of the art. International ophthalmology. 2019 Feb:39(2):497-505. doi: 10.1007/s10792-018-0821-6. Epub 2018 Jan 13 [PubMed PMID: 29332227]
Houston CA, Cleary M, Dutton GN, McFadzean RM. Clinical characteristics of microtropia--is microtropia a fixed phenomenon? The British journal of ophthalmology. 1998 Mar:82(3):219-24 [PubMed PMID: 9602615]
Kaur K, Gurnani B. Intermittent Exotropia. StatPearls. 2024 Jan:(): [PubMed PMID: 34662028]
Mravicic I, Gulic MP, Barisic A, Biscevic A, Pjano MA, Pidro A. Different Surgical Approaches for Treatment of Dissociated Vertical Deviation (DVD). Medical archives (Sarajevo, Bosnia and Herzegovina). 2019 Dec:73(6):386-390. doi: 10.5455/medarh.2019.73.386-390. Epub [PubMed PMID: 32082005]
Bagheri A, Sahebghalam R, Abrishami M. Double elevator palsy, subtypes and outcomes of surgery. Journal of ophthalmic & vision research. 2008 Apr:3(2):108-13 [PubMed PMID: 23479532]
Gantz L, Millodot M, Roth GL. Analysis of Alphabet Patterns of Deviations Found in Patients Without Strabismus in Primary Position. Clinical optometry. 2020:12():49-56. doi: 10.2147/OPTO.S197783. Epub 2020 Mar 20 [PubMed PMID: 32256138]
Kekunnaya R, Negalur M. Duane retraction syndrome: causes, effects and management strategies. Clinical ophthalmology (Auckland, N.Z.). 2017:11():1917-1930. doi: 10.2147/OPTH.S127481. Epub 2017 Oct 30 [PubMed PMID: 29133973]
Koc AA, Aygit ED, Inal A, Ocak B, Gurez C, Ahmet S, Duman B, Gokyigit B. Brown Syndrome: Features and Long-term Results of Management. Beyoglu eye journal. 2021:6(3):223-228. doi: 10.14744/bej.2021.35693. Epub 2021 Sep 27 [PubMed PMID: 35005520]
Picciolini O, Porro M, Cattaneo E, Castelletti S, Masera G, Mosca F, Bedeschi MF. Moebius syndrome: clinical features, diagnosis, management and early intervention. Italian journal of pediatrics. 2016 Jun 3:42(1):56. doi: 10.1186/s13052-016-0256-5. Epub 2016 Jun 3 [PubMed PMID: 27260152]
Kanazawa T, Hino U, Kuramae T, Ishihara M. Idiopathic unilateral oculomotor nerve palsy: A case report. Heliyon. 2020 Dec:6(12):e05651. doi: 10.1016/j.heliyon.2020.e05651. Epub 2020 Dec 3 [PubMed PMID: 33305057]
Level 3 (low-level) evidenceAzarmina M, Azarmina H. The six syndromes of the sixth cranial nerve. Journal of ophthalmic & vision research. 2013 Apr:8(2):160-71 [PubMed PMID: 23943691]
Bixenman WW. Diagnosis of superior oblique palsy. Journal of clinical neuro-ophthalmology. 1981 Sep:1(3):199-208 [PubMed PMID: 6213662]
Wong AM. Understanding skew deviation and a new clinical test to differentiate it from trochlear nerve palsy. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2010 Feb:14(1):61-7. doi: 10.1016/j.jaapos.2009.11.019. Epub [PubMed PMID: 20227626]
Level 3 (low-level) evidenceFulton AB, Hansen RM, Manning KA. Measuring visual acuity in infants. Survey of ophthalmology. 1981 Mar-Apr:25(5):325-32 [PubMed PMID: 7221878]
Level 3 (low-level) evidenceSalley B, Brady NC, Hoffman L, Fleming K. Preverbal Communication Complexity in Infants. Infancy : the official journal of the International Society on Infant Studies. 2020 Jan-Feb:25(1):4-21. doi: 10.1111/infa.12318. Epub 2019 Nov 25 [PubMed PMID: 32132879]
Salati R, Schiavulli O, Giammari G, Borgatti R. Checklist for the evaluation of low vision in uncooperative patients. Journal of pediatric ophthalmology and strabismus. 2001 Mar-Apr:38(2):90-4 [PubMed PMID: 11310713]
Paul CM, Sathyan S. Comparison of the efficacy of Lea Symbol chart and Sheridan Gardiner chart for preschool vision screening. Indian journal of ophthalmology. 2018 Jul:66(7):924-928. doi: 10.4103/ijo.IJO_1078_17. Epub [PubMed PMID: 29941732]
Gautam Adhikari P, Shah S, Bhatta N, Mandal P, Sharma Paudel B, Pokhrel A, Koirala B, Shah CP. Stereoacuity among Undergraduate Medical and Nursing Students at a Tertiary Care Hospital: A Descriptive Cross-sectional Study. JNMA; journal of the Nepal Medical Association. 2022 Jan 15:60(245):54-58. doi: 10.31729/jnma.7053. Epub 2022 Jan 15 [PubMed PMID: 35199674]
Level 2 (mid-level) evidenceKraft SP, O'Donoghue EP, Roarty JD. Improvement of compensatory head postures after strabismus surgery. Ophthalmology. 1992 Aug:99(8):1301-8 [PubMed PMID: 1513584]
Level 2 (mid-level) evidenceMutti DO, Jones LA, Moeschberger ML, Zadnik K. AC/A ratio, age, and refractive error in children. Investigative ophthalmology & visual science. 2000 Aug:41(9):2469-78 [PubMed PMID: 10937556]
Garcia SSS, Santiago APD, Directo PMC. Evaluation of a Hirschberg Test-Based Application for Measuring Ocular Alignment and Detecting Strabismus. Current eye research. 2021 Nov:46(11):1768-1776. doi: 10.1080/02713683.2021.1916038. Epub 2021 Apr 19 [PubMed PMID: 33856941]
Sethi H, Naik M, Joshi M. Modified Krimsky test for irregular scarred corneas. International ophthalmology. 2017 Oct:37(5):1243-1245. doi: 10.1007/s10792-016-0392-3. Epub 2016 Nov 8 [PubMed PMID: 27826935]
Mestre C, Otero C, Díaz-Doutón F, Gautier J, Pujol J. An automated and objective cover test to measure heterophoria. PloS one. 2018:13(11):e0206674. doi: 10.1371/journal.pone.0206674. Epub 2018 Nov 1 [PubMed PMID: 30383846]
Hull S, Tailor V, Balduzzi S, Rahi J, Schmucker C, Virgili G, Dahlmann-Noor A. Tests for detecting strabismus in children aged 1 to 6 years in the community. The Cochrane database of systematic reviews. 2017 Nov 6:11(11):CD011221. doi: 10.1002/14651858.CD011221.pub2. Epub 2017 Nov 6 [PubMed PMID: 29105728]
Level 1 (high-level) evidencePediatric Eye Disease Investigator Group. Interobserver reliability of the prism and alternate cover test in children with esotropia. Archives of ophthalmology (Chicago, Ill. : 1960). 2009 Jan:127(1):59-65. doi: 10.1001/archophthalmol.2008.548. Epub [PubMed PMID: 19139339]
Holmes JM, Leske DA, Hohberger GG. Defining real change in prism-cover test measurements. American journal of ophthalmology. 2008 Feb:145(2):381-5 [PubMed PMID: 18045567]
Pointer JS. An enhancement to the Maddox Wing test for the reliable measurement of horizontal heterophoria. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2005 Sep:25(5):446-51 [PubMed PMID: 16101952]
Dolman P. The Maddox Rod Screen Test. Transactions of the American Ophthalmological Society. 1919:17():235-49 [PubMed PMID: 16692471]
Honglertnapakul W, Praneeprachachon P, Pukrushpan P. Normal Range of Ocular Ductions in Various Age Brackets by Prism Shifting Light-Reflex Test. Journal of binocular vision and ocular motility. 2020 Apr-Jun:70(2):47-52. doi: 10.1080/2576117X.2019.1711354. Epub 2020 Jan 17 [PubMed PMID: 31951789]
Jarwick LCJ, Taylor K, Connor AJ, Fieldsend CS. Postoperative diplopia test-repeatability and prediction of surgical outcomes. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2022 Oct:26(5):252.e1-252.e5. doi: 10.1016/j.jaapos.2022.07.011. Epub 2022 Sep 23 [PubMed PMID: 36156298]
Level 2 (mid-level) evidenceKouri AS, Bessant DA, Adams GG, Sloper JJ, Lee JP. Quantitative changes in the field of binocular single vision following a fadenoperation to a vertical rectus muscle. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2002 Oct:6(5):294-9 [PubMed PMID: 12381988]
Roper-Hall G. The hess screen test. The American orthoptic journal. 2006:56():166-74. doi: 10.3368/aoj.56.1.166. Epub [PubMed PMID: 21149145]
Murray AD. An Approach to Some Aspects of Strabismus from Ocular and Orbital Trauma. Middle East African journal of ophthalmology. 2015 Jul-Sep:22(3):312-9. doi: 10.4103/0974-9233.159732. Epub [PubMed PMID: 26180469]
Chang JW. Refractive error change and vision improvement in moderate to severe hyperopic amblyopia after spectacle correction: Restarting the emmetropization process? PloS one. 2017:12(4):e0175780. doi: 10.1371/journal.pone.0175780. Epub 2017 Apr 19 [PubMed PMID: 28423020]
Kim S, Yang HK, Hwang JM. Surgical outcomes of unilateral recession and resection in intermittent exotropia according to forced duction test results. PloS one. 2018:13(7):e0200741. doi: 10.1371/journal.pone.0200741. Epub 2018 Jul 26 [PubMed PMID: 30048470]
Lee JE, Yang HK, Kim JH, Hwang JM. Diagnostic Utility of the Three-Step Test According to the Presence of the Trochlear Nerve in Superior Oblique Palsy. Journal of clinical neurology (Seoul, Korea). 2018 Jan:14(1):66-72. doi: 10.3988/jcn.2018.14.1.66. Epub [PubMed PMID: 29629542]
Corr RH. Fundoscopy in the smartphone age: current ophthalmoscopy methods in neurology. Arquivos de neuro-psiquiatria. 2023 May:81(5):502-509. doi: 10.1055/s-0043-1763489. Epub 2023 May 31 [PubMed PMID: 37257471]
Frantz KA, Cotter SA, Wick B. Re-evaluation of the four prism diopter base-out test. Optometry and vision science : official publication of the American Academy of Optometry. 1992 Oct:69(10):777-86 [PubMed PMID: 1436999]
Herzau V, Schoser G. [The value of the prism adaptation test in determining the degree of squint surgery]. Der Ophthalmologe : Zeitschrift der Deutschen Ophthalmologischen Gesellschaft. 1993 Feb:90(1):11-6 [PubMed PMID: 8443441]
Horwood A. Neonatal ocular misalignments reflect vergence development but rarely become esotropia. The British journal of ophthalmology. 2003 Sep:87(9):1146-50 [PubMed PMID: 12928285]
Lavrich JB. Intermittent exotropia: continued controversies and current management. Current opinion in ophthalmology. 2015 Jul:26(5):375-81. doi: 10.1097/ICU.0000000000000188. Epub [PubMed PMID: 26204476]
Level 3 (low-level) evidenceWriting Committee for the Pediatric Eye Disease Investigator Group, Cotter SA, Foster NC, Holmes JM, Melia BM, Wallace DK, Repka MX, Tamkins SM, Kraker RT, Beck RW, Hoover DL, Crouch ER 3rd, Miller AM, Morse CL, Suh DW. Optical treatment of strabismic and combined strabismic-anisometropic amblyopia. Ophthalmology. 2012 Jan:119(1):150-8. doi: 10.1016/j.ophtha.2011.06.043. Epub 2011 Sep 29 [PubMed PMID: 21959371]
Level 2 (mid-level) evidenceRepka MX, Kraker RT, Holmes JM, Summers AI, Glaser SR, Barnhardt CN, Tien DR, Pediatric Eye Disease Investigator Group. Atropine vs patching for treatment of moderate amblyopia: follow-up at 15 years of age of a randomized clinical trial. JAMA ophthalmology. 2014 Jul:132(7):799-805. doi: 10.1001/jamaophthalmol.2014.392. Epub [PubMed PMID: 24789375]
Level 1 (high-level) evidenceOsborne DC, Greenhalgh KM, Evans MJE, Self JE. Atropine Penalization Versus Occlusion Therapies for Unilateral Amblyopia after the Critical Period of Visual Development: A Systematic Review. Ophthalmology and therapy. 2018 Dec:7(2):323-332. doi: 10.1007/s40123-018-0151-9. Epub 2018 Oct 16 [PubMed PMID: 30328078]
Level 1 (high-level) evidenceGray LS. The prescribing of prisms in clinical practice. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2008 May:246(5):627-9. doi: 10.1007/s00417-008-0799-2. Epub 2008 Apr 1 [PubMed PMID: 18379815]
Hiatt RL, Ringer C, Cope-Troupe C. Miotics vs glasses in esodeviation. Journal of pediatric ophthalmology and strabismus. 1979 Jul-Aug:16(4):213-7 [PubMed PMID: 490272]
Ozkan SB, Topaloğlu A, Aydin S. The role of botulinum toxin A in augmentation of the effect of recession and/or resection surgery. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2006 Apr:10(2):124-7 [PubMed PMID: 16678746]
Jampolsky A, von Noorden GK, Spiritus M. Unnecessary surgery in fully refractive accommodative esotropia. International ophthalmology. 1992 Mar:16(2):129-30; discussion 130-1 [PubMed PMID: 1587696]
Ing MR, Okino LM. Outcome study of stereopsis in relation to duration of misalignment in congenital esotropia. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2002 Feb:6(1):3-8 [PubMed PMID: 11907472]
Leske DA, Holmes JM. Maximum angle of horizontal strabismus consistent with true stereopsis. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2004 Feb:8(1):28-34 [PubMed PMID: 14970796]
Kampanartsanyakorn S, Surachatkumtonekul T, Dulayajinda D, Jumroendararasmee M, Tongsae S. The outcomes of horizontal strabismus surgery and influencing factors of the surgical success. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2005 Nov:88 Suppl 9():S94-9 [PubMed PMID: 16681059]
Level 2 (mid-level) evidenceRepka MX, Lum F, Burugapalli B. Strabismus, Strabismus Surgery, and Reoperation Rate in the United States: Analysis from the IRIS Registry. Ophthalmology. 2018 Oct:125(10):1646-1653. doi: 10.1016/j.ophtha.2018.04.024. Epub 2018 May 18 [PubMed PMID: 29779683]
Kaur K, Gurnani B. Esotropia. StatPearls. 2024 Jan:(): [PubMed PMID: 35201735]
Kim WK, Kang SY, Rhiu S, Chung SA, Lee JB. The analysis of AC/A ratio in nonrefractive accommodative esotropia treated with bifocal glasses. Korean journal of ophthalmology : KJO. 2012 Feb:26(1):39-44. doi: 10.3341/kjo.2012.26.1.39. Epub 2012 Jan 14 [PubMed PMID: 22323884]
Level 2 (mid-level) evidenceSuh SY, Kim MJ, Choi J, Kim SJ. Outcomes of surgery in children with early-onset exotropia. Eye (London, England). 2013 Jul:27(7):836-40. doi: 10.1038/eye.2013.75. Epub 2013 Apr 26 [PubMed PMID: 23619215]
Level 2 (mid-level) evidenceHatt SR, Gnanaraj L. Interventions for intermittent exotropia. The Cochrane database of systematic reviews. 2013 May 31:2013(5):CD003737. doi: 10.1002/14651858.CD003737.pub3. Epub 2013 May 31 [PubMed PMID: 23728647]
Level 1 (high-level) evidenceLou DH, Xu YS, Li YM. Sensory exotropia subsequent to senile cataract. Journal of Zhejiang University. Science. B. 2005 Dec:6(12):1220-2 [PubMed PMID: 16358383]
Kekunnaya R, Mendonca T, Sachdeva V. Pattern strabismus and torsion needs special surgical attention. Eye (London, England). 2015 Feb:29(2):184-90. doi: 10.1038/eye.2014.270. Epub 2014 Nov 21 [PubMed PMID: 25412718]
Nelson LB, Wagner RS, Simon JW, Harley RD. Congenital esotropia. Survey of ophthalmology. 1987 May-Jun:31(6):363-83 [PubMed PMID: 3303394]
Level 3 (low-level) evidenceMulvihill A, MacCann A, Flitcroft I, O'Keefe M. Outcome in refractive accommodative esotropia. The British journal of ophthalmology. 2000 Jul:84(7):746-9 [PubMed PMID: 10873987]
Akhtar A, Macfarlane RJ, Waseem M. Pre-operative assessment and post-operative care in elective shoulder surgery. The open orthopaedics journal. 2013:7():316-22. doi: 10.2174/1874325001307010316. Epub 2013 Sep 6 [PubMed PMID: 24093051]
Althiabi S, AlDarrab A, Alenezi SH, Alharbi BA, Aljbreen AJ, Alsalamah GF, Alotaibi RA, Almutairi FA, Albadrani NA. Psychological and Social Challenges Parents of Children With Strabismus Face in Qassim Region, Saudi Arabia: A Cross-Sectional Study. Cureus. 2023 Mar:15(3):e36920. doi: 10.7759/cureus.36920. Epub 2023 Mar 30 [PubMed PMID: 37128539]
Level 2 (mid-level) evidenceSaxena R, Singh D, Jethani J, Sharma P, Sinha R, Sharma N, Sachdev Writing Committee MS, Prepared in Association with the AIOS Pediatric and. Pediatric ophthalmology, strabismus and neuro-ophthalmology practice in the COVID-19 era: All India Ophthalmological Society guidelines. Indian journal of ophthalmology. 2020 Jul:68(7):1300-1305. doi: 10.4103/ijo.IJO_1789_20. Epub [PubMed PMID: 32587154]
PRANGEN AD. The treatment of strabismus in children. Medical world. 1945 Dec:63():551 [PubMed PMID: 21007425]