Introduction
The spinal cord is a tubular structure composed of nervous tissue that extends from the brainstem and continues distally before tapering at the lower thoracic/upper lumbar region as the conus medullaris. The spinal cord is anchored distally by the filum terminale, a fibrous extension of the pia mater anchoring the spinal cord to the coccyx.[1] Protecting the spinal cord is the surrounding cerebrospinal fluid (CSF), supportive soft tissue membranes and meninges, and the osseous vertebral column.[2] Basic knowledge of the spinal cord and spinal column structure and function is essential for healthcare providers as the recognition of characteristic clinical signs and symptoms is imperative for the appropriate treatment of patients presenting with a wide range of clinical symptoms.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Meninges and Spaces
- Epidural space - fatty space between the bony framework of the spinal vertebral column and the thick dura mater surrounding the spinal cord. It contains adipose tissue and blood vessels.
- Dura mater - Thick outermost covering (meninges) of the spinal cord, extending down to the level of the S2 vertebra.
- Arachnoid mater - The middle covering of the spinal cord
- Subarachnoid space - Space between the arachnoid mater and the innermost covering of the spinal cord. It contains Cerebrospinal fluid.
- Pia mater - The innermost covering of the spinal cord, intimately adhering to its surface, stabilizes the spinal cord through lateral extensions of the pia called the denticulate ligaments, extending between the ventral and dorsal roots unto the dura mater.
Spinal cord
- The length is about 45 cm in men and 43 cm in women[1]
- The anatomic course originates in the brainstem before coursing through the foramen magnum. The spinal cord continues distally through the cervical and thoracic regions of the spinal column before terminating as a tapered structure known as the conus medullaris
- The spinal cord proper terminates at the L1-L2 vertebral level and is anchored distally via the filum terminale, representing an extension of the pia mater with fibrous attachments to the coccyx
- The spinal cord comprises 5 segments, cervical, thoracic, lumbar, sacral, and coccygeal
- Long, cylindrical structure with varying levels of thickness/width depending on the corresponding vertebral levels
- 31 total nerve root segments
- 8 cervical
- 12 thoracic
- 5 lumbar
- 5 sacral
- 1 coccygeal
- Cord width ranges from 0.64 to 0.83 cm in the thoracic region to 1.27 to 1.33 cm in the cervical and lumbar regions.
- A 2016 systematic review of the literature demonstrated that, on average, the largest transverse diameter corresponded to the C5 neuronal segment (1.33 +/- 0.22 cm), and the smallest transverse diameter, on average, corresponding to the T8 segment (0.83 +/- 0.21 cm)[3]
- Enlarged regions of gray matter correspond to nerve root distribution to the upper and lower extremities.
- A cross-sectional view of the spinal cord shows its organization into the gray and white matter. The anterior aspect of the cord is identifiable with the presence of an anterior median fissure. The gray matter is organized into an H- shaped body of cell bodies. The anterior horn comprises motor nuclei, while the posterior horn comprises sensory nuclei. The surrounding white matter is organized into anterior, posterior, and lateral columns (funiculi), from neuronal axons organized into tracts that convey neural messages back and forth to the CNS (the ascending and descending tracts). The anterolateral columns carry temperature and pain information, while the dorsal column communicates the sense of touch, proprioception, and vibration. The cervical and thoracic spinal segments present an intermediolateral gray horn which gives off preganglionic sympathetic fibers onto the sympathetic trunk on both sides of the spinal cord.
- The spinal cord's central canal is an extension of the 4th ventricle. It contains CSF; surrounding it is the gray commissure and the anterior white commissure. Decussation of the tracts of the white columns occurs at the anterior white commissure.
Embryology
After the third week of development, a fusion of the neural folds into a tube (neurulation) occurs; the neural tube then closes completely at day 28 and forms the brain and the spinal cord.
The caudal neural tube's cross-sectional view initially appears diamond-shaped, lined by neuroepithelial cells, which divide and multiply into neuroblasts that populate surrounding areas called the mantle zone, eventually forming the gray matter. Divided neuroepithelial cells now form the ependymal lining of the central spinal canal with roles in CSF production.
The mantle zone differentiates into - basal plate, alar plate, and intermediolateral plate. More lateral parts form into the marginal zone, which becomes the white mater with ascending and descending myelinated fibers.
The basal plates differentiate into the anterior or ventral gray horn. Multipolar neurons in the anterior horn are first-order neurons and give off motor fibers that exit the spinal segments and become myelinated by Schwann cells (derivative of neural crest cells).
The alar plates differentiate into the posterior or dorsal gray horn. They comprise second-order pseudo-unipolar neurons, which receive sensory communication from first-order neurons derived from neural crest-derived dorsal ganglia.
The intermediolateral plates in cervical and thoracic regions are populated by pre-ganglion neurons, which give off fibers exiting ventrally onto the sympathetic trunk.
Blood Supply and Lymphatics
- Anterior spinal artery - branch of the vertebral artery, supplies the anterior 2/3 of the spinal segment[4]
- Left and right posterior spinal arteries - The pair posterior branches of the vertebral artery supply the posterior third of the spinal segment
Radiculo-medullary branches from the anterior and posterior spinal arteries and the costocervical trunk anastomose supply the cervical region of the spinal cord. The thoracolumbar segments of the spinal cord receive extra arterial blood supply through radiculo-medullary branches of segmental arteries from the aorta; of note is the great radicular artery called the Adamkiewicz artery.[4] It has a variable origin arising anywhere between T9 and L5 vertebra.
Nerves
There are 31 spinal nerve pairs (mixed) that arise from the intervertebral foramen on both sides of the vertebral column.
- 8 Cervical nerves - C1 - C7 nerves arising from above corresponding cervical vertebra except for C8, which exits from between C7 and T1 Vertebrae
- 12 Thoracic nerves
- 5 Lumbar nerves
- 5 Sacral nerves
- 1 Coccygeal segment
Nerves from the lower spinal segment exit terminal to the conus medullaris and form the cauda equina.
Ventral spinal nerve roots - make up the motor component of the spinal innervation with rootlets arising from the anterior horn of the spinal segment, sending motor impulses to muscles and joints, etc.
Dorsal spinal nerve roots - make up the sensory component, with the dorsal ganglia sending sensory impulses via nerve rootlets to the posterior horn of spinal segments.
Surgical Considerations
- Placing an incision on the surface of the spinal cord is known as myelotomy.
- A posterior median sulcus approach - for most intramedullary gliomas and ependymomas
- Lateral myelotomy - for vascular tumors such as hemangioblastoma or cavernous malformation
- Limited midline myelotomy - for intractable visceral pain
Cordotomy[7]
- Cervical cordotomy - the nociceptive pathways in the lateral spinothalamic tract (anterolateral column) are surgically destroyed at the level of C1-C2. This is done for pain relief in unilateral malignancies and lower limb pathologies.
Clinical Significance
Spinal cord disorders, injuries (SCIs), or syndromes may include (but are not limited to)[8][9][10]
- Traumatic (ground-level falls in the elderly, high-energy motor vehicle accidents in any age group)
- The incidence and prevalence of traumatic SCI in the United States are higher compared to rates reported in the literature for other countries worldwide[11][12]
- The average age at clinical presentation continues to increase, corresponding to the aging of the general population[11]
- Heightened clinical suspicion should be given to vertebral compression fractures, which can occur spontaneously (i.e., in the absence of trauma)[13][14][15][16][17][18]
- Infection[19]
- Tumors/malignancy (including metastatic disease)[20][21][22]
- Disc herniations[23][24]
- Spinal stenosis/degenerative conditions/facet arthropathy[23][25][26][27][28]
- Syringomyelia[29][30]
In general, the extent of disability depends on the level of injury and the underlying degree of severity of the corresponding clinical pathology. For example, injuries at the levels of the cervical segment affect both upper and lower limbs, while lesions from thoracic segments downwards affect the lower limb.[31]
Spinal Cord Injury (SCI) Patterns
- Descriptive
- Tetraplegia
- Cervical spine injury resulting in impaired arm/trunk/leg/pelvic organ function
- Paraplegia
- Thoracic/lumbar/sacral spinal injury leading to impaired trunk/leg/pelvic organ function
- Preserved arm function
- Complete injuries
- By definition, a complete SCI yields no sparing of the motor or sensory function below the injured level.
- The patient must have already recovered from the acute phase of spinal shock (usually 48 hours from presentation)
- Spinal shock: by definition, the temporary (typically 48 hours) loss of all spinal cord function (including reflex activity) below the level of injury
- Absent bulbocavernosus reflex
- Flaccid paralysis
- Bradycardia/hypotension
- By definition, a complete SCI yields no sparing of the motor or sensory function below the injured level.
- Tetraplegia
- Spina bifida - Neural tube defect in which the neural tube does not completely close, leaving a dorsal defect. Folate deficiency in early pregnancy is a risk factor.[32] The severity of symptoms depends on the extent of the defect; myelomeningocele is the most severe variant with the spinal cord, meninges both exposed. Other variants include meningocele, which exposes only the meninges, and spina bifida occulta, which is the mildest variant. Symptoms include loss of lower limb sensations, lower limb weakness, urinary incontinence, bowel incontinence
Incomplete Spinal Cord Injuries (SCIs)
- Central cord syndrome[8]
- Most common incomplete SCI
- Pathophysiology: central gray matter injury
- Mechanism(s): hyperextension (i.e., from a fall) in a patient with underlying cervical spinal canal stenosis
- Clinical presentation:
- Upper extremity loss of motor function (lower extremity motor function no affected/minimally affected)
- Sensory sparing variable
- Prognosis: Good
- Anterior cord syndrome[31]
- Second most common incomplete SCI
- Pathophysiology: injuries occur secondary to direct compression to the anterior spinal cord (e.g., hyperflexion injuries, anterior spinal artery occlusion, or disc prolapse)
- Mechanism(s): hyperflexion injuries, anterior spinal artery occlusion, disc prolapse
- Clinical presentation:
- Loss of motor, pain, and temperature reception below the level of injury
- Preserved dorsal column function (i.e., proprioception, vibration sensation, and deep pressure sensation)
- Prognosis: Poor (for motor recovery specifically)
- Posterior cord syndrome[33]
- Very rare/least common incomplete SCI pattern of injury
- Pathophysiology: injury to the dorsal column
- Mechanism(s):
- Subacute combined degeneration
- Tabes dorsalis (i.e., secondary to syphilis)
- Multiple sclerosis
- Vascular malformations (arterio-venous malformation - AVM)
- Malignancy (e.g., compressive extramedullary tumors)
- Degenerative conditions (e.g., spondylosis)
- Clinical presentation:
- Loss of proprioception, vibration, and deep pressure sensation below the level of injury
- Preserved ambulatory function
- Patients will complain of difficulty balancing in the dark or with their eyes closed
- Classic exam consistent with a positive Romberg sign
- Prognosis: Preserved ambulatory function; dorsal column recovery unpredictable
- Spinal cord hemisection/hemicord (Brown-Sequard syndrome)[34]
- Rare (2% to 4% of SCIs)[35]
- Pathophysiology: trauma to one side of the spinal cord (in cross-sectional reference)
- Mechanism(s):
- Penetrating trauma (knife, gunshot wound)
- Clinical presentation:
- Ipsilateral loss of motor and proprioception (directly below the level of injury)
- Contralateral loss of pain/temperature
- Classically the contralateral pain/temperature loss occurs one to two levels below the level of injury)
- Prognosis: 90% recover ambulatory function
- Cauda equina syndrome[33][36]
- Pathophysiology: Injury to (only) the nerve roots of the cauda equina itself (i.e., spares the spinal cord itself)
- Mechanism(s):
- Disc herniations
- Burst fractures (e.g., associated hematoma from trauma)
- Clinical presentation:
- Bilateral buttock/lower extremity pain
- Bowel/bladder dysfunction (urinary retention)
- Saddle anesthesia
- Loss of lower extremity motor/sensory function
- Differentiated from conus medullaris syndrome in that findings are asymmetrical, as opposed to symmetrical (i.e., conus medullaris motor symptoms are symmetrical on presentation)
- Prognosis: surgical decompression within the first 48 hours appears to yield improved overall outcomes (although the overall prognosis remains guarded)
- Conus medullaris syndrome[33]
- Often confused with cauda equina syndrome, although this must be recognized as a separate clinical entity.
- Pathophysiology: injury to the spinal cord at the L1-L2 level
- Mechanism(s):
- Direct spinal trauma to the thoracolumbar junction[33]
- Clinical presentation:
- Saddle anesthesia
- Bowel/bladder dysfunction (often presents with dysfunction more acutely compared to cauda equina, which can evolve over a variable period of time prior to the patient's presentation)
- Classically presents with mild, symmetrical motor symptoms (often mixed upper and lower motor neuron syndromes)
- can present with both spasticity and flaccid paresis
- hyperreflexia and/or hyporeflexia
- Prognosis: guarded
Other Issues
Epidural anesthesia - Injecting anesthetic medications into the epidural space, using a catheter, and multiple dosing is achievable.
Subarachnoid anesthesia - anesthetic medications delivered into the subarachnoid space, usually between L3 and L5.[37]
Lumbar puncture - Tiny needle through L3 and L5 to obtain CSF from the subarachnoid space for biochemical and microbiology investigations.
Media
(Click Image to Enlarge)
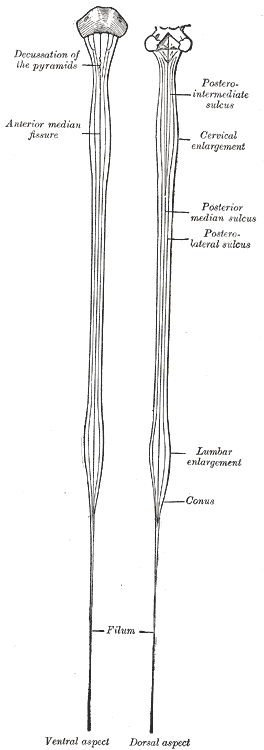
Spinal Cord, Neurology, Medulla Spinalis; Ventral and Dorsal aspect, Decussation of the pyramids, Posterior intermediate sulcus, Conus
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
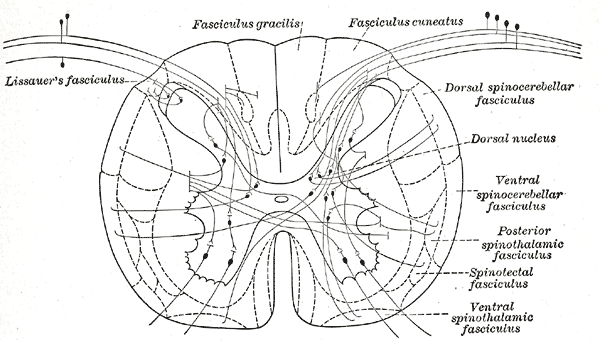
Structures of the Gray matter, Spinal Cord, Connections of afferent (sensory) fibers; posterior root with the efferent fibers from the ventral column and with the various long ascending fasciculi
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Bican O, Minagar A, Pruitt AA. The spinal cord: a review of functional neuroanatomy. Neurologic clinics. 2013 Feb:31(1):1-18. doi: 10.1016/j.ncl.2012.09.009. Epub [PubMed PMID: 23186894]
Huff T, Tadi P, Weisbrod LJ, Varacallo M. Neuroanatomy, Cerebrospinal Fluid. StatPearls. 2023 Jan:(): [PubMed PMID: 29262203]
Frostell A,Hakim R,Thelin EP,Mattsson P,Svensson M, A Review of the Segmental Diameter of the Healthy Human Spinal Cord. Frontiers in neurology. 2016 [PubMed PMID: 28066322]
Lindeire S, Hauser JM. Anatomy, Back, Artery Of Adamkiewicz. StatPearls. 2023 Jan:(): [PubMed PMID: 30422566]
Takami T, Naito K, Yamagata T, Ohata K. Surgical management of spinal intramedullary tumors: radical and safe strategy for benign tumors. Neurologia medico-chirurgica. 2015:55(4):317-27. doi: 10.2176/nmc.ra.2014-0344. Epub 2015 Mar 23 [PubMed PMID: 25797779]
Vedantam A, Koyyalagunta D, Bruel BM, Dougherty PM, Viswanathan A. Limited Midline Myelotomy for Intractable Visceral Pain: Surgical Techniques and Outcomes. Neurosurgery. 2018 Oct 1:83(4):783-789. doi: 10.1093/neuros/nyx549. Epub [PubMed PMID: 29165656]
Teoli D,An J, Cordotomy . 2020 Jan [PubMed PMID: 30571067]
Jeanmonod R,Varacallo M, Geriatric Cervical Spine Injury . 2018 Jan [PubMed PMID: 29262191]
Toney-Butler TJ,Varacallo M, Motor Vehicle Collision . 2018 Jan [PubMed PMID: 28722984]
Varacallo M, Davis DD, Pizzutillo P. Osteoporosis in Spinal Cord Injuries. StatPearls. 2023 Jan:(): [PubMed PMID: 30252365]
Devivo MJ. Epidemiology of traumatic spinal cord injury: trends and future implications. Spinal cord. 2012 May:50(5):365-72. doi: 10.1038/sc.2011.178. Epub 2012 Jan 24 [PubMed PMID: 22270188]
Level 2 (mid-level) evidenceChen Y, He Y, DeVivo MJ. Changing Demographics and Injury Profile of New Traumatic Spinal Cord Injuries in the United States, 1972-2014. Archives of physical medicine and rehabilitation. 2016 Oct:97(10):1610-9. doi: 10.1016/j.apmr.2016.03.017. Epub 2016 Apr 22 [PubMed PMID: 27109331]
Varacallo M,Pizzutillo P, Osteopenia . 2018 Jan [PubMed PMID: 29763053]
Porter JL, Varacallo M. Osteoporosis. StatPearls. 2023 Jan:(): [PubMed PMID: 28722930]
Varacallo MA, Fox EJ. Osteoporosis and its complications. The Medical clinics of North America. 2014 Jul:98(4):817-31, xii-xiii. doi: 10.1016/j.mcna.2014.03.007. Epub 2014 May 9 [PubMed PMID: 24994054]
Varacallo MA,Fox EJ,Paul EM,Hassenbein SE,Warlow PM, Patients' response toward an automated orthopedic osteoporosis intervention program. Geriatric orthopaedic surgery & rehabilitation. 2013 Sep [PubMed PMID: 24319621]
Donnally III CJ, DiPompeo CM, Varacallo M. Vertebral Compression Fractures. StatPearls. 2023 Jan:(): [PubMed PMID: 28846351]
Tenny S, Munakomi S, Varacallo M. Odontoid Fractures. StatPearls. 2023 Jan:(): [PubMed PMID: 28722985]
Cornett CA,Vincent SA,Crow J,Hewlett A, Bacterial Spine Infections in Adults: Evaluation and Management. The Journal of the American Academy of Orthopaedic Surgeons. 2016 Jan [PubMed PMID: 26700630]
Tenny S,Varacallo M, Chordoma . 2018 Jan [PubMed PMID: 28613596]
Garg S, Dormans JP. Tumors and tumor-like conditions of the spine in children. The Journal of the American Academy of Orthopaedic Surgeons. 2005 Oct:13(6):372-81 [PubMed PMID: 16224110]
Al-Qurainy R,Collis E, Metastatic spinal cord compression: diagnosis and management. BMJ (Clinical research ed.). 2016 May 19 [PubMed PMID: 27199232]
Donnally III CJ,Varacallo M, Lumbar Degenerative Disk Disease . 2018 Jan [PubMed PMID: 28846354]
Donnally III CJ, Butler AJ, Varacallo M. Lumbosacral Disc Injuries. StatPearls. 2023 Jan:(): [PubMed PMID: 28846258]
Alexander CE,Varacallo M, Lumbosacral Facet Syndrome . 2018 Jan [PubMed PMID: 28722935]
Donnally III CJ,Varacallo M, Lumbar Spondylolysis And Spondylolisthesis . 2018 Jan [PubMed PMID: 28846329]
Munakomi S, Foris LA, Varacallo M. Spinal Stenosis and Neurogenic Claudication. StatPearls. 2023 Jan:(): [PubMed PMID: 28613622]
Alexander CE,Varacallo M, Lumbosacral Radiculopathy . 2018 Jan [PubMed PMID: 28613587]
Donnally III CJ, Munakomi S, Varacallo M. Basilar Invagination. StatPearls. 2023 Jan:(): [PubMed PMID: 28846299]
Hidalgo JA, Tork CA, Varacallo M. Arnold-Chiari Malformation. StatPearls. 2023 Jan:(): [PubMed PMID: 28613730]
Ng KS, Abdul Halim S. Anterior spinal cord syndrome as a rare complication of acute bacterial meningitis in an adult. BMJ case reports. 2018 Oct 24:2018():. pii: bcr-2018-226082. doi: 10.1136/bcr-2018-226082. Epub 2018 Oct 24 [PubMed PMID: 30361450]
Level 3 (low-level) evidenceLiu J, Li Z, Ye R, Liu J, Ren A. Periconceptional folic acid supplementation and sex difference in prevention of neural tube defects and their subtypes in China: results from a large prospective cohort study. Nutrition journal. 2018 Dec 12:17(1):115. doi: 10.1186/s12937-018-0421-3. Epub 2018 Dec 12 [PubMed PMID: 30541549]
Diaz E,Morales H, Spinal Cord Anatomy and Clinical Syndromes. Seminars in ultrasound, CT, and MR. 2016 Oct [PubMed PMID: 27616310]
Zeng Y, Ren H, Wan J, Lu J, Zhong F, Deng S. Cervical disc herniation causing Brown-Sequard syndrome: Case report and review of literature (CARE-compliant). Medicine. 2018 Sep:97(37):e12377. doi: 10.1097/MD.0000000000012377. Epub [PubMed PMID: 30213001]
Level 3 (low-level) evidenceRoth EJ,Park T,Pang T,Yarkony GM,Lee MY, Traumatic cervical Brown-Sequard and Brown-Sequard-plus syndromes: the spectrum of presentations and outcomes. Paraplegia. 1991 Nov [PubMed PMID: 1787982]
Dave BR,Samal P,Sangvi R,Degulmadi D,Patel D,Krishnan A, Does the Surgical Timing and Decompression Alone or Fusion Surgery in Lumbar Stenosis Influence Outcome in Cauda Equina Syndrome? Asian spine journal. 2018 Nov 27 [PubMed PMID: 30472822]
Olawin AM,M Das J, Spinal Anesthesia . 2020 Jan [PubMed PMID: 30725984]