Introduction
Sleep disorders are a group of conditions that disturb normal sleep patterns. Sleep disorders are one of the most common clinical problems encountered. Inadequate or non-restorative sleep can interfere with normal physical, mental, social, and emotional functioning. Sleep disorders can affect overall health, safety, and quality of life. A study showed significant impairment in the quality of life in patients with insomnia.[1]
There are many different types of sleep disorders. The International Classification of Sleep Disorders (ICSD) helps provide a standardized classification and definitions for sleep disorders.[2] Specifically, the third edition of the ICSD (ICSD-3) includes the following categories of sleep disorders:
- Insomnia
- Sleep-disordered breathing
- Central disorders of hypersomnolence
- Circadian rhythm sleep-wake disorders
- Parasomnias
- Sleep-related movement disorders
Sleep disorders are common in both adults and children. However, children with sleep disorders may present with different symptoms than adults. Children with sleep problems may exhibit motor overactivity, inattentiveness, irritability, or oppositional behavior rather than overt sleepiness.[3] Here we will review sleep disorders in adults, and sleep disorders in pediatrics will be discussed in a different section.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
There are different causes for different sleep disorders. For each sleep disorder listed below, more details are discussed in the pertinent section referenced below.
Insomnia
The exact causes of insomnia are unknown. Some contributing factors include environmental, genetic, psychological, and behavioral, leading to hyperarousal.[4][5]
Sleep-Disordered Breathing (SDB)
The causes of SDB range from breathing control to upper airway and chest wall mechanics, causing compromised ventilatory and resistive loading. SDB is a spectrum of disorders ranging from [6] syndrome to OSA and central sleep apnea (CSA). In the obstructive type of SDB, obesity plays a key role, and more information is discussed in the sections on OSA, CSA, and obesity hypoventilation syndrome.[6][7][8][9]
Central Disorders of Hypersomnolence
The central causes of hypersomnolence are commonly due to intrinsic abnormalities in the central nervous system's control of sleep-wake. Central hypersomnia is usually divided into three main subtypes: narcolepsy type 1, narcolepsy type 2, and idiopathic hypersomnia (IH), which are reviewed in more detail in separate sections.[10][11] In addition, other causes of central hypersomnolence include Kleine-Levin syndrome,[11] hypersomnia due to a medical disorder, medication or substance, psychiatric disorder, and sleep insufficiency syndrome.
Circadian Rhythm Sleep-Wake Disorders (CRSD)
The responsible causes of CRSD can be divided into two major groups (1): the environment is not well aligned with the internal circadian timing (e.g., shift work, jetlag); and (2) those occurring when the circadian timing system becomes altered relative to the external environment (e.g., delayed sleep phase syndrome, non-24, advanced sleep phase syndrome, irregular sleep-wake rhythm).[12] More details are outlined in separate review articles.[13]
Parasomnias
The causes of parasomnia vary from environmental, genetic, and gene-environment interactions, all of which may play a significant role in the origin of parasomnias.[14] Parasomnia is divided into the following major categories: Non-rapid eye movement (NREM)-related parasomnias, rapid eye movement (REM)-related parasomnias, and other parasomnias. NREM-related parasomnia includes confusional arousal, sleepwalking, sleep terrors, and a sleep-related eating disorder. REM-related parasomnias include REM sleep behavior disorder (RBD) and nightmare disorder.[15] The etiology of various types of parasomnia is discussed in a separate article.[16]
Sleep-Related Movement Disorders
Abnormal movements during sleep are disorders of motor control excitation or disinhibition often associated with sleep disturbances.[17] The etiology of various movements condition during sleep depends on the type of that disorder. For example, in restless legs syndrome (RLS), the etiology could be primarily due to familial and genetic predisposition or secondary to iron deficiency. More details on the etiology of RLS are discussed in a separate article.[18] Other sleep-related movement disorders include categories based on the type of movements: simple, periodic, rhythmic, or complex conditions (some of which are associated with parasomnias).[19] This will be discussed in detail in a dedicated section.
Epidemiology
The prevalence of sleep disorders differs based on the specific condition. A link between SDB, short sleep duration, and non-restorative sleep has recently been reported.[20] A recent study has linked poor sleep to other sleep disorders; for example, among a sample of patients with diabetes, 61% reported poor sleep, 47% of the participants screened positive for RLS, and 51% had an increased risk for OSA.[21] We will briefly list the prevalence of each major sleep disorder as classified by the ICSD-3.
Insomnia
Difficulty sleeping or insomnia symptoms are among the most common medical complaints affecting nearly a third of the adult population. When the symptoms are severe enough to cause daytime consequences, the prevalence is estimated to be approximately 10% and is higher among women than among men (17.6% vs. 10.1%%, respectively).[22] In addition, insomnia is found to be a persistent disorder (lasting over five years) and affects over 40% of patients if they have severe insomnia symptoms at presentation.[22]
Sleep-Disordered Breathing (SDB)
The prevalence of SDB is dependent on the type of disease. As people age, the incidence of sleep problems also rises. Approximately 50% of older adults have sleep problems.[23] Details on the prevalence of specific SDB (obstructive, central, upper airway resistance syndrome, sleep-related hypoventilation syndrome, or obesity hypoventilation) as outlined in their respective articles.[24][7][6][9][7]
Central Disorders of Hypersomnia
The prevalence of narcolepsy in the general population is approximately 142,600 individuals (44.3 per 100,000 persons), but there is a reported trend of increase over the last decade (by 14% from 38.9 in 2013 to 44.3 in 2016).[15]
Likewise, The prevalence of idiopathic hypersomnia also increased by 32% (from 7.8 to 10.3 per 100,000 persons), with similar rates between both sexes.
Circadian Rhythm Sleep-Wake Disorders (CRSD)
The prevalence of CRSD among the general population depends on the type and is reported to be between 0.13 to 0.17%.[25][26] However, the prevalence is higher among individuals with comorbid psychiatric illnesses.[27] Delayed sleep phase syndrome (DSPD) is common in adolescents and young adults, with an estimated prevalence of 7 to 16%.[28]
Parasomnia
Parasomnia, such as sleepwalking, confusional arousals, sleep terrors, sleep talking, and nightmares, are prevalent, including during childhood. The overall parasomnia prevalence in the no OSA group is approximately 3% in the NREM group (such as in sleepwalking, sexual acts during sleep, and sleep-related eating), 43.8% in nightmares, and the prevalence of RBD is estimated to be 8.7 per 100,000 people (with men to women ratio is 3:1).[29][15]
Sleep-Related Movement Disorders
Restless leg syndrome and periodic limb movement disorder are also more prevalent in the elderly.[30] Primary insomnia is more common in women over 50 than their male counterparts.[23] The prevalence of periodic leg movements disorder (PLMD) is approximately 40 per 100,000 persons and has increased in the last decade about 30%.
There are gender differences in many of these sleep disorders. The prevalence of insomnia is higher in women than men throughout most of life (with a ratio of 1.4:1.0).[31][23] The prevalence of RLS is twice as high for women as for men (9.0% vs. 5.4%) across all ages.[32] In contrast, the prevalence of SDB is higher in men than in premenopausal women (with a ratio of 2:1).[20] In the Wisconsin Sleep Cohort Study (WSCS), the prevalence of SDB increased over time n both sexes (26.4 to 33.9 % in men and 13.2 to 17.4 % in women).[33] Several possibilities for this increase in prevalence were contemplated, including increased obesity and aging of the general population, in addition to improved diagnostic techniques.
There are also racial and ethnic differences in the prevalence of sleep disorders.[34] In the Multi-Ethnic Study of Atherosclerosis (MESA), Hispanics and Chinese individuals had higher odds of SDB and short sleep than Whites. Likewise, Black have higher odds (1.8) for sleep apnea syndrome (AHI > five events per hour associated with excessive daytime sleepiness) compared to white after adjusting for age, gender and BMI.
History and Physical
The clinical presentations of sleep disorders depend on the specific disease. In general, sleep disturbances can present with a wide range of clinical pictures and commonly include insomnia, hypersomnia, or unusual sleep-related behaviors. Early identification of the underlying sleep disorder is essential to prevent complications and health consequences. A detailed history, sleep habits, and work schedule are critical to the assessment. Obtaining a complete list of medications (both prescribed and over-the-counter) is essential in assessing patients with sleep disturbances. In addition, evaluating detailed family and social history is very important, including any substances used by patients that can affect sleep and/or breathing.
Insomnia
Insomnia may present as difficulty falling asleep and/or staying asleep. Patients report taking thirty minutes or more to fall asleep (for those with sleep initiation difficulties) or spending thirty minutes or more awake during the night (for those with sleep maintenance difficulties). The diagnosis of insomnia also requires the presence of compromised daytime function, which includes one or more symptoms like fatigue, daytime sleepiness, poor attention, increased accidents, aggression, reduced motivation, or energy. Insomnia can often be a persistent or recurrent condition with exacerbations connected to medical, psychiatric, and psychosocial stressors. Recently insomnia was classified as a short-term and chronic type.[35]
The ICSD-3 criteria of the diagnosis of chronic insomnia disorder include the following three conditions: (1) difficulty in sleep initiation or maintenance, (2) adequate opportunity to sleep, and (3) presence of daytime consequences due to difficulty sleeping. These conditions should last for at least three months and thrice weekly.[35] Early identification of insomnia is crucial and requires a low threshold for suspicion. Clinical features that predispose, precipitate, and perpetuate insomnia symptoms should be identified from history.[36]
Hypersomnia
Patients with hypersomnia complain of disabling excessive daytime sleepiness. They find it difficult to maintain alertness during significant waking hours, with sleep occurring unintentionally or at inappropriate times that interfere with the daily routine. Many patients describe a considerable impact on their cognitive function, calling it brain fog. In addition, in idiopathic hypersomnia, there has been an association between excessive sleepiness and depressive symptom, and low quality of life.[37] Fatigue can present in a broad range of sleep disorders and can be confused with sleepiness.
The severity of hypersomnia and fatigue are commonly measured by questionnaires such as the Epworth sleepiness scale and fatigue severity scale.[38][39] Other sleepiness features are related to sleep duration, such as idiopathic hypersomnia (IH) or specific neurobiological disorder such as narcolepsy. IH has distinctive clinical features in addition to the severity of hypersomnia, such as prolonged nighttime sleep (more than 10 hours) and sleeps inertia.[37] Narcolepsy, however, is a chronic neurological disorder due to the brain's inability to control sleep and wakefulness. It is associated with a low cerebrospinal fluid level of orexin-A/hypocretin-1.
Patients with narcolepsy complain of excessive chronic daytime sleepiness with cataplexy (type I) or without cataplexy (type II) (transient loss of muscle tone in response to intense emotion such as laughter), hallucinations while falling asleep (hypnagogic hallucinations), or hallucinations while waking (hypnopompic hallucinations), and sleep paralysis (inability to move immediately after awakening). Cataplexy can be manifested commonly (more than 50% of the time) as nontypical presentations (including spontaneous cataplectic attacks or cataplexy induced by non-humorous triggers such as anger) and 30% as partial cataplexy (involves the jaw and the face).[40]
Excessive daytime sleepiness is one of the most common clinical presentations of sleep-disordered breathing (SDB) (reported usually in up to 50% of patients), in addition to loud snoring and observed apnea or gasping by a bed partner.[41] However, many patients with SDB are asymptomatic, particularly in special populations with heart failure, stroke, and other neurological disorders.[42] More details on SDB are described in separate articles.[24][7]
Unusual Sleep-Related Behaviors
Features of specific behavior before, during, or after sleep can provide essential clues to certain sleep disorders such as movement disorders, eating disorders, or parasomnia. For example, reporting sleep-related movement disorders such as the urge to move legs during a specific time of the evening could suggest restless leg movements or periodic leg movements, and further questions are needed to confirm the diagnosis. Confusional arousal or sleep drunkenness during arousal or awakening from sleep is a common manifestation of hypersomnolence disorder, such as idiopathic hypersomnia or, less commonly, sleep-related sex (sexsomnia).[43] Sexsomnia is abnormal sexual behaviors without recollection, including sexual intercourse with a bed partner, masturbation, or sexual vocalizations.[44]
Patients who report movements during sleep, such as kicking, punching, arm-flailing, or jumping from bed in response to violent dreams, could suffer from REM sleep behavior disorder (RBD). The patient can recall the dream if he awakens during the episode. This disorder may be associated with other medical conditions such as Parkinson disease, Lewy body dementia, or multiple system atrophy.[19] Other sleep-related symptoms that require detailed history to reach a clinical diagnosis include sleepwalking, sleep talking, and night terrors (common in children aged 2 to 12) and usually resolve spontaneously as the child ages). They mainly occur in non-REM sleep, without memory of the event. On the other hand, nightmares occur during REM sleep, usually in the middle of the night and early morning. During a nightmare, the person may scream and yell out things.
The difference between nightmares and night terrors is that the person can become fully alert when awakened during a nightmare. Also, there is a memory of the event in a nightmare, i.e., a person can recall a nightmare. Sleep-eating disorders are other unusual sleep-related behaviors that require detailed histories to differentiate from each other. Sleep-related eating disorders (SRED) manifest as recurrent episodes of involuntary eating during the first one-third of sleep with reduced consciousness. However, night eating syndrome (NES) manifests by excessive eating between dinner and bedtime or after a complete awakening from sleep.[45] Complex sleep behaviors are nonrapid eye movement (NREM)-related behaviors such as sleepwalking resulting in serious injuries or death, particularly among middle-aged and older patients with chronic insomnia.[46]
The symptoms associated with sleep disorders are commonly exacerbated by sleep deprivation, physical or emotional stress, traumatic events, and the use and abuse of substances or medications. Some of the medicines that are commonly linked to unusual sleep-related behaviors are antipsychotics and psychotropic medications (e.g., anticholinergics), sedatives, and hypnotic agents, particularly the class of Z drugs or nonbenzodiazepine benzodiazepine receptor agonists (e.g., zolpidem and eszopiclone) which now have a black box warning from US Food and Drug Administration (FDA) due to increased risk of complex sleep behaviors.[47]
Evaluation
A variety of information is required to evaluate sleep problems. After a detailed medical history, medication history, and physical examination, some clinical and investigative tools could help narrow the differential diagnosis and help identify the type of sleep disorders. Here is a list of some of these questionnaires and tests
Epworth sleepiness scale (ESS): ESS is an eight-item self-administered questionnaire that measures the presence and severity of sleepiness.[38]
Fatigue severity scale (FSS): FSS is a nine-item instrument that can help distinguish sleepiness from fatigue and estimate fatigue severity. [39]
Insomnia Severity Index (ISI): ISI is the most widely accepted clinical assessment tool that helps identify and monitor insomnia severity [48] in addition to a sleep diary.
Sleep diary: The sleep diary, or sleep log, is a personal paper record of sleep and wakefulness over weeks to months. Patients should record a detailed description of sleep, such as bedtime, duration until sleep onset, the number of awakenings, duration of awakenings, and nap times.
Sleep studies: Objective measures of sleep may be obtained by sleep studies such as home sleep apnea testing (HSAT) or polysomnography (PSG).[49] PSG is the gold standard for diagnosing OSA and other sleep disorders. During PSG, numerous monitoring devices are connected to the patient, allowing the patient to sleep. Various physiologic parameters such as respiratory effort, sleep stages, electrocardiography, airflow, body position, and limb movements are assessed. The information obtained from these parameters helps to diagnose various REM & NREM sleep disorders and determine the causes of sleep disturbance. In cases with a diagnosis of OSA and residual hypersomnia despite PAP therapy with adequate adherence, follow-up PSG can be used to reassess patients and ensure adequate PAP. However, a follow-up sleep study (PSG or HSAT) is not recommended in asymptomatic patients as a routine test.[50]
Laboratory studies: Some of the lab studies appropriate for those with sleep disorders include:
- Arterial blood gases (ABG)
- Thyroid function tests
- Drug and alcohol toxicity screening
- Iron studies and ferritin level
- Cerebrospinal fluid (CSF) hypocretin-1 deficiency (<110 pg/ml).[51]
Actigraphy: In this test, an actigraph device is worn on the wrist like a watch. The signals are detected when there is movement, and very few to no signs are recorded during sleep/inactivity. This device can assess sleep-wake cycles or circadian rhythm over an extended period and thus diagnose advanced or delayed sleep phase syndrome.
Multiple sleep latency testing (MSLT): This objective test determines the degree of sleepiness.[52] This test is often called a nap study. On the day following an overnight PSG study, the patient is asked to take four or five naps for 8 to 10 hours. Each nap lasts about 20 minutes. These tests help identify the causes of excessive daytime sleepiness, which can be present in various disorders such as sleep apnea, hypersomnia, and narcolepsy.[53]
Treatment / Management
Treatments for sleep disorders depend on the type of sleep disorder.
Treatment of insomnia can be broadly categorized into non-pharmacological and pharmacological treatments.
Non-pharmacological
- Cognitive-behavioral therapy for insomnia (CBT-I) includes a set of psychological and behavioral techniques specific to treating insomnia. Studies report that CBT-I is the psychological treatment of choice, using individual or group therapy techniques and, recently, digital CBT-I formats.[54][55] A meta-analysis of 61 randomized controlled trials, which included 11,571 participants and assessed different CBT-I delivery formats (individual, group, guided self-help, digital assisted, and unguided self-help ) with control conditions found that CBT-I not only significantly increases sleep parameters such as sleep efficiency and total sleep time but reduces sleep onset latency, wake after sleep onset, and insomnia severity.[54] CBT-I therapy is particularly important in groups of patients that may not tolerate pharmacological treatment, such as older patients, due to increased risk of side effects and addiction and tolerance to using Z drugs.[46] Other interventions are not proven to have a clinical effect if used alone.[56] These interventions include:
- Sleep restriction therapy (SRT): SRT limits the total time allowed in bed to increase the drive to sleep.
- Stimulus control therapy helps change sleep habits so that the patients don't have difficulty falling asleep. Patients should not go to bed until they are sleepy. Also, the bed should be used only for sleeping and not for watching television or reading books.
- Relaxation therapy: Relaxation techniques may be implemented before sleep. Meditation and breathing exercises are some of the relaxation techniques.
- Sleep hygiene: A set of education about lifestyle and environmental factors (e.g., light, noise, temperature) that may interfere with sleep. Sleep hygiene may include education about normal sleep, avoidance of substance use, regular exercise, bedroom environment, sleep and wake times, and avoidance of daytime naps. However, sleep hygiene education alone is less effective than CBT-I in individuals with poor sleep or insomnia.[56]
(A1)
Pharmacologic
- Histamine type 1 receptor blockers (e.g., chlorpheniramine and diphenhydramine) are commonly used for difficulty sleeping due to their sedative effects. However, due to their anticholinergic effect, these drugs should be avoided.
- Benzodiazepines (BZD): these drugs are commonly used to treat insomnia. The drugs bind to a particular benzodiazepine site on the gamma-aminobutyric acid (GABA) receptor complex, enhancing the activity of neurotransmitters. These drugs suppress REM sleep and reduce stage 3 sleep while increasing stage 2 sleep. Examples include flurazepam and temazepam.
- Non-benzodiazepine hypnotics or z-drugs: these agents are used to treat acute and short-term insomnia. These drugs have non-BZD-like chemical structures but interact with the GABA-BZD receptor, causing sedation. Examples include zolpidem and zaleplon.
- Melatonin receptor agonists: the melatonin receptors MT1 and MT2 are implicated in regulating sleepiness and the sleep-wake cycle. Melatonin receptor agonists act on these receptors and improve sleep through the endogenous regulating system. These drugs are used in circadian rhythm sleep disorders, jet lag, and delayed sleep-wake phase disorder (insomnia with difficulty in sleep onset).[57][58][59] An example includes ramelteon.
- Orexin receptor antagonists: orexin promotes wakefulness. Thus, the antagonism of this receptor helps in sleep. An example includes suvorexant, which improved ISI through improvement in sleep onset and maintenance.[60] (A1)
Treatment of OSA includes primarily mechanical positive airway therapy (PAP), lifestyle changes, and options of oral appliances or surgical procedures in certain patients.[24]. The use of drug treatment such as solriamfetol, stimulants (such as amphetamines or modafinil), and norepinephrine reuptake inhibitors to increase wakefulness in patients with OSA and persistent hypersomnia despite adequate PAP adherence and elimination of respiratory events can be considered in selected patients to treat their day time symptoms.[61][62] A long-term study of the safety and efficacy of solriamfetol under open-label and double-blind, placebo-controlled conditions demonstrated long-term efficacy of solriamfetol and reported side effects in less than 5% of patients with OSA or narcolepsy such as headache, nausea, nasopharyngitis, insomnia, dry mouth, anxiety, decreased appetite, and upper respiratory tract infection.[63](A1)
A number of medications can be used for the treatment of narcolepsy. Modafinil, a non-amphetamine stimulant that promotes wakefulness, is considered first-line therapy for narcolepsy as it reduces daytime sleepiness, is well tolerated, and has less abuse potential compared to traditional stimulants (amphetamines, methylphenidate). These traditional drugs are second-line drugs. Patients with significant cataplexy may benefit from REM-suppressing medications such as anti-depressants and sodium oxybate.
Light-phase shift therapy is useful for sleep disturbances associated with circadian rhythm abnormalities.[64] Patients may be exposed to bright light to help normalize their sleep schedule.(A1)
Gabapentin enacarbil, a prodrug formulation of gabapentin, significantly improves restless leg syndrome and hence can alleviate sleep disturbance.[65](A1)
Differential Diagnosis
The differential diagnosis of sleep disorders are as follows:
- Post-traumatic stress disorder (PTSD)
- Depression
- Anxiety disorder
- Bipolar disorder
- Opioid abuse
- Alcoholism
- Stimulants abuse (amphetamine)
- Chronic obstructive pulmonary disease (COPD)
- Hyperthyroidism
Prognosis
Insufficient sleep can result in industrial or motor vehicle accidents, decreased work performance, and cognitive dysfunction. The prognosis of sleep disorders depends widely on the cause of the sleep disorder. Insomnia due to OSA generally resolves with treatment, whereas patients with chronic insomnia have an increased risk of depression, anxiety, and reduced quality of life.
Complications
Untreated sleep disorders may lead to an increased risk of accidents and the development of various serious complications.[66] Mood and anxiety disorders may develop. Sleep deprivation can lead to false memory and a decline in cognitive functioning.[67]
Patients with periodic limb movement sleep disorder may have a higher risk of cerebrovascular accidents.[68]
Untreated OSA (especially if severe and associated with hypersomnia) can lead to various cardiovascular disorders.[69]
Deterrence and Patient Education
All patients should be educated well and encouraged to practice good sleep hygiene. "Sleep hygiene" is a term used to describe good sleep habits.
The following advice should be given to the patients to practice good sleep hygiene:
- Maintain a regular schedule, i.e., go to bed and wake up at the same time every day
- Use the bed for sleep and sex only. Avoid watching television, looking at phones, or reading in the bed
- Exercise almost every day, but not right before bedtime
- Avoid caffeine or smoking, mainly during the evening
- Maintain a dark, calm, and quiet environment in the bedroom
- Avoid struggling to fall asleep in bed. If you can't sleep, get up and try again later or change the bed.
Also, if the patient takes sedative-hypnotic medications, this should be documented in the medical record. Patients should be counseled to avoid driving and operating machines when under these medications.
Enhancing Healthcare Team Outcomes
The proper management of sleep disorders requires the efforts of an interprofessional healthcare team that includes clinicians (MDs, DOs, NPs, and PAs), specialists, pharmacists, nursing staff, psychological professionals (social workers, counselors, etc.), and in some cases a sleep clinic, and a dietician. Surgical consultations are required for some of the underlying causes of insomnia, such as in cases of OSA, which may require palate surgery. Interprofessional collaboration is essential for good patient outcomes in sleep disorders.
Nurses can coordinate activities between the managing clinicians and other health professionals on the case, as well as counsel the patient and answer any questions. The pharmacist will verify the medication dosing, check for interactions, and counsel patients on proper administration. Sleep clinics will look deeper into the case, including potential sleep studies, when indicated. Psychological professionals will work with any issues that may contribute to sleep problems and report to the rest of the interprofessional team. Clinicians will do well to consider input from all team members in deciding their course of therapy; the patient and possibly family (e.g., spouses, parents) are also members of the care team.
All interprofessional team members are responsible for maintaining accurate and updated records regarding the patient's case with every interaction or intervention taken. They must also be free to openly communicate with all other team members when there are any concerns about the patient's condition or progress. This interprofessional model will help drive optimal outcomes for those patients who experience issues with sleep disorders of any type. [Level 5]
Media
(Click Image to Enlarge)
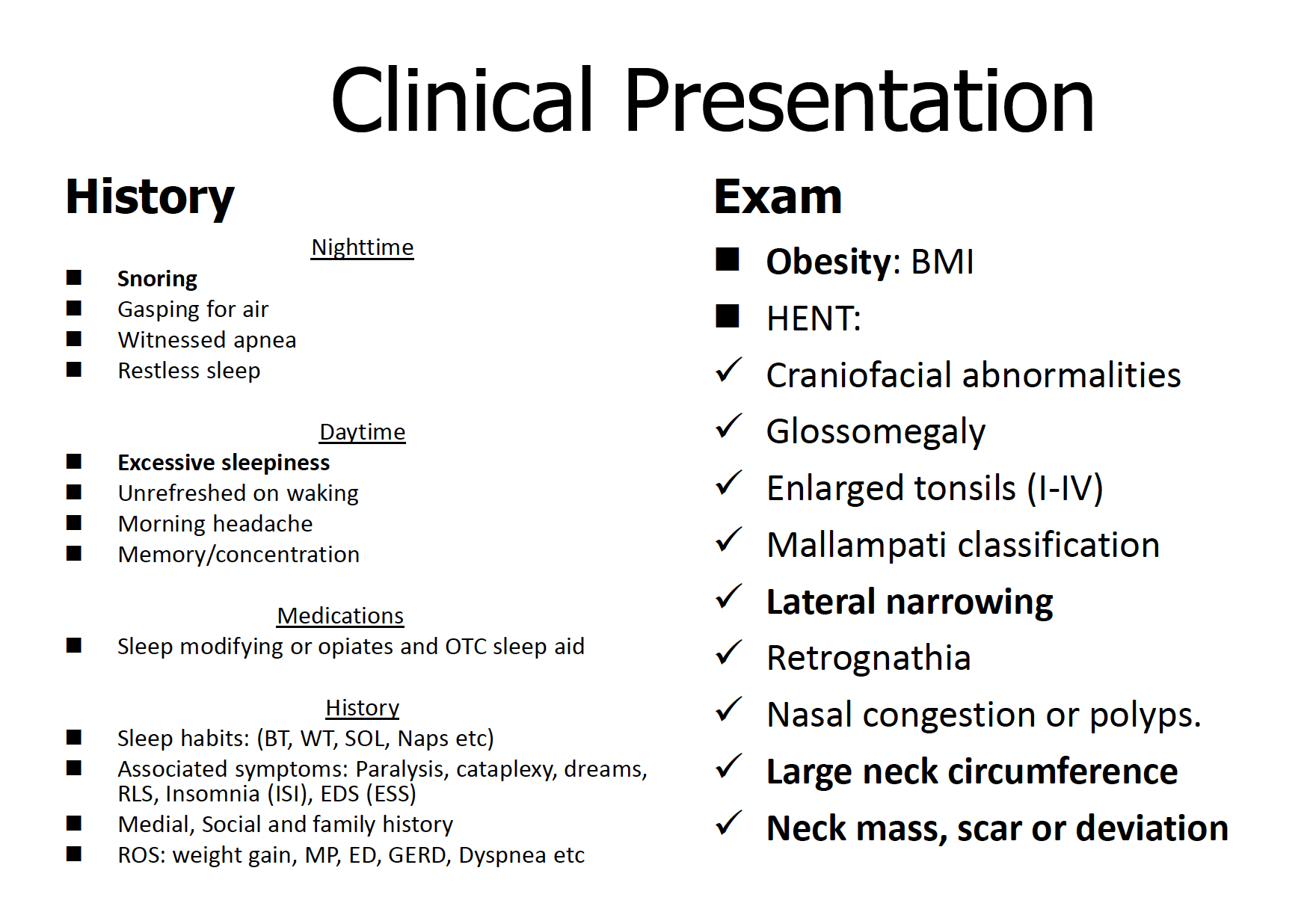
Sleep Apnea Clinical Assessment. The image demonstrates the clinical assessment of patients with suspected sleep apnea.
Contributed by A Sankari, MD, PhD
References
Zammit GK,Weiner J,Damato N,Sillup GP,McMillan CA, Quality of life in people with insomnia. Sleep. 1999 May 1; [PubMed PMID: 10394611]
Level 2 (mid-level) evidenceGauld C,Lopez R,Geoffroy PA,Morin CM,Guichard K,Giroux É,Dauvilliers Y,Dumas G,Philip P,Micoulaud-Franchi JA, A systematic analysis of ICSD-3 diagnostic criteria and proposal for further structured iteration. Sleep medicine reviews. 2021 Aug; [PubMed PMID: 33596531]
Level 1 (high-level) evidenceHuyett P,Siegel N,Bhattacharyya N, Prevalence of Sleep Disorders and Association With Mortality: Results From the NHANES 2009-2010. The Laryngoscope. 2020 Jul 18 [PubMed PMID: 32681735]
Kaur H, Spurling BC, Bollu PC. Chronic Insomnia. StatPearls. 2023 Jan:(): [PubMed PMID: 30252392]
Momin RR,Ketvertis K, Short Term Insomnia StatPearls. 2022 Jan [PubMed PMID: 32119403]
Maggard MD, Sankari A, Cascella M. Upper Airway Resistance Syndrome. StatPearls. 2025 Jan:(): [PubMed PMID: 33232072]
Rana AM, Sankari A. Central Sleep Apnea. StatPearls. 2024 Jan:(): [PubMed PMID: 35201727]
Ghimire P, Sankari A, Antoine MH, Bollu PC, Kaul P. Obesity-Hypoventilation Syndrome. StatPearls. 2025 Jan:(): [PubMed PMID: 31194373]
Antoine MH, Sankari A, Bollu PC. Obesity-Hypoventilation Syndrome(Archived). StatPearls. 2025 Jan:(): [PubMed PMID: 29493925]
Slowik JM,Collen JF,Yow AG, Narcolepsy StatPearls. 2022 Jan [PubMed PMID: 29083681]
Shah F,Gupta V, Kleine–Levin syndrome (KLS) StatPearls. 2022 Jan [PubMed PMID: 33760515]
Okawa M,Uchiyama M, Circadian rhythm sleep disorders: characteristics and entrainment pathology in delayed sleep phase and non-24-h sleep-wake syndrome. Sleep medicine reviews. 2007 Dec; [PubMed PMID: 17964201]
Basit H,Damhoff TC,Huecker MR, Sleeplessness And Circadian Disorder StatPearls. 2022 Jan; [PubMed PMID: 30480971]
Hublin C,Kaprio J, Genetic aspects and genetic epidemiology of parasomnias. Sleep medicine reviews. 2003 Oct [PubMed PMID: 14573377]
Acquavella J,Mehra R,Bron M,Suomi JM,Hess GP, Prevalence of narcolepsy and other sleep disorders and frequency of diagnostic tests from 2013-2016 in insured patients actively seeking care. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2020 Aug 15 [PubMed PMID: 32807293]
Fariba KA,Tadi P, Parasomnias StatPearls. 2022 Jan [PubMed PMID: 32809359]
Bargiotas P,Bassetti CL, Sleep-related movement disorders and disturbances of motor control. Current opinion in neurology. 2017 Aug; [PubMed PMID: 28582324]
Level 3 (low-level) evidenceMansur A,Castillo PR,Rocha Cabrero F,Bokhari SRA, Restless Legs Syndrome StatPearls. 2022 Jan; [PubMed PMID: 28613628]
Pham CK,Sankari A,Slowik JM, Rapid Eye Movement Sleep Behavior Disorder StatPearls. 2022 Jan [PubMed PMID: 32310388]
Matsumoto T,Chin K, Prevalence of sleep disturbances: Sleep disordered breathing, short sleep duration, and non-restorative sleep. Respiratory investigation. 2019 May [PubMed PMID: 30827934]
Demirtaş H, Dolu İ. The prevalence of poor sleep quality and its association with the risk of obstructive sleep apnea and restless legs syndrome in diabetic patients treated with cyanoacrylate glue for varicose veins. Sleep & breathing = Schlaf & Atmung. 2023 May:27(2):745-755. doi: 10.1007/s11325-022-02676-1. Epub 2022 Jul 1 [PubMed PMID: 35776370]
Level 2 (mid-level) evidenceMorin CM, Jarrin DC, Ivers H, Mérette C, LeBlanc M, Savard J. Incidence, Persistence, and Remission Rates of Insomnia Over 5 Years. JAMA network open. 2020 Nov 2:3(11):e2018782. doi: 10.1001/jamanetworkopen.2020.18782. Epub 2020 Nov 2 [PubMed PMID: 33156345]
Rodriguez JC,Dzierzewski JM,Alessi CA, Sleep problems in the elderly. The Medical clinics of North America. 2015 Mar; [PubMed PMID: 25700593]
Slowik JM, Sankari A, Collen JF. Obstructive Sleep Apnea. StatPearls. 2024 Jan:(): [PubMed PMID: 29083619]
Yazaki M,Shirakawa S,Okawa M,Takahashi K, Demography of sleep disturbances associated with circadian rhythm disorders in Japan. Psychiatry and clinical neurosciences. 1999 Apr; [PubMed PMID: 10459707]
Level 2 (mid-level) evidenceSchrader H,Bovim G,Sand T, The prevalence of delayed and advanced sleep phase syndromes. Journal of sleep research. 1993 Mar [PubMed PMID: 10607071]
Takaesu Y,Inoue Y,Murakoshi A,Komada Y,Otsuka A,Futenma K,Inoue T, Prevalence of Circadian Rhythm Sleep-Wake Disorders and Associated Factors in Euthymic Patients with Bipolar Disorder. PloS one. 2016 [PubMed PMID: 27442503]
Liu C,Tang X,Gong Z,Zeng W,Hou Q,Lu R, Circadian Rhythm Sleep Disorders: Genetics, Mechanisms, and Adverse Effects on Health. Frontiers in genetics. 2022 [PubMed PMID: 35571019]
Lundetræ RS,Saxvig IW,Pallesen S,Aurlien H,Lehmann S,Bjorvatn B, Prevalence of Parasomnias in Patients With Obstructive Sleep Apnea. A Registry-Based Cross-Sectional Study. Frontiers in psychology. 2018; [PubMed PMID: 30026716]
Level 2 (mid-level) evidenceGulia KK,Kumar VM, Sleep disorders in the elderly: a growing challenge. Psychogeriatrics : the official journal of the Japanese Psychogeriatric Society. 2018 May; [PubMed PMID: 29878472]
Phillips BA,Collop NA,Drake C,Consens F,Vgontzas AN,Weaver TE, Sleep disorders and medical conditions in women. Proceedings of the Women [PubMed PMID: 18710367]
Allen RP,Walters AS,Montplaisir J,Hening W,Myers A,Bell TJ,Ferini-Strambi L, Restless legs syndrome prevalence and impact: REST general population study. Archives of internal medicine. 2005 Jun 13 [PubMed PMID: 15956009]
Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. American journal of epidemiology. 2013 May 1:177(9):1006-14. doi: 10.1093/aje/kws342. Epub 2013 Apr 14 [PubMed PMID: 23589584]
Level 2 (mid-level) evidenceChen X,Wang R,Zee P,Lutsey PL,Javaheri S,Alcántara C,Jackson CL,Williams MA,Redline S, Racial/Ethnic Differences in Sleep Disturbances: The Multi-Ethnic Study of Atherosclerosis (MESA). Sleep. 2015 Jun 1 [PubMed PMID: 25409106]
Level 2 (mid-level) evidenceSateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014 Nov:146(5):1387-1394. doi: 10.1378/chest.14-0970. Epub [PubMed PMID: 25367475]
Ellis JG,Perlis ML,Espie CA,Grandner MA,Bastien CH,Barclay NL,Altena E,Gardani M, The natural history of insomnia: predisposing, precipitating, coping, and perpetuating factors over the early developmental course of insomnia. Sleep. 2021 Sep 13; [PubMed PMID: 33849074]
Rassu AL,Evangelista E,Barateau L,Chenini S,Lopez R,Jaussent I,Dauvilliers Y, Idiopathic Hypersomnia Severity Scale to better quantify symptoms severity and their consequences in idiopathic hypersomnia. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2022 Feb 1 [PubMed PMID: 34596041]
Johns MW. Sleepiness in different situations measured by the Epworth Sleepiness Scale. Sleep. 1994 Dec:17(8):703-10 [PubMed PMID: 7701181]
Lichstein KL,Means MK,Noe SL,Aguillard RN, Fatigue and sleep disorders. Behaviour research and therapy. 1997 Aug [PubMed PMID: 9256516]
Level 2 (mid-level) evidenceOvereem S, van Nues SJ, van der Zande WL, Donjacour CE, van Mierlo P, Lammers GJ. The clinical features of cataplexy: a questionnaire study in narcolepsy patients with and without hypocretin-1 deficiency. Sleep medicine. 2011 Jan:12(1):12-8. doi: 10.1016/j.sleep.2010.05.010. Epub 2010 Dec 8 [PubMed PMID: 21145280]
Gottlieb DJ, Punjabi NM. Diagnosis and Management of Obstructive Sleep Apnea: A Review. JAMA. 2020 Apr 14:323(14):1389-1400. doi: 10.1001/jama.2020.3514. Epub [PubMed PMID: 32286648]
Sankari A, Vaughan S, Bascom A, Martin JL, Badr MS. Sleep-Disordered Breathing and Spinal Cord Injury: A State-of-the-Art Review. Chest. 2019 Feb:155(2):438-445. doi: 10.1016/j.chest.2018.10.002. Epub 2018 Oct 12 [PubMed PMID: 30321507]
Trotti LM. Idiopathic Hypersomnia. Sleep medicine clinics. 2017 Sep:12(3):331-344. doi: 10.1016/j.jsmc.2017.03.009. Epub 2017 Jun 16 [PubMed PMID: 28778232]
Schenck CH,Arnulf I,Mahowald MW, Sleep and sex: what can go wrong? A review of the literature on sleep related disorders and abnormal sexual behaviors and experiences. Sleep. 2007 Jun; [PubMed PMID: 17580590]
Loddo G,Zanardi M,Caletti MT,Mignani F,Petroni ML,Chiaro G,Marchesini G,Provini F, Searching food during the night: the role of video-polysomnography in the characterization of the night eating syndrome. Sleep medicine. 2019 Dec [PubMed PMID: 31671328]
Guo F,Yi L,Zhang W,Bian ZJ,Zhang YB, Association Between Z Drugs Use and Risk of Cognitive Impairment in Middle-Aged and Older Patients With Chronic Insomnia. Frontiers in human neuroscience. 2021; [PubMed PMID: 34955792]
Harbourt K,Nevo ON,Zhang R,Chan V,Croteau D, Association of eszopiclone, zaleplon, or zolpidem with complex sleep behaviors resulting in serious injuries, including death. Pharmacoepidemiology and drug safety. 2020 Jun [PubMed PMID: 32323442]
Morin CM, Belleville G, Bélanger L, Ivers H. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011 May 1:34(5):601-8 [PubMed PMID: 21532953]
Level 3 (low-level) evidenceKapur VK, Auckley DH, Chowdhuri S, Kuhlmann DC, Mehra R, Ramar K, Harrod CG. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2017 Mar 15:13(3):479-504. doi: 10.5664/jcsm.6506. Epub 2017 Mar 15 [PubMed PMID: 28162150]
Level 1 (high-level) evidenceCaples SM,Anderson WM,Calero K,Howell M,Hashmi SD, Use of polysomnography and home sleep apnea tests for the longitudinal management of obstructive sleep apnea in adults: an American Academy of Sleep Medicine clinical guidance statement. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2021 Jun 1 [PubMed PMID: 33704050]
van der Hoeven AE,Fronczek R,Schinkelshoek MS,Roelandse FWC,Bakker JA,Overeem S,Bijlenga D,Lammers GJ, Intermediate hypocretin-1 cerebrospinal fluid levels and typical cataplexy: their significance in the diagnosis of narcolepsy type 1. Sleep. 2022 May 12; [PubMed PMID: 35554594]
Dietmann A,Gallino C,Wenz E,Mathis J,Bassetti CLA, Multiple sleep latency test and polysomnography in patients with central disorders of hypersomnolence. Sleep medicine. 2021 Mar [PubMed PMID: 33453460]
Krahn LE,Arand DL,Avidan AY,Davila DG,DeBassio WA,Ruoff CM,Harrod CG, Recommended protocols for the Multiple Sleep Latency Test and Maintenance of Wakefulness Test in adults: guidance from the American Academy of Sleep Medicine. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2021 Dec 1 [PubMed PMID: 34423768]
Gao Y,Ge L,Liu M,Niu M,Chen Y,Sun Y,Chen J,Yao L,Wang Q,Li Z,Xu J,Li M,Hou L,Shi J,Yang K,Cai Y,Li L,Zhang J,Tian J, Comparative efficacy and acceptability of cognitive behavioral therapy delivery formats for insomnia in adults: A systematic review and network meta-analysis. Sleep medicine reviews. 2022 May 31; [PubMed PMID: 35759820]
Level 2 (mid-level) evidenceEspie CA,Emsley R,Kyle SD,Gordon C,Drake CL,Siriwardena AN,Cape J,Ong JC,Sheaves B,Foster R,Freeman D,Costa-Font J,Marsden A,Luik AI, Effect of Digital Cognitive Behavioral Therapy for Insomnia on Health, Psychological Well-being, and Sleep-Related Quality of Life: A Randomized Clinical Trial. JAMA psychiatry. 2019 Jan 1 [PubMed PMID: 30264137]
Level 2 (mid-level) evidenceEdinger JD,Arnedt JT,Bertisch SM,Carney CE,Harrington JJ,Lichstein KL,Sateia MJ,Troxel WM,Zhou ES,Kazmi U,Heald JL,Martin JL, Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2021 Feb 1 [PubMed PMID: 33164741]
Level 1 (high-level) evidenceXie Z,Chen F,Li WA,Geng X,Li C,Meng X,Feng Y,Liu W,Yu F, A review of sleep disorders and melatonin. Neurological research. 2017 Jun; [PubMed PMID: 28460563]
Sletten TL,Magee M,Murray JM,Gordon CJ,Lovato N,Kennaway DJ,Gwini SM,Bartlett DJ,Lockley SW,Lack LC,Grunstein RR,Rajaratnam SMW, Efficacy of melatonin with behavioural sleep-wake scheduling for delayed sleep-wake phase disorder: A double-blind, randomised clinical trial. PLoS medicine. 2018 Jun; [PubMed PMID: 29912983]
Level 1 (high-level) evidenceAuld F,Maschauer EL,Morrison I,Skene DJ,Riha RL, Evidence for the efficacy of melatonin in the treatment of primary adult sleep disorders. Sleep medicine reviews. 2017 Aug; [PubMed PMID: 28648359]
Herring WJ,Connor KM,Snyder E,Snavely DB,Morin CM,Lines C,Michelson D, Effects of suvorexant on the Insomnia Severity Index in patients with insomnia: analysis of pooled phase 3 data. Sleep medicine. 2019 Apr [PubMed PMID: 30522875]
Schweitzer PK,Rosenberg R,Zammit GK,Gotfried M,Chen D,Carter LP,Wang H,Lu Y,Black J,Malhotra A,Strohl KP, Solriamfetol for Excessive Sleepiness in Obstructive Sleep Apnea (TONES 3). A Randomized Controlled Trial. American journal of respiratory and critical care medicine. 2019 Jun 1; [PubMed PMID: 30521757]
Level 1 (high-level) evidenceWang J,Yang S,Li X,Wang T,Xu Z,Xu X,Gao H,Chen G, Efficacy and safety of solriamfetol for excessive sleepiness in narcolepsy and obstructive sleep apnea: findings from randomized controlled trials. Sleep medicine. 2021 Mar; [PubMed PMID: 33472129]
Level 1 (high-level) evidenceMalhotra A,Shapiro C,Pepin JL,Hedner J,Ahmed M,Foldvary-Schaefer N,Strollo PJ,Mayer G,Sarmiento K,Baladi M,Chandler P,Lee L,Schwab R, Long-term study of the safety and maintenance of efficacy of solriamfetol (JZP-110) in the treatment of excessive sleepiness in participants with narcolepsy or obstructive sleep apnea. Sleep. 2020 Feb 13 [PubMed PMID: 31691827]
Faulkner SM,Bee PE,Meyer N,Dijk DJ,Drake RJ, Light therapies to improve sleep in intrinsic circadian rhythm sleep disorders and neuro-psychiatric illness: A systematic review and meta-analysis. Sleep medicine reviews. 2019 Aug; [PubMed PMID: 31108433]
Level 1 (high-level) evidenceAhmed M,Hays R,Steven Poceta J,Jaros MJ,Kim R,Shang G, Effect of Gabapentin Enacarbil on Individual Items of the International Restless Legs Study Group Rating Scale and Post-sleep Questionnaire in Adults with Moderate-to-Severe Primary Restless Legs Syndrome: Pooled Analysis of 3 Randomized Trials. Clinical therapeutics. 2016 Jul; [PubMed PMID: 27288210]
Level 1 (high-level) evidencePocobelli G,Akosile MA,Hansen RN,Eavey J,Wellman RD,Johnson RL,Carls G,Bron M,Dublin S, Obstructive sleep apnea and risk of motor vehicle accident. Sleep medicine. 2021 Sep [PubMed PMID: 34348205]
Lo JC,Chong PL,Ganesan S,Leong RL,Chee MW, Sleep deprivation increases formation of false memory. Journal of sleep research. 2016 Dec; [PubMed PMID: 27381857]
Lin TC,Zeng BY,Chen YW,Wu MN,Chen TY,Lin PY,Wu CK,Tseng PT,Hsu CY, Cerebrovascular Accident Risk in a Population with Periodic Limb Movements of Sleep: A Preliminary Meta-Analysis. Cerebrovascular diseases (Basel, Switzerland). 2018; [PubMed PMID: 29982243]
Level 1 (high-level) evidenceYasir M, Pervaiz A, Sankari A. Cardiovascular Outcomes in Sleep-Disordered Breathing: Are We Under-estimating? Frontiers in neurology. 2022:13():801167. doi: 10.3389/fneur.2022.801167. Epub 2022 Mar 15 [PubMed PMID: 35370882]