Introduction
Bones are often considered static structures that only offer structural support (see Image. Parts of a Long Bone). However, bones have many functions, like other organ systems. Besides serving as a framework for soft tissue, bones permit locomotion, protect vital organs, facilitate breathing, play a role in electrolyte homeostasis, and house hematopoietic sites. Bone remodeling continues throughout life, driven by physiologic demands.
The skeletal system can respond to increased mechanical stress by activating osteogenesis—the bone formation process. This ability is evident in how resistance training shapes the body. Resistance exercise has proven to be a viable therapeutic option for osteosarcopenia or age-related bone and muscle loss.[1] Bones adapt in response to both external and internal stimuli. Unlike other organs, these hard structures may break when subjected to excessive force but regenerate without fibrosis or scarring.
Human infants typically have 270 bones, fusing into around 206 in the human adult. Variability in number arises from some bones' anatomic variations. Bones differ in size, shape, and strength, depending on function.[2] Understanding bone anatomy and physiology helps healthcare professionals treat skeletal conditions.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Bone Structure
From a histological perspective, bones are highly specialized connective tissues that can remodel based on exogenous demand. The cell primarily responsible for building bones is the osteoblast, which secretes a collagen-rich fluid known as osteoid. Ground substance, composed primarily of osteocalcin and chondroitin sulfate, is also present in osteoid.
Bone hardening requires mineralization, making bones the body's main calcium and phosphate reservoir. These ions are typically obtained from the diet, eg, dairy products.[3] However, calcium and phosphate can easily deplete if not stored in bones. Mineralization transforms the osteoblast into the mature bone cell, the osteocyte.
The osteon is the bone's functional unit (see Image. Osteon). Osteocytes are typically found in the osteon's lacunae arranged concentrically around a central opening, the Haversian canal. Canaliculi are osteocyte processes interconnected by gap junctions, allowing the mature bone cells to communicate and exchange cytoplasmic contents.
The osteon's blood supply originates from the highly vascularized periosteum, the soft tissue covering the bone's outer surface. Periosteal blood vessels reach the Haversian canal via the endosteum-lined Volkmann canals, the perpendicular channels traversing the osteon. Arteries emanating from the Haversian canal supply the osteocytes in the inner two-thirds of cortical bone and the marrow cavity.
From a gross anatomical perspective, most bones have a well-organized, compact outer shell comprised of osteons known as the cortex. Bones' meshlike inner portions are called "trabecular bones," "spongy bones," or "cancellous bones." The inner surface's meshlike quality reduces the impact of strong external forces and leaves space for hematopoiesis. Osteons run parallel to the bone shaft.
The ratio of cortical to trabecular bone in healthy adults is approximately 80:20.[4] The vertebrae are the only bones without a true cortex and are entirely covered by a dense trabecular network. The periosteum covers all bones, providing innervation, circulation, and nutrition, especially to the bone's outer third.
Bone Classification
Bones can be classified into long, short, and flat bones based on shape. Long bones evolve via endochondral ossification. Examples of long bones are the femur and phalanges. These bones vary in size and are typically tubular. Long bones have 3 distinct anatomical zones:
- Diaphysis: Also known as the shaft. The diaphysis contains the bone medulla, which houses yellow marrow.
- Epiphysis: Located at the tip of the long bone, typically responsible for articulation. The epiphysis is also the primary source of red marrow in long bones, the site of erythropoiesis.
- Metaphysis: The region between the diaphysis and epiphysis that contains the epiphyseal plate in children. Epiphyseal plates are responsible for linear bone growth and remain cartilaginous until after puberty. After ossification, the metaphysis becomes primarily responsible for transferring mechanical loads from the epiphysis to the diaphysis.[5]
Short bones also evolve by endochondral ossification but are smaller and take on different shapes. Examples of short bones are the carpal bones.
Flat bones form by intramembranous ossification and have unique, plate-like shapes. Examples include the sternum and cranial bones.
Bone Cells
Pluripotent mesenchymal stem cells form the osteoblasts, which later become the osteocytes. During bone remodeling, osteocyte apoptosis sends signals to marrow osteoblasts to activate osteoclast formation. Osteoclasts are myeloid-derived cells that initiate bone resorption.[6]
Bone Composition
The bone's extracellular matrix comprises collagen type I and crystals of the calcium phosphate mineral, calcium hydroxyapatite. The osteon contains the osteocytes, which are crucial to bone integrity and the remodeling process. Cement lines, also known as cement sheaths, delineate the osteons and have a higher mineral density than other parts of the bone matrix.[7]
Bone Remodeling
Bone undergoes constant remodeling in response to stress and hormonal control. Bone is resorbed under conditions of reduced stress, leading to bone loss. Thus, bedridden patients and astronauts on prolonged space travel develop weaker bones over time.
During remodeling, osteocyte apoptosis signals osteoblasts to induce osteoclast differentiation from myeloid cells. Osteoclasts remove old osteocytes, initiate bone resorption, and form new osteoblasts. New osteocytes arise from new osteoblasts.
Osteoclasts are multinucleated cells found in Howship lacunae on the bone's inner surface. The osteoclasts' outer membranes contain the receptor activator of nuclear factor-kappa B (RANK). This receptor is activated by the osteoblasts' product, the receptor activator of nuclear factor-kappa B ligand (RANKL). Another osteoblastic secretion, osteoprotegerin, disrupts RANK-RANKL interaction to prevent osteoclast differentiation.[8]
Osteoclasts use carbonic anhydrase and collagenase to break down the bone matrix. Carbonic anhydrase is a proton-producing enzyme that acidifies the bone matrix. Collagenase is an enzyme that degrades collagen.[9]
Estrogen increases osteoblastic activity. Reduced estrogen levels in postmenopausal women put them at risk of bone loss, osteoporosis, and fractures.[10]
Embryology
Most bones arise from the mesoderm. Middle ear ossicles and some craniofacial bones originate from neural crest cells. Long and short bones form from cartilaginous precursors and later undergo endochondral ossification. Flat bones evolve differently and develop by intramembranous ossification. During intramembranous ossification, osteoblasts produce bone spicules, which form trabeculae. Woven bone arises from merging trabeculae. Periosteum comes from the mesenchymal cells surrounding the trabeculae. Osteogenic cells from the periosteum grow along the woven bone's surface and become lamellar bone after mineralization. Osteogenesis starts in the 6th week of development and continues until age 25.[11]
Blood Supply and Lymphatics
Long bones have a nutrient artery that enters the midshaft region. The nutrient artery divides into longitudinal branches in the marrow cavity that travel toward each bone tip. Nearly all long bones have a nutrient artery that passes through the nutrient foramen in the diaphysis' middle third. Some may have 2 nutrient arteries.
The periosteum surrounds the bone surface. Volkmann canals connect the periosteum's blood vessels to those inside the Haversian canals and adjacent osteons. Small periosteal branches supply most compact bones. Stripping off the periosteum may lead to bone cell death.
The epiphyses receive their own blood supply from the epiphyseal arteries, which arise from articular anastomoses.[12]
Nerves
Periosteal nerves are mostly pain fibers. The pain afferents carry signals to spinal nuclei via the dorsal root ganglia. Efferent innervation on the periosteum and inside the bone comes from the sympathetic nervous system, which regulates blood flow in these areas. The sympathetic cell bodies are located in the spinal cord's intermediolateral column, and their axons form the sympathetic ganglia. Postganglionic fibers pass via the gray rami communicantes to the branches of the cervical, brachial, or lumbosacral plexuses. Fibers from these plexuses reach the bone.[13] Besides sensing pain and regulating blood flow, recent evidence shows that nerves within bones are crucial to bone regeneration after a fracture. Denervated bones tend to develop smaller calluses during the repair process.[14]
Surgical Considerations
Fractures must be surgically repaired to ensure proper healing. Otherwise, malunion or nonunion can occur, causing mobility problems. Most pediatric fractures heal spontaneously or by splinting due to young bone's malleability. However, pediatric epiphyseal fractures may result in growth stunting and long bone deformities.[15] Adult fractures may be repaired by nails, screws, and plates by open reduction and internal fixation.
Clinical Significance
Bone Fractures
Bone fractures vary in severity. Simple fractures may heal with supportive measures or closed procedures, such as splinting, casting, and closed reduction. Severe injuries typically require open reduction aided by nails, plates, and screws.[16]
Augmented reality is currently being tested as a surgical simulation training tool for orthopedic surgeons.[17] Additionally, novel treatments, such as cementless total knee replacements, are being developed to improve postsurgical outcomes.[18]
Vertebral wedge fracture and "dowager's hump"
Vertebrae have features of both cortical and trabecular bones. The vertebral body's outer surface is composed of compact bone. Meanwhile, the inner portion contains thousands of trabeculae oriented in different directions. A "wedge fracture" occurs when the compact vertebral pedicles and processes remain intact while the inner trabecular segment gets damaged by a compressive force. Wedge fractures in the superior spine can lead to kyphosis, or the upper thorax's excessive bending, and a "dowager's hump" posterior to the cervical spine base.[19] A similar mechanism underlies vertebral wedge fractures of the lumbar vertebrae, resulting in distortion of the lumbar and thoracic curvatures.
Osteosarcoma
Osteosarcoma is a highly aggressive bone malignancy, the 3rd most common adolescent cancer after leukemia and lymphoma.[20] This condition has a bimodal age distribution globally, frequently affecting patients in the 2nd to 3rd and 7th to 8th decades of life.[21] Osteosarcoma involves malignant bone-forming primitive mesenchymal cells. Primary osteosarcoma most commonly affects the long bones, particularly the proximal humerus and tibia and distal femur. Symptoms include nighttime pain, reduced range of motion, and swelling of the nearby joints.[22]
Lung metastases and posttherapeutic recurrence are frequent in osteosarcoma cases. M2-like tumor-associated macrophages (TAMS) in the tumor stroma increase the risk of pulmonary metastasis and have a poor prognosis.[23][24][25] This condition requires multidisciplinary care. Treatment usually involves chemotherapy, surgery, and sometimes, radiation. Osteosarcoma's 5-year survival rate is 80%.
Dendritic cell immunotherapy is a novel intervention that uses the dendritic cells' immunomodulatory effects to eliminate cancer tissue.[26] Peptide vaccines, immune checkpoint inhibitors, genetically modified T cells, cytokines, immune modulators, and macrophage activators are other current and emerging immunotherapeutic options for osteosarcoma.[27] Percutaneous cryoablation shows promise for treating various malignant and benign bone and soft tissue tumors due to its flexibility, precision, and relatively safe profile. Research highlights its effectiveness in managing primary tumors, recurrent sarcomas, metastases, and benign lesions, indicating its potential as an alternative or adjunct to surgery with favorable outcomes and minimal adverse events.[28]
Other Issues
Other clinical issues that may arise within the skeletal system are the following:
- Infection: Osteomyelitis is a bacterial bone infection that can develop from inoculation or direct or hematogenous spread. Staphylococcus aureus is most often the causative agent.[29]
- Avascular necrosis: The condition occurs when the bone's blood supply is compromised. Necrosis may lead to nonunion. The femoral head, knee, humeral head, and talus are particularly susceptible to avascular necrosis.[30]
- Osteoporosis: This term refers to bone weakness due to loss of density. The condition is common in older patients, especially postmenopausal women.
- Vitamin D deficiency: Insufficiency of vitamin D levels can result in rickets in pediatric patients and osteomalacia in adults. Vitamin D is critical to calcium and phosphate metabolism. Osteoid will not mineralize properly without this prohormone. Bone weakening and pain are characteristic (see Image. Rickets).[31]
- Craniofacial malformations: These conditions arise from disordered neural crest cell migration.[32]
- Apophyseal fracture: An apophysis serves as the attachment site for muscles and tendons to the parent bone in young individuals. An ossification center separates the apophysis from the parent bone during normal development until skeletal maturity. This configuration renders the apophysis a relatively minor point of resistance compared to the tendons attached to it.[33]
Media
(Click Image to Enlarge)

Parts of a Long Bone. This illustration shows the articular cartilage, epiphyseal line, spongy bone (aka trabecular bone), medullary cavity, endosteum, periosteum, and periosteal arteries.
Contributed by Beckie Palmer
(Click Image to Enlarge)
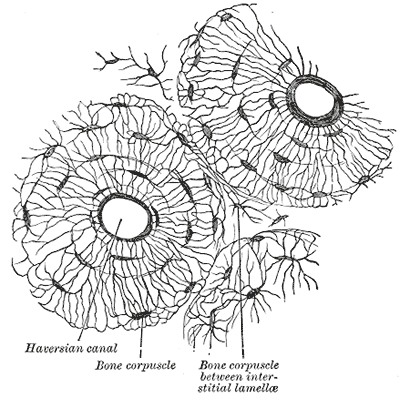
Osteon. Transverse section of the human fibula showing the osteon and its structures. The Haversian canal, osteocytes (bone corpuscles), and lamellae are shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
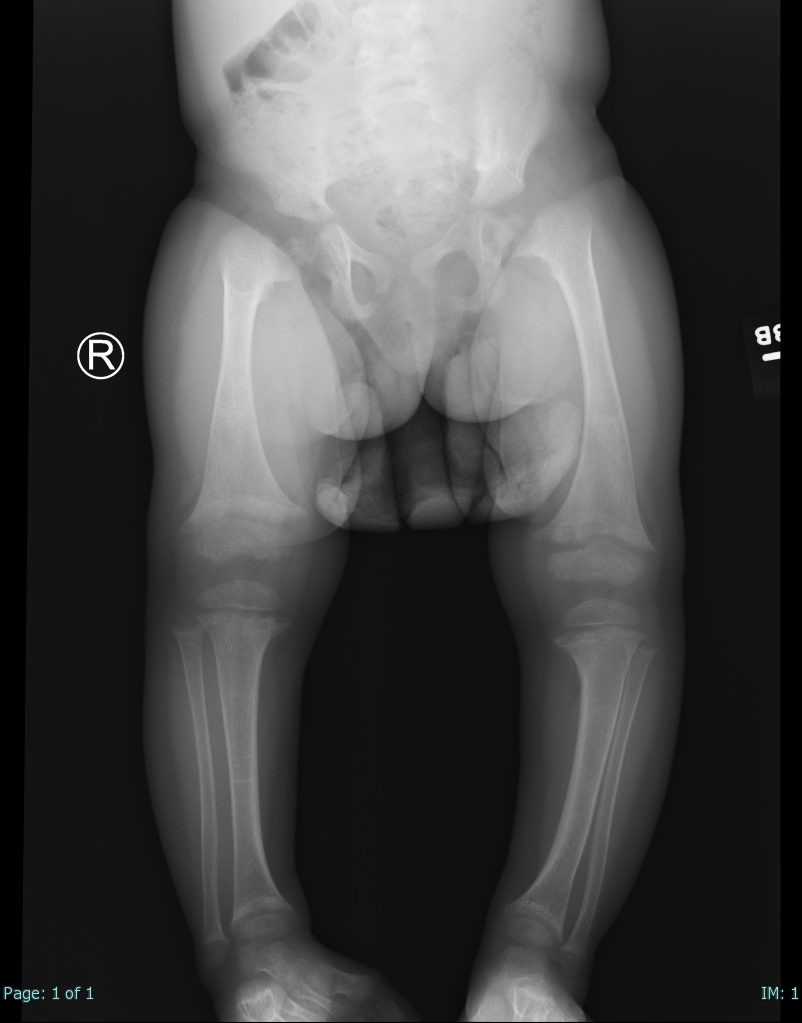
Rickets. Single AP view from a leg alignment study demonstrates metaphyseal flaring (widening) of the distal femurs and proximal and distal tibial metaphyses. Tibial-shaft inbowing is also evident in the X-ray of this 2-year-old female with a known history of rickets.
Contributed by Hassana Barazi, MD
References
Hong AR, Kim SW. Effects of Resistance Exercise on Bone Health. Endocrinology and metabolism (Seoul, Korea). 2018 Dec:33(4):435-444. doi: 10.3803/EnM.2018.33.4.435. Epub [PubMed PMID: 30513557]
El Sayed SA, Nezwek TA, Varacallo M. Physiology, Bone. StatPearls. 2024 Jan:(): [PubMed PMID: 28722997]
Burrow K , Young W , Carne A , McConnell M , Hammer N , Scholze M , Bekhit AE . Consumption of sheep milk compared to cow milk can affect trabecular bone ultrastructure in a rat model. Food & function. 2019 Jan 22:10(1):163-171. doi: 10.1039/c8fo01598h. Epub [PubMed PMID: 30516196]
Xue N,Ding X,Huang R,Jiang R,Huang H,Pan X,Min W,Chen J,Duan JA,Liu P,Wang Y, Bone Tissue Engineering in the Treatment of Bone Defects. Pharmaceuticals (Basel, Switzerland). 2022 Jul 17 [PubMed PMID: 35890177]
Augusto ACL, Goes PCK, Flores DV, Costa MAF, Takahashi MS, Rodrigues ACO, Padula LC, Gasparetto TD, Nogueira-Barbosa MH, Aihara AY. Imaging Review of Normal and Abnormal Skeletal Maturation. Radiographics : a review publication of the Radiological Society of North America, Inc. 2022 May-Jun:42(3):861-879. doi: 10.1148/rg.210088. Epub 2022 Feb 25 [PubMed PMID: 35213260]
Marahleh A, Kitaura H, Ohori F, Noguchi T, Mizoguchi I. The osteocyte and its osteoclastogenic potential. Frontiers in endocrinology. 2023:14():1121727. doi: 10.3389/fendo.2023.1121727. Epub 2023 May 24 [PubMed PMID: 37293482]
Grünewald TA, Johannes A, Wittig NK, Palle J, Rack A, Burghammer M, Birkedal H. Bone mineral properties and 3D orientation of human lamellar bone around cement lines and the Haversian system. IUCrJ. 2023 Mar 1:10(Pt 2):189-198. doi: 10.1107/S2052252523000866. Epub 2023 Mar 1 [PubMed PMID: 36786504]
Ono T, Hayashi M, Sasaki F, Nakashima T. RANKL biology: bone metabolism, the immune system, and beyond. Inflammation and regeneration. 2020:40():2. doi: 10.1186/s41232-019-0111-3. Epub 2020 Feb 7 [PubMed PMID: 32047573]
Da W, Tao L, Zhu Y. The Role of Osteoclast Energy Metabolism in the Occurrence and Development of Osteoporosis. Frontiers in endocrinology. 2021:12():675385. doi: 10.3389/fendo.2021.675385. Epub 2021 May 12 [PubMed PMID: 34054735]
Gavali S, Gupta MK, Daswani B, Wani MR, Sirdeshmukh R, Khatkhatay MI. Estrogen enhances human osteoblast survival and function via promotion of autophagy. Biochimica et biophysica acta. Molecular cell research. 2019 Sep:1866(9):1498-1507. doi: 10.1016/j.bbamcr.2019.06.014. Epub 2019 Jun 28 [PubMed PMID: 31255720]
Breeland G, Sinkler MA, Menezes RG. Embryology, Bone Ossification. StatPearls. 2024 Jan:(): [PubMed PMID: 30969540]
Chen J, Hendriks M, Chatzis A, Ramasamy SK, Kusumbe AP. Bone Vasculature and Bone Marrow Vascular Niches in Health and Disease. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 2020 Nov:35(11):2103-2120. doi: 10.1002/jbmr.4171. Epub 2020 Sep 23 [PubMed PMID: 32845550]
Brazill JM, Beeve AT, Craft CS, Ivanusic JJ, Scheller EL. Nerves in Bone: Evolving Concepts in Pain and Anabolism. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 2019 Aug:34(8):1393-1406. doi: 10.1002/jbmr.3822. Epub 2019 Jul 26 [PubMed PMID: 31247122]
Liu S, Liu S, Li S, Liang B, Han X, Liang Y, Wei X. Nerves within bone and their application in tissue engineering of bone regeneration. Frontiers in neurology. 2022:13():1085560. doi: 10.3389/fneur.2022.1085560. Epub 2023 Feb 2 [PubMed PMID: 36818724]
Levine RH, Thomas A, Nezwek TA, Waseem M. Salter-Harris Fracture. StatPearls. 2024 Jan:(): [PubMed PMID: 28613461]
Koenen L, Waseem M. Orbital Floor Fracture. StatPearls. 2025 Jan:(): [PubMed PMID: 30521246]
Condino S, Turini G, Parchi PD, Viglialoro RM, Piolanti N, Gesi M, Ferrari M, Ferrari V. How to Build a Patient-Specific Hybrid Simulator for Orthopaedic Open Surgery: Benefits and Limits of Mixed-Reality Using the Microsoft HoloLens. Journal of healthcare engineering. 2018:2018():5435097. doi: 10.1155/2018/5435097. Epub 2018 Nov 1 [PubMed PMID: 30515284]
Quevedo González FJ, Lipman JD, Lo D, De Martino I, Sculco PK, Sculco TP, Catani F, Wright TM. Mechanical performance of cementless total knee replacements: It is not all about the maximum loads. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2019 Feb:37(2):350-357. doi: 10.1002/jor.24194. Epub 2019 Jan 3 [PubMed PMID: 30499604]
Meeta M, Harinarayan CV, Marwah R, Sahay R, Kalra S, Babhulkar S. Clinical Practice Guidelines on Postmenopausal Osteoporosis: *An Executive Summary and Recommendations - Update 2019-2020. Journal of mid-life health. 2020 Apr-Jun:11(2):96-112. doi: 10.4103/jmh.JMH_143_20. Epub 2020 Aug 10 [PubMed PMID: 33281419]
Level 1 (high-level) evidenceJeys LM, Thorne CJ, Parry M, Gaston CL, Sumathi VP, Grimer JR. A Novel System for the Surgical Staging of Primary High-grade Osteosarcoma: The Birmingham Classification. Clinical orthopaedics and related research. 2017 Mar:475(3):842-850. doi: 10.1007/s11999-016-4851-y. Epub [PubMed PMID: 27138473]
Rojas GA, Hubbard AK, Diessner BJ, Ribeiro KB, Spector LG. International trends in incidence of osteosarcoma (1988-2012). International journal of cancer. 2021 Sep 1:149(5):1044-1053. doi: 10.1002/ijc.33673. Epub 2021 May 17 [PubMed PMID: 33963769]
Al-Chalabi MMM, Jamil I, Wan Sulaiman WA. Unusual Location of Bone Tumor Easily Misdiagnosed: Distal Radius Osteosarcoma Treated as Osteomyelitis. Cureus. 2021 Nov:13(11):e19905. doi: 10.7759/cureus.19905. Epub 2021 Nov 25 [PubMed PMID: 34976513]
Cersosimo F, Lonardi S, Bernardini G, Telfer B, Mandelli GE, Santucci A, Vermi W, Giurisato E. Tumor-Associated Macrophages in Osteosarcoma: From Mechanisms to Therapy. International journal of molecular sciences. 2020 Jul 23:21(15):. doi: 10.3390/ijms21155207. Epub 2020 Jul 23 [PubMed PMID: 32717819]
Pu Y, Ji Q. Tumor-Associated Macrophages Regulate PD-1/PD-L1 Immunosuppression. Frontiers in immunology. 2022:13():874589. doi: 10.3389/fimmu.2022.874589. Epub 2022 May 3 [PubMed PMID: 35592338]
Mao X, Xu J, Wang W, Liang C, Hua J, Liu J, Zhang B, Meng Q, Yu X, Shi S. Crosstalk between cancer-associated fibroblasts and immune cells in the tumor microenvironment: new findings and future perspectives. Molecular cancer. 2021 Oct 11:20(1):131. doi: 10.1186/s12943-021-01428-1. Epub 2021 Oct 11 [PubMed PMID: 34635121]
Level 3 (low-level) evidenceBarry KC, Hsu J, Broz ML, Cueto FJ, Binnewies M, Combes AJ, Nelson AE, Loo K, Kumar R, Rosenblum MD, Alvarado MD, Wolf DM, Bogunovic D, Bhardwaj N, Daud AI, Ha PK, Ryan WR, Pollack JL, Samad B, Asthana S, Chan V, Krummel MF. A natural killer-dendritic cell axis defines checkpoint therapy-responsive tumor microenvironments. Nature medicine. 2018 Aug:24(8):1178-1191. doi: 10.1038/s41591-018-0085-8. Epub 2018 Jun 25 [PubMed PMID: 29942093]
Miwa S, Shirai T, Yamamoto N, Hayashi K, Takeuchi A, Igarashi K, Tsuchiya H. Current and Emerging Targets in Immunotherapy for Osteosarcoma. Journal of oncology. 2019:2019():7035045. doi: 10.1155/2019/7035045. Epub 2019 Jan 1 [PubMed PMID: 30693030]
Papalexis N, Savarese LG, Peta G, Errani C, Tuzzato G, Spinnato P, Ponti F, Miceli M, Facchini G. The New Ice Age of Musculoskeletal Intervention: Role of Percutaneous Cryoablation in Bone and Soft Tissue Tumors. Current oncology (Toronto, Ont.). 2023 Jul 17:30(7):6744-6770. doi: 10.3390/curroncol30070495. Epub 2023 Jul 17 [PubMed PMID: 37504355]
Momodu II, Savaliya V. Osteomyelitis. StatPearls. 2024 Jan:(): [PubMed PMID: 30335283]
Matthews AH, Davis DD, Fish MJ, Stitson D. Avascular Necrosis. StatPearls. 2024 Jan:(): [PubMed PMID: 30725692]
Dahash BA, Sankararaman S. Rickets. StatPearls. 2024 Jan:(): [PubMed PMID: 32965956]
Siismets EM, Hatch NE. Cranial Neural Crest Cells and Their Role in the Pathogenesis of Craniofacial Anomalies and Coronal Craniosynostosis. Journal of developmental biology. 2020 Sep 9:8(3):. doi: 10.3390/jdb8030018. Epub 2020 Sep 9 [PubMed PMID: 32916911]
Losco M, Ceglia MJ, Lazzarini F, De Biase P, Buzzi R. A rare case of avulsion fracture of the iliac crest apophysis in a young female athlete. Trauma case reports. 2019 Dec:24():100257. doi: 10.1016/j.tcr.2019.100257. Epub 2019 Nov 7 [PubMed PMID: 31737774]
Level 3 (low-level) evidence