Introduction
Sacroiliitis is an inflammation of the sacroiliac joint (SI), usually resulting in pain. Often it is a diagnosis of exclusion. The sacroiliac joint (SI) is one of the largest joints in the body and is a common source of the buttock and lower back pain. It connects the bones of the ilium to the sacrum. Sacroiliitis can be particularly difficult to diagnose because its symptoms are similar to many other common sources of back pain. It often is overlooked as a source of back or buttock pain. Pain from this condition often is due to chronic degenerative causes yet relatively uncommon. Sacroiliitis can be secondary to rheumatic, infectious, drug-related, or oncologic sources. Some specific examples of non-degenerative conditions that can lead to sacroiliitis are ankylosing spondylitis, psoriatic arthropathy, Bechet disease, hyperparathyroidism, and various pyogenic sources. [1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Various conditions result in the inflammation of the SI joint, leading to significant pain. Osteoarthritis can cause degeneration of the joint resulting in pathologic articulation and motion leading to this condition. Spondyloarthropathies themselves can cause significant inflammation of the joint itself. Pregnancy is another cause of the inflammation due to the hormone relaxin leading to the relaxation, stretching, and possible widening of the SI joint(s). The increased weight of pregnancy also causes extra mechanical stress on the joint, leading to further wear and tear. Trauma can cause direct or indirect stress and damage to the SI joint. Pyogenic sacroiliitis is the most frequently reported cause of acute sacroiliitis. Pain can originate from the synovial joint but can also originate from the posterior sacral ligaments.[4][5]
Epidemiology
Reports on the prevalence of sacroiliac pain vary widely. Some studies report the prevalence as 10% to 25% of those with lower back pain. In those with a confirmed diagnosis, the presentation of pain was ipsilateral buttock (94% cases) and midline lower lumbar area (74%). As mentioned previously the presentation can vary. Up to 50% of cases have radiation to the lower extremity: 6% to the upper lumbar area, 4% percent to the groin, and 2% percent to the lower abdomen.[6][7]
Pathophysiology
The sacrum articulates with the ilium, which helps to distribute body weight to the pelvis. The SI joint capsule is relatively thin and often develops defects that enable fluid, such as joint effusion or pus, to leak out onto the surrounding structures. As surrounding muscles and structures are affected different presentations of pain can present because different nerve roots innervate these structures. Common distributions of pain are L4-L5 dermatomes, but distributions can certainly present in dermatomes as high as L2 and as low as S3. The asymmetric motion of the pelvis can cause mechanical dysfunction, leading to degeneration and significant pain. Differential diagnosis includes leg-length discrepancies, unilateral weaker limb or gluteal muscles, tight or strained surrounding muscles structures, or hip osteoarthritis.[8]
Histopathology
Common degenerative findings show destruction and fibrosis of the cartilage and disruption, erosion, and ossification of sub-chondral bone. Synovitis also is commonly found which reveals hyperplasia of linings cells with infiltration of inflammatory cells. Degenerative enthesitis similarly reveals inflammatory cells. Infectious etiologies of sacroiliitis reveal lymphocytes, plasma cells, and fibrosis. Notably, some patients will show no histopathologic changes.
History and Physical
Sacroiliitis commonly presents as lower back pain. The pain presentation varies greatly, and patients could describe pain in one or both buttocks, hip pain, thigh pain, or even pain more distal. Patients may report that their pain is worse after sitting for prolonged periods or with rotational movements. Characterization of pain also varies widely and is commonly described as sharp and stabbing but can also be described as dull and achy. It is very important to ascertain more than just the timing and descriptions of the pain. Ask about a history of inflammatory disorders as discussed previously. Also, obtain a thorough review of systems to evaluate for systemic symptoms such as fevers, chills, night sweats, and weight loss. These symptoms are indicative of a more serious process indicating likely systemic illness.
Although not always obvious, inspection can reveal pelvic asymmetry. Measurement of the limbs can rule out a leg-length discrepancy. Inspect the spine for any abnormal curvatures or rotational abnormalities. Typically the range of motion, neurologic, and strength testing are unremarkable although the patient may experience pain during some of these tests.
Special provocative tests can be very helpful in reproducing the patient’s pain:
- “Fortin finger sign”- reproduction of pain after applying a deep palpation with the four-hand fingers posteriorly at the patient's SI joint(s).
- FABER test- reproduction of pain after flexing the hip while also abducting and externally rotating the hip.
- Sacral distraction test- reproduction of pain after applying pressure to the anterior superior iliac spine.
- Iliac compression test- reproduction of pain after applying pressure downward on the superior aspect of the iliac crest.
- Gaenslen test- reproduction of pain after having the patient flex the hip on the unaffected side and then dangle the affected leg off the examining table. Pressure is then directed downward on the leg to extend further the hip, which causes stress on the SI joint.
- Thigh thrust test- reproduction of pain after flexing the hip and applying a posterior shearing force to the SI joint.
- Sacral thrust test- reproduction of pain with the patient prone and then applying an anterior pressure through the sacrum.
The likelihood of SI joint mediated pain increases as the number of positive-provocative tests increase.
Evaluation
As discussed previously, various inflammatory conditions may cause or contribute to SI joint pain. If an inflammatory condition is suspected, consider ordering complete blood cell count, erythrocyte sedimentation rate, C-reactive protein, antinuclear antibody, human leukocyte antigen (HLA-B27), and rheumatoid factor. Although cancer is a far less common cause of sacroiliitis, if a cancerous process is suspected, consider ordering labs to assess for malignancy. [9][10]
In most clinical evaluations, common laboratory findings in the aseptic setting include:
- WBC count - usually normal (elevated in infection/septic presentation)
- ESR - elevated
- CRP - elevated
- HLA-B27 - About 50% to 92%% of patients with ankylosing spondylitis will be HLA-B27 positive
- Rheumatoid Factor (RF) - Negative in the setting of true ankylosing spondylitis
If trauma or inflammatory causes are not suspected, then radiographs are typically not needed, as there is usually no correlation between pain and radiographic images. If radiographs are performed an anteroposterior view of the pelvis/lumbar spine should be ordered. These images can show sclerosis or other degenerative changes of the SI joint. Specific sacroiliac views also can be taken at a 25 to 30-degree angle to help delineate widening or sclerotic changes at joint margins. CT scan also can show sclerotic changes and reveal reactive spurring or subluxation. The previously noted imaging findings are usually later changes. MRI may show subchondral edema, which is the earliest sign of sacroiliitis. PET scans can be ordered to evaluate for bony metastatic disease.
The most informative test for the diagnosis of sacroiliitis is SI joint injection with local anesthetics and steroids. If this procedure relieves the pain, it is likely that the inflammation at this site was the cause of the pain. Potentially, a single injection or series of injections can completely treat the pain. If the injection provided a very significant amount of pain relief, even if for a short period, then the chronic pain can likely be attributed to the SI joint. In such cases, a surgical intervention should be considered as the injections were able to localize the pain to the SI joint(s). No more than three injections should occur over a year.
Treatment / Management
Physical therapy can be very helpful if the pain is due to hypermobility. Therapy can help to stabilize and strengthen lumbopelvic musculature. If the pain is due to immobility, then physical therapy can help increase mobilization of the SI joint. NSAIDs and muscle relaxants can be prescribed during the acute phase of presentations. These are less effective as cases become more chronic. Real-time image-guided intra-articular anesthetic/steroid injections can be performed for diagnostic and therapeutic effect. If the previous treatments do not provide adequate relief, then some providers will consider radiofrequency ablation. Usually, surgery is reserved as a last resort for patients with chronic pain. In such cases, one can consider SI joint fusion with SI screws.[11][12][13]
Differential Diagnosis
- Ankylosing spondylitis
- Hip tendonitis/fracture
- Piriformis syndrome
- Sacroiliac joint infection
- Trochanteric bursitis
Complications
- Chronic back and hip pain
- Muscle wasting
Pearls and Other Issues
Aseptic sacroiliitis
Alternative treatment options include ultrasound-guided prolotherapy, which is an injection of saline and glucose directed to the SI joint. It is theorized that this procedure is pro-inflammatory and results in increased healing, scarring, and tightening of the SI ligaments. SI joint belts can be provided in conjunction with various therapies, and theoretically, they function to stabilize the gluteal muscles and support the SI joint. If the leg-length discrepancy is thought to be a major contributor, then orthotics and/or shoe lifts can be considered.
Surgical indications
- Surgery is indicated after nonoperative modalities are first attempted and exhausted
- Most cases (aseptic) are self-limiting and improve with rest, activity modification, and NSAIDs
- In the case of aggressive recalcitrant symptoms or infection, especially in the setting of a documented abscess, surgery is performed earlier in the course of treatment
Special considerations
- Nonoperative management is the first line of treatment in the setting of pregnancy. Current evidence suggests a high likelihood of symptom resolution after childbirth
- Sacroiliitis in the setting of a larger spondylopathy, management begins with more aggressive PT modalities, NSAIDs and TNF alpha inhibitors
Septic sacroiliitis
- In the setting of high index of clinical suspicion, exam, and laboratory results (including leukocytosis), initial management with broad-spectrum IV antibiotics, followed by culture-specific, and eventually a course of PO antibiotics
- Transitioning from broad-spectrum antibiotics to culture-specific can occur after an adequate sample is aspirated and/or biopsied using either interventional radiology and/or a surgical service if the aforementioned procedure fails. In general, an open approach for SI joint debridement and biopsy has more associated morbidity compared to the minimally invasive aspiration techniques.
Enhancing Healthcare Team Outcomes
Sacroiliitis is best managed by an interprofessional team that consists of a physical therapist, physician rheumatologist, and dietitian. Patient education is the key to good outcomes. All patients should be informed that the condition is benign and will improve with conservative measures. The patient should be encouraged to participate in a regular exercise program, lose weight and eat healthily. Home exercises can help prevent deconditioning. The patient should also be asked to quit smoking and abstain from alcohol. There is ample evidence indicating that patients who remain physically active have an excellent quality of life. [14][11](Level V)
Outcomes
The majority of patients with sacroiliitis have an excellent outcome. However, the recovery may take 2-4weeks. Recurrences are common if patients do not change their lifestyle. Some series report a recurrence rate of over 30%.[15][16] (Level V)
Media
(Click Image to Enlarge)
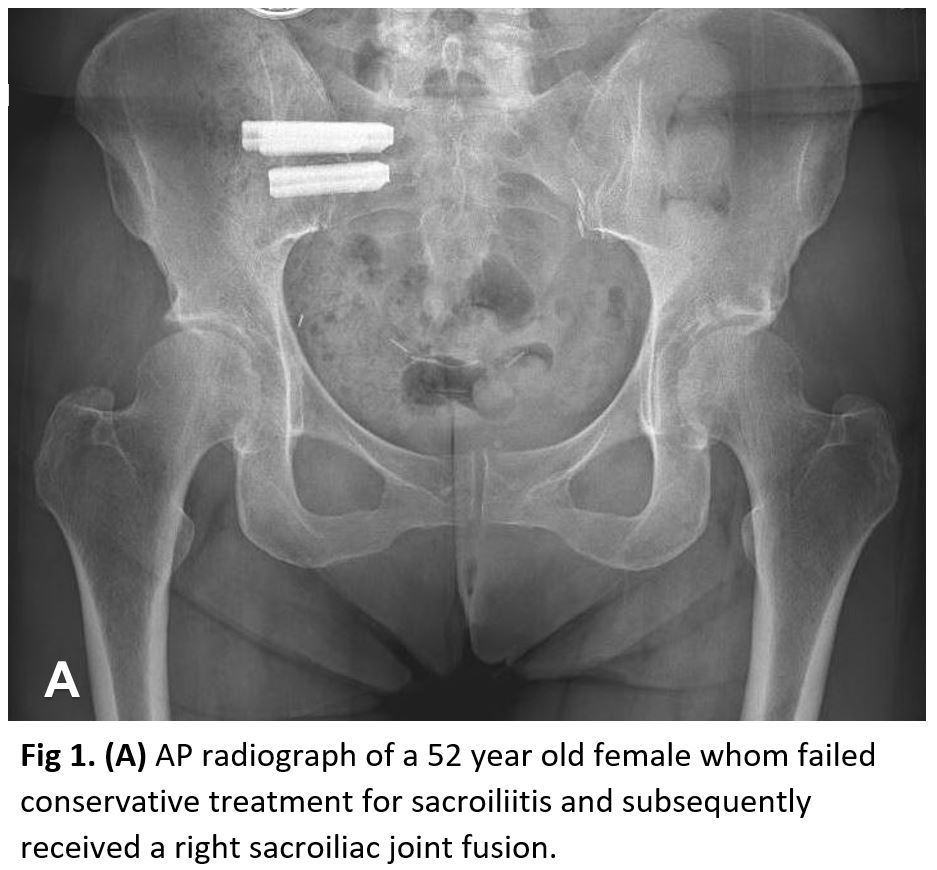
Anteroposterior Radiograph, Sacroiliitis, Right Sacroiliac Joint Fusion Contributed by StatPearls
References
Slobodin G, Hussein H, Rosner I, Eshed I. Sacroiliitis - early diagnosis is key. Journal of inflammation research. 2018:11():339-344. doi: 10.2147/JIR.S149494. Epub 2018 Sep 10 [PubMed PMID: 30237730]
Chahal BS, Kwan ALC, Dhillon SS, Olubaniyi BO, Jhiangri GS, Neilson MM, Lambert RGW. Radiation Exposure to the Sacroiliac Joint From Low-Dose CT Compared With Radiography. AJR. American journal of roentgenology. 2018 Nov:211(5):1058-1062. doi: 10.2214/AJR.18.19678. Epub 2018 Sep 12 [PubMed PMID: 30207791]
Gutierrez M, Rodriguez S, Soto-Fajardo C, Santos-Moreno P, Sandoval H, Bertolazzi C, Pineda C. Ultrasound of sacroiliac joints in spondyloarthritis: a systematic review. Rheumatology international. 2018 Oct:38(10):1791-1805. doi: 10.1007/s00296-018-4126-x. Epub 2018 Aug 11 [PubMed PMID: 30099591]
Level 1 (high-level) evidenceKocak O, Kocak AY, Sanal B, Kulan G. Bilateral Sacroiliitis Confirmed with Magnetic Resonance Imaging during Isotretinoin Treatment: Assessment of 11 Patients and a Review of the Literature. Acta dermatovenerologica Croatica : ADC. 2017 Oct:25(3):228-233 [PubMed PMID: 29252176]
Pandita A, Madhuripan N, Hurtado RM, Dhamoon A. Back pain and oedematous Schmorl node: a diagnostic dilemma. BMJ case reports. 2017 May 22:2017():. pii: bcr-2017-219904. doi: 10.1136/bcr-2017-219904. Epub 2017 May 22 [PubMed PMID: 28536227]
Level 3 (low-level) evidenceProtopopov M, Poddubnyy D. Radiographic progression in non-radiographic axial spondyloarthritis. Expert review of clinical immunology. 2018 Jun:14(6):525-533. doi: 10.1080/1744666X.2018.1477591. Epub 2018 May 24 [PubMed PMID: 29774755]
Ziade NR. HLA B27 antigen in Middle Eastern and Arab countries: systematic review of the strength of association with axial spondyloarthritis and methodological gaps. BMC musculoskeletal disorders. 2017 Jun 29:18(1):280. doi: 10.1186/s12891-017-1639-5. Epub 2017 Jun 29 [PubMed PMID: 28662723]
Level 1 (high-level) evidencePoddubnyy D, Listing J, Haibel H, Knüppel S, Rudwaleit M, Sieper J. Functional relevance of radiographic spinal progression in axial spondyloarthritis: results from the GErman SPondyloarthritis Inception Cohort. Rheumatology (Oxford, England). 2018 Apr 1:57(4):703-711. doi: 10.1093/rheumatology/kex475. Epub [PubMed PMID: 29373733]
Tan S, Ward MM. Computed tomography in axial spondyloarthritis. Current opinion in rheumatology. 2018 Jul:30(4):334-339. doi: 10.1097/BOR.0000000000000507. Epub [PubMed PMID: 29538011]
Level 3 (low-level) evidenceŽlnay M. [The role of magnetic resonance imaging in diagnostics of axial spondyloarthritis]. Vnitrni lekarstvi. 2018 Spring:64(2):117-126 [PubMed PMID: 29595277]
Expert Panel on Musculoskeletal Imaging:, Bernard SA, Kransdorf MJ, Beaman FD, Adler RS, Amini B, Appel M, Arnold E, Cassidy RC, Greenspan BS, Lee KS, Tuite MJ, Walker EA, Ward RJ, Wessell DE, Weissman BN. ACR Appropriateness Criteria(®) Chronic Back Pain Suspected Sacroiliitis-Spondyloarthropathy. Journal of the American College of Radiology : JACR. 2017 May:14(5S):S62-S70. doi: 10.1016/j.jacr.2017.01.048. Epub [PubMed PMID: 28473095]
Nash P, Lubrano E, Cauli A, Taylor WJ, Olivieri I, Gladman DD. Updated guidelines for the management of axial disease in psoriatic arthritis. The Journal of rheumatology. 2014 Nov:41(11):2286-9. doi: 10.3899/jrheum.140877. Epub [PubMed PMID: 25362712]
van der Heijde D, Ramiro S, Landewé R, Baraliakos X, Van den Bosch F, Sepriano A, Regel A, Ciurea A, Dagfinrud H, Dougados M, van Gaalen F, Géher P, van der Horst-Bruinsma I, Inman RD, Jongkees M, Kiltz U, Kvien TK, Machado PM, Marzo-Ortega H, Molto A, Navarro-Compàn V, Ozgocmen S, Pimentel-Santos FM, Reveille J, Rudwaleit M, Sieper J, Sampaio-Barros P, Wiek D, Braun J. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Annals of the rheumatic diseases. 2017 Jun:76(6):978-991. doi: 10.1136/annrheumdis-2016-210770. Epub 2017 Jan 13 [PubMed PMID: 28087505]
Nelson AM, Nagpal G. Interventional Approaches to Low Back Pain. Clinical spine surgery. 2018 Jun:31(5):188-196. doi: 10.1097/BSD.0000000000000542. Epub [PubMed PMID: 28486278]
Darr E, Meyer SC, Whang PG, Kovalsky D, Frank C, Lockstadt H, Limoni R, Redmond A, Ploska P, Oh MY, Cher D, Chowdhary A. Long-term prospective outcomes after minimally invasive trans-iliac sacroiliac joint fusion using triangular titanium implants. Medical devices (Auckland, N.Z.). 2018:11():113-121. doi: 10.2147/MDER.S160989. Epub 2018 Apr 9 [PubMed PMID: 29674852]
van Lunteren M, Ez-Zaitouni Z, de Koning A, Dagfinrud H, Ramonda R, Jacobsson L, Landewé R, van der Heijde D, van Gaalen FA. In Early Axial Spondyloarthritis, Increasing Disease Activity Is Associated with Worsening of Health-related Quality of Life over Time. The Journal of rheumatology. 2018 Jun:45(6):779-784. doi: 10.3899/jrheum.170796. Epub 2018 Mar 15 [PubMed PMID: 29545448]
Level 2 (mid-level) evidence